
Abstract
The World Organization of Family Doctors (WONCA) developed the third edition of the International Classification of Primary Care (ICPC-3) to support the shift from a medical perspective to a person-centered perspective in primary health care. The previous editions (ICPC-1 and ICPC-2) allowed description of 3 important elements of health care encounters: the reason for the encounter, the diagnosis and/or health problem, and the process of care. The ICPC-3 adds function-related information as a fourth element, thereby capturing most parts of the encounter in a single practical and concise classification. ICPC-3 thus has the potential to give more insight on patients’ activities and functioning, supporting physicians in shifting from a strict medical/disease-based approach to care to a more person-centered approach. The ICPC-3 is also expanded with a new chapter for visits pertaining to immunizations and for coding of special screening examinations and public health promotion; in addition, it contains classes for programs related to reported conditions (eg, a cardiovascular program, a heart failure program) and can accommodate relevant national or regional classes. Classes are selected based on what is truly and frequently occurring in daily practice. Each class has its own codes. Less frequently used concepts pertaining to morbidity are captured as inclusions within the main classes. Implementation of the ICPC-3 in an electronic health record allows provision of meaningful feedback to primary care, and supports the exchange of information within teams and between primary and secondary care. It also gives policy makers and funders insight into what is happening in primary care and thus has the potential to improve provision of care.
- ICPC-3
- classification
- primary care
- health data
- patient-centered care
- functioning
- prevention
- health programs
- medical informatics
- population health
INTRODUCTION
For a long time, family physicians have been recording routine clinical data in health records. Use of these primary care data for clinical decision support, quality assessment, research, and policy purposes requires that they be available in a structured form. In 1987, the World Organization of Family Doctors (WONCA) developed and published the first edition of the International Classification of Primary Care (ICPC-1).1 This classification allowed coding of 3 important elements of health care encounters: the reason for the encounter, the diagnosis and/or health problem, and the process of care. Before publication of this new classification, data regarding morbidity collected in primary care research were coded using the International Classification of Diseases (ICD).2 The ICD is designed for mortality and hospital statistics, however, so it lacks codes for many symptoms and nondisease conditions encountered in primary care.
The second edition of the ICPC (ICPC-2)3 not only brought the ICPC classification in line with the ICD-10 (published in 1992),4 but also added inclusion criteria for and cross-references among classes in the classification. The ICPC-2 has been translated into 22 languages and is accepted by the World Health Organization as a member of the Family of International Classifications. It is the standard classification used by family physicians in the Netherlands, Norway, Denmark, Belgium, Ukraine, and Portugal; in addition, several other countries (Australia, Brazil, Poland, France, Finland, Japan, Morocco, and Malta) have used it in studies of health care encounters.5-8 Use of the ICPC is hampered by many countries’ requirement that morbidity be reported with ICD, even though that classification is not adequate for primary care. Additional limitations include the lack of a corresponding data model in the electronic health record (EHR) as well as the mediocre search systems available to find the correct code.9
The most important application of the ICPC is in the coding episodes of care.10 An episode of care is characterized by a discrete disease, health problem, or preventive need, and covers all care provided to a patient starting with the first presentation to a health care professional and ending with the last interaction for that health problem or disease. An episode of care consists of 1 or more encounters, each with its own reason for the encounter11,12 and diagnoses and interventions, and documents changes in the relations between encounters over time. It allows episode epidemiology, whereby clinicians and others can better understand why patients do and do not get better, what works for which patient, and which interventions were provided for patients and when, over time. This picture enables discovery of what happens to patients with symptoms (vs diagnoses) and the predictive value of symptoms for diseases, research that can be done only using primary care data because in most countries, patients must see primary care clinicians before seeing specialists.13,14
As recognized by WONCA, the coding of primary care content should reflect the core values of the field with an emphasis on improving the user experience and health of people. The focus in family medicine is changing from a medical/disease-based perspective to a more person-centered perspective, which means that greater emphasis is placed on prevention, functioning, patient preferences, and meaningful outcomes. To help meet these new objectives, the WONCA ICPC-3 Consortium developed the ICPC-3 (https://icpc-3.info), which became publicly available in December 2020 and was formally endorsed by WONCA in April 2021.
At the same time, 40 years after health experts and world leaders drafted the Declaration of Alma-Ata, the Declaration of Astana restated the importance of primary health care15,16 for person-centered care and for provision of preventive care by interprofessional teams.17 A systematic review has shown that primary care–based health systems, with their emphasis on person-centered care, contribute to better population health.18 This finding has driven health reforms that will strengthen the role of primary care. Successful health care transformation requires real-life data with an emphasis on primary care. The ICPC-3 enables coding of much of this information in a practical way.
PURPOSE
In this article, we introduce the ICPC-3 and advocate for its use in all primary care settings. Our aim is to show that implementing this classification in an episode of care structure is a promising way to understand factors related to treatment success and failure. We also describe information that can now be coded with the third edition that could not be coded with the previous editions. Finally, we show the potential benefits of integrating the ICPC-3 in the primary care EHR by presenting a clinical case.
NEW FEATURES
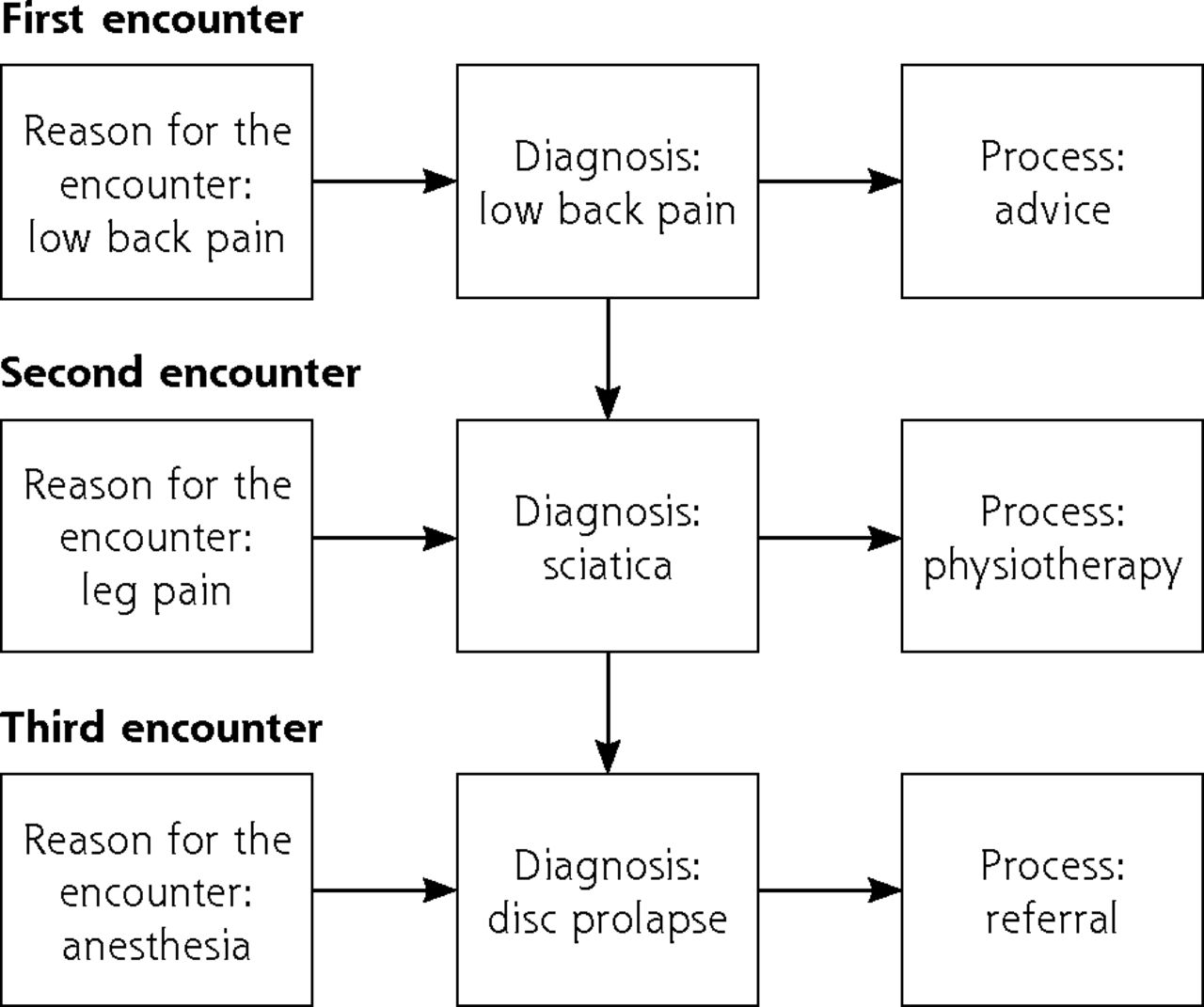
The ICPC-3 addresses several missing or limited aspects of clinical encounters in the previous editions. We discuss important new features below. A comparison of coding for an episode of care spanning several encounters in a patient with low back pain with the ICPC-1 and ICPC-2 (Figure 1) vs the ICPC-3 (Figure 2) illustrates the enhanced clinical picture provided by the latter.
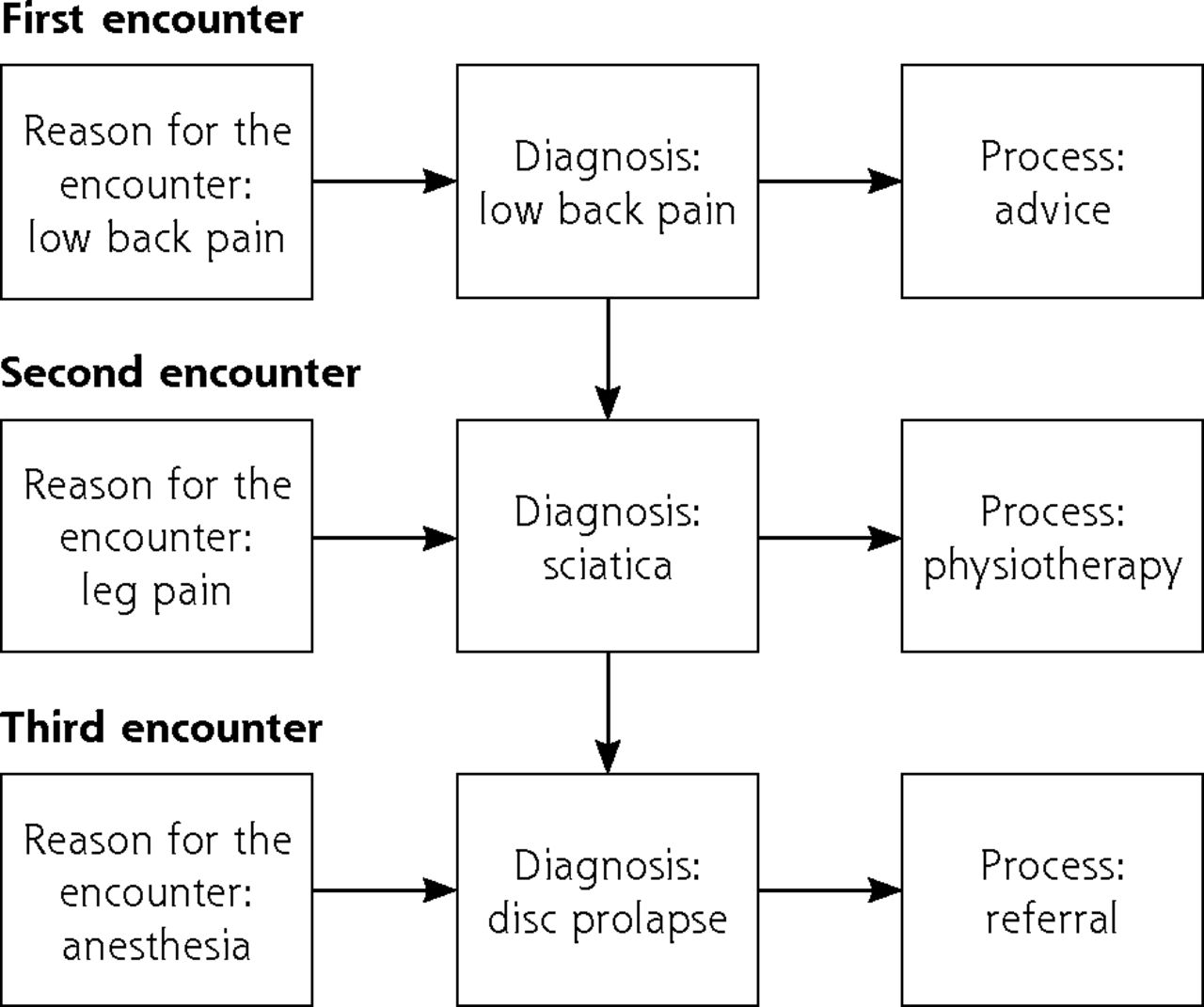
An episode of care in ICPC-1 and ICPC-2.
ICPC-1 = International Classification of Primary Care, First Edition; ICPC-2 = International Classification of Primary Care, Second Edition.
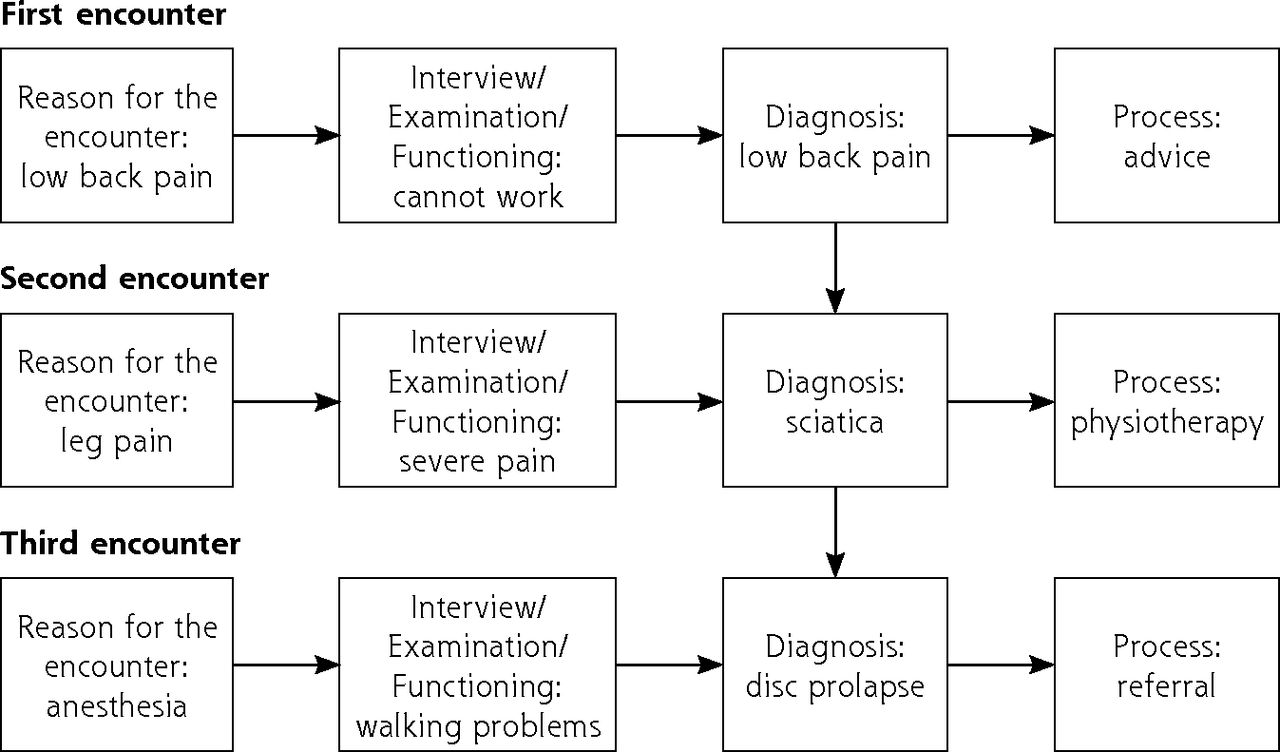
An episode of care in ICPC-3.
ICPC-3 = International Classification of Primary Care, Third Edition.
Capture of Person-Centered Data
The ICPC-2 does not permit coding of activities (and limitations in activities) and participation (and restrictions in participation), patient treatment preferences, and environmental factors and personality traits that influence health. The proposed solution was to introduce function-related rubrics as an integral part of the ICPC-3. These rubrics can be used to indicate patients’ functional status and can capture patients’ input, for example, if a patient expresses a severe limitation in an activity or a barrier to participation. The rubrics also importantly provide an impression of the outcome of clinical interventions. In addition, the ICPC-3 allows coding of the wish to receive or decline specific treatments or care (eg, preferences regarding vaccination, screening, antibiotic treatment, and end of life care).
More Granularity for Certain Visits
The ICPC-3 provides more granularity for certain types of visits: those for general and routine examinations, family planning, prevention, and other reasons. The rubrics in the nondisease part of the classification, for example, in the organ/system chapters, were developed to better define an episode of care. For visits pertaining to prevention, the ICPC-2 offers only 1 class, whereas the ICPC-3 offers 35 classes.
Ability to Code Common Regional Conditions
The ICPC-3 includes extensions for regional and national conditions; therefore, the modified national modules required in the ICPC-1 and ICPC-2 are no longer needed. Currently, the regional extensions comprise diseases and symptoms from the Global Burden of Disease19 list, and diseases and symptoms prevalent in the African, European, and South American regions.
COMPREHENSIVE DATA
The ICPC-3 captures more comprehensive data than previous editions, although some data still cannot be captured. Case descriptions often contain personal characteristics and environmental factors: sociodemographic variables such as age, sex, occupation, cultural background, and family status. Some of this context can be documented unrelated to the reason for an encounter, for instance, by using the Primary Care Functioning Scale.20 This questionnaire on functioning in daily life has been validated for patients older than 50 years with multimorbidity, and contains items that are part of the ICPC-3. If functioning is determined to play a role in the context of a reason for the encounter, it can then be coded with the ICPC-3 during the encounter. These classes become meaningful when paired with the scale values. For example, rotator cuff syndrome is an inclusion of shoulder syndrome, and the scale values for pain add a measure of severity.
ILLUSTRATIVE CLINICAL CASE
A specific clinical case with 3 episodes of care in a single encounter helps illustrate the expanded capability offered by the ICPC-3. In the case description below, summarized in Table 1 with the ICPC coding framework, italicized text denotes information that can now be coded with the ICPC-3 that could not be coded with the previous editions.
Coding of 3 Episodes of Care in a Single Encounter
Mrs Rodriguez is 53 years old and lives near Sao Paulo, Brazil. She visits the primary health center and reports that she has a fever, headache, and joint pain since yesterday. She thinks she has dengue fever as there are a lot of people with dengue in her neighborhood.
History and examination by the nurse shows the patient’s blood pressure is 120/80 mm Hg, and she is well hydrated and has no other serious symptoms. The tourniquet test is negative. The patient reports that she is unable to work. After examining the patient, the family physician decides to treat her for an almost certain dengue infection, with a prescription for acetaminophen and advice to come back if she notices any signs of worsening.
The patient also mentions an unpleasant sensation in her right eye after sleeping with her contact lenses in at night, and she believes that something has been left behind. On physical examination and fluorescein examination of the eye, no abnormalities are found. Her vision is normal. The diagnosis is burning eyes. The patient is advised to wait for the symptoms to resolve, as the physician expects resolution within 2 days.
Mrs Rodriguez’s other reason for visiting the primary health center is to get a flu shot. The injection is not administered because she has a fever. She is advised to return after 2 weeks and resolution of her fever to receive the vaccine. This episode is an encounter for immunization against influenza.
This example demonstrates that the most important encounter information can be correctly captured and coded by using the ICPC-3. This edition still lacks labels and codes for physical findings; in future development, we plan to expand it to capture this information.
PERSPECTIVES
The ICPC-3 was developed with all primary care clinicians in mind and is not limited to family physicians or general practitioners. This classification therefore makes it easier to connect to other disciplines using the same classification. A full picture of a patient is necessary for goal-oriented primary care, so we recommend implementing all components of the ICPC-3. Comprehensive patient data will also be required for evaluating policies on every level: patient, practice, and population.
The ICPC-3 is interoperable with classifications such as the ICD-10 and ICD-11, the International Classification of Health Interventions (ICHI),21 and the International Classification of Functioning, Disability and Health (ICF),22 as well as with clinical terminology classifications such as the Systematized Nomenclature of Medicine – Clinical Terms (SNOMED CT).23 At the same time, the ICPC-3 remains backward compatible with previous editions of the classification. Its optimal use is in an EHR on a desktop computer, laptop, tablet, or mobile telephone.
Structuring of EHR data offers the opportunity to connect person-centered episodes of care with clinical pathways and expert systems (eg, linking diagnoses to a prescription system). Construction of clinical pathways requires information about episodes of care, diagnoses, and procedures; details of the care input data (eg, when and by whom data were entered, along with the entries); and information about clinical findings and observational data, as well as an understanding of relations among these various elements. Data on functioning support this understanding. Furthermore, a patient- and goal-oriented team approach is key for diagnostic and therapeutic decision making. By compiling coded data in episodes of care, the ICPC-3 offers a way of logically organizing and thinking about primary care in a single classification.
Footnotes
Conflicts of interest: authors report none.
- Received for publication August 5, 2021.
- Revision received January 7, 2022.
- Accepted for publication January 12, 2022.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}