
Article Figures & Data
Figures
- Figure 1.
Dutch CRC screening protocol.
CRC = colorectal cancer; FIT = fecal immunochemical test.
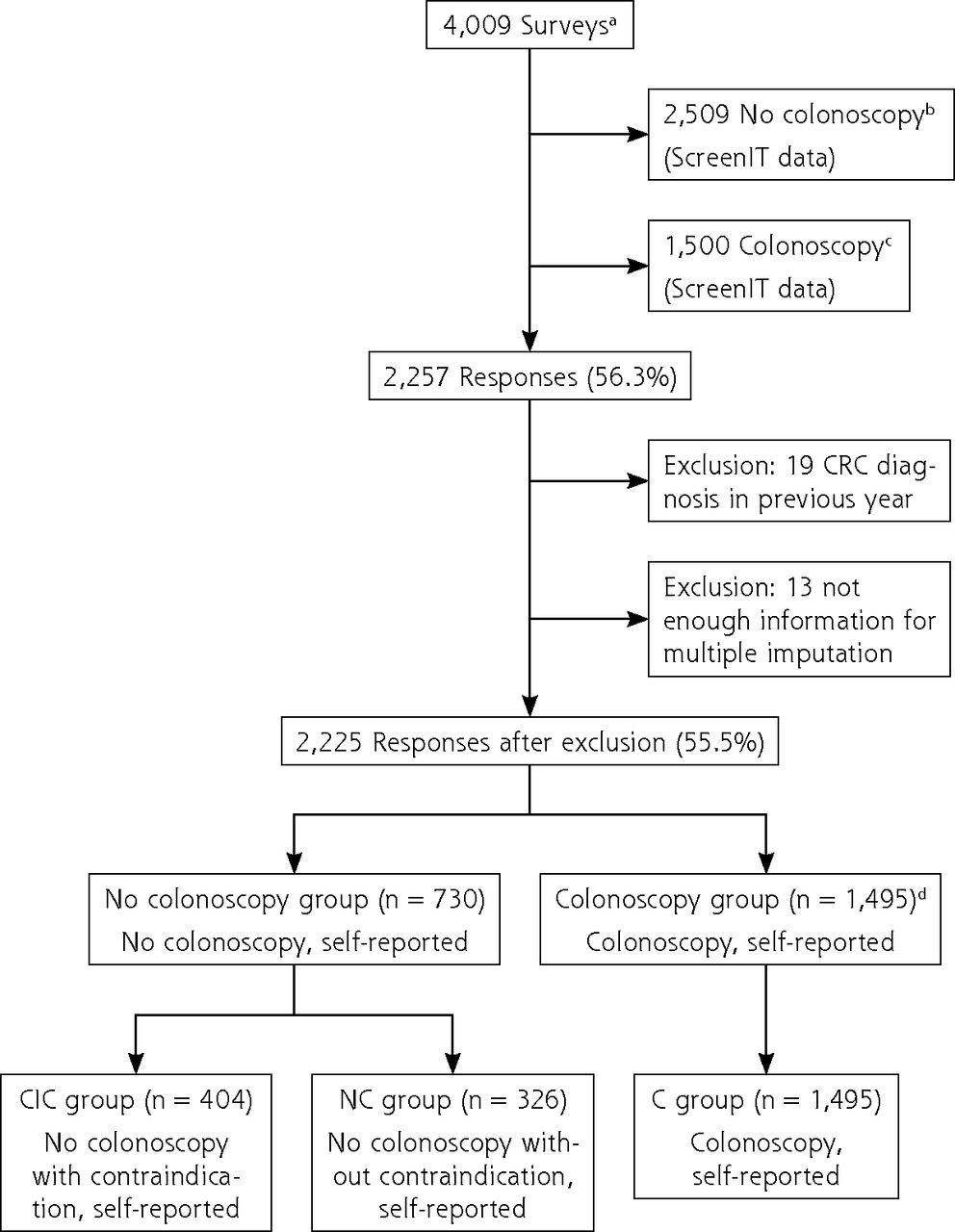
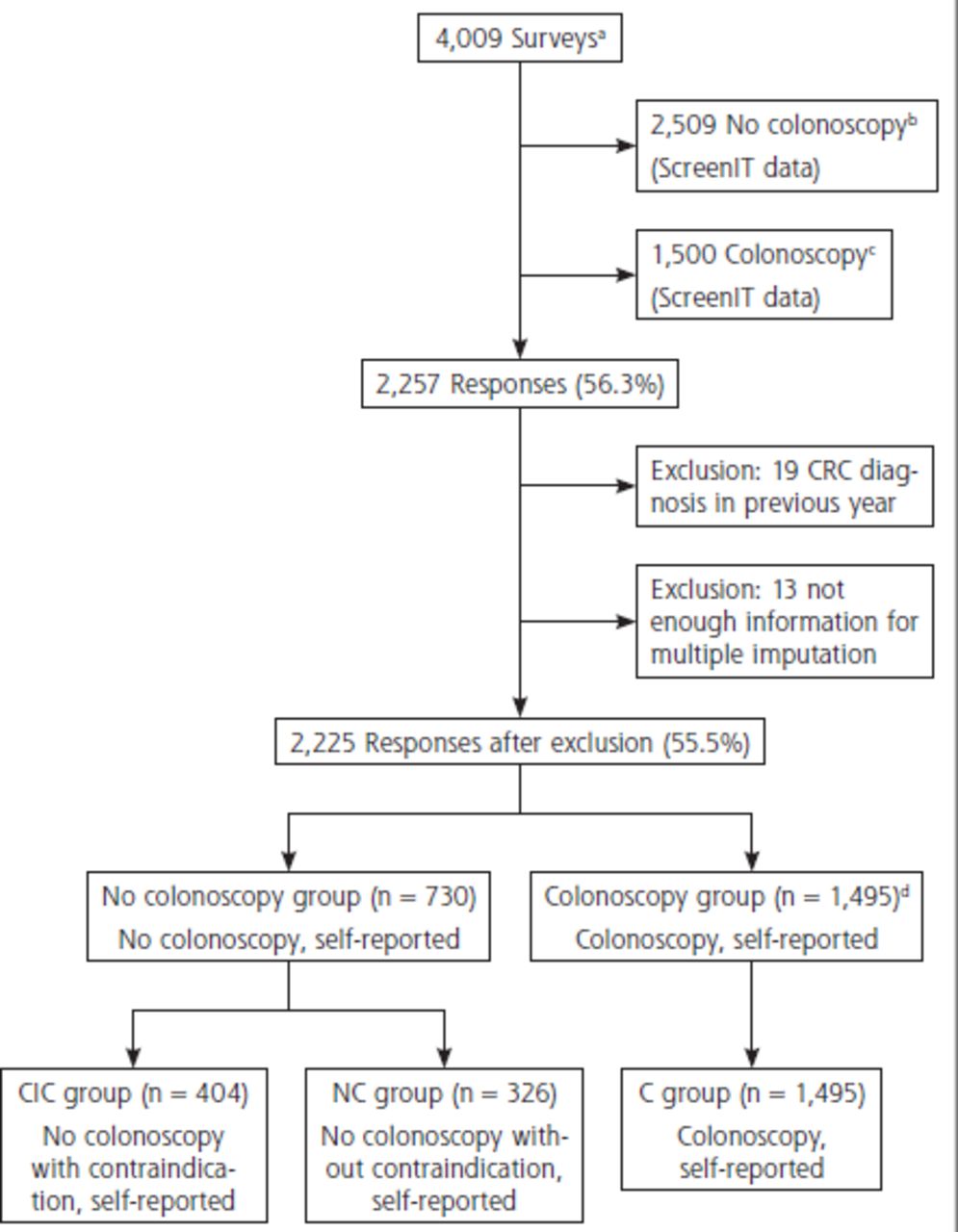
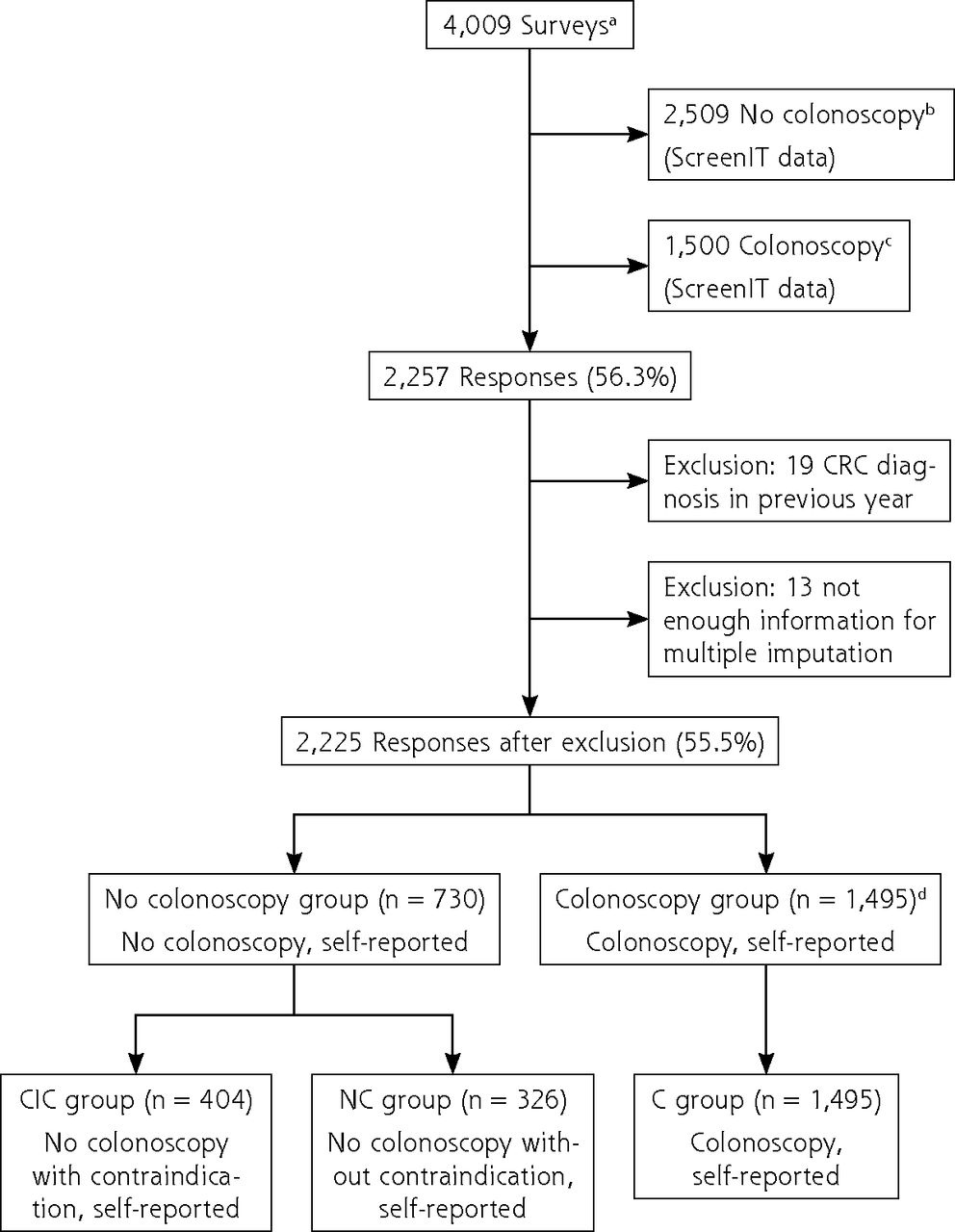
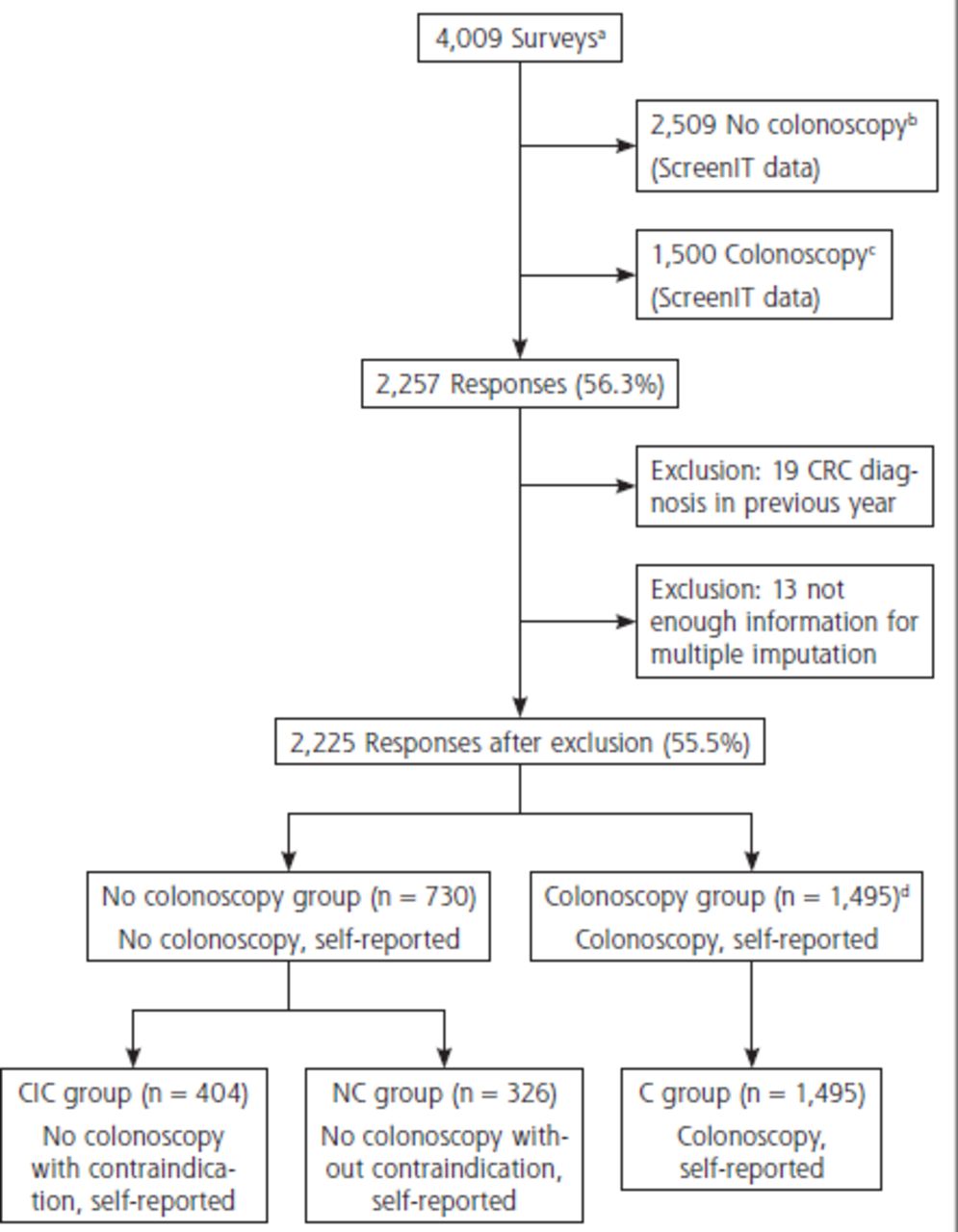
- Figure 2.
Overview of inclusion.
C = colonoscopy; CIC = contraindication and no colonoscopy; CRC = colorectal cancer; FIT = fecal immunochemical test; NC = no colonoscopy and no contraindication; ScreenIT = database of the Netherlands National Institute for Public Health and the Environment, which is the Dutch screening organization.
a Participants in the Dutch CRC screening program with a positive FIT 4-6 months ago at time of postal mailing of questionnaires.
b All FIT-positive participants with a positive FIT 4-6 months ago who did not undergo colonoscopy in the Netherlands were sent the questionnaire.
c Control group that did undergo colonoscopy matched to no colonoscopy group for age, sex, and previous participation in the screening program.
d Because it was unlikely that 1,495 individuals responded of the 1,500 that were sent the questionnaire (see C), it appeared that a proportion of individuals who were registered as no colonoscopy (see B) did report a colonoscopy and therefore ended up in the colonoscopy group (see C) in this study.
Tables
Characteristic Missing or No Answer % CIC Group (n = 404) NC Group Sig. (2-Tailed)a C Group Sig. (2-Tailed)b N %c or Mean P (Mean Difference)d P (Mean Difference)d Age, y 15 NA 67.61 .292 .001 (1.19) Male 14 183 47.3% .482 .02 Living with partner 15 280 69.3% .002 (0.113) .054 Having ≥1 child 15 298 86.6% .003 (0.09) .686 Living in urban area 18 333 44.4% .07 .187 Educational level 18 Primary NA 19 4.7% .233 .941 Secondary NA 113 28.0% .728 .569 Vocational training NA 105 26.0% .139 .001 (−0.081) Higher education NA 94 23.3% .705 .02 Sufficient financial resources 28 257 88.6% .004 (.092) .981 Not born in the Netherlands 13 22 6.3% .032 .979 C = colonoscopy; CIC = contraindication no colonoscopy; NA = not applicable; NC = no colonoscopy no contraindication; Sig. = significance level.
↵a Two-tailed independent t test comparing means of CIC group and NC group.
↵b Two-tailed independent t test comparing means of CIC group and C group.
↵c Valid percentages (percentages left when missing data are excluded from the calculation) reported.
↵d Mean difference vs control group stated for variables with a significance level of P < .05.
Reason No. % % of Cases
(Nr = 730)Had a recent colonoscopy 211 14.0 28.9 Alternative explanation for positive FITa 214 14.2 29.5 Chronic illness 172 11.5 23.6 Diagnosis of ulcerative colitis/Crohn disease or other reason for regular visits with gastrointestinal specialist or internist 130 8.7 17.8 Advised against colonoscopy by gastrointestinal specialist or internist 93 6.2 12.7 Aversion to colonoscopy 73 4.9 10.0 FP advised against colonoscopy 71 4.7 9.7 Had a second negative FIT 69 4.6 9.5 Acute illness 63 4.2 8.6 Undergoing cancer treatment 56 3.7 7.7 No answer provided 47 3.1 6.4 Advised against colonoscopy during intake for colonoscopy 44 2.9 6.0 No symptoms/fecal blood has no meaning 31 2.1 4.2 Short life expectancy 30 2.0 4.1 Medical barrier 27 1.8 3.7 Fear of outcome 25 1.7 3.4 Practical barrier 24 1.6 3.3 Want a second FIT 17 1.1 2.3 Want more personalized care 16 1.1 2.2 Low perception of risk of CRC 14 0.9 1.9 Financial consequences of colonoscopy 13 0.9 1.8 Nonmedical priorities 11 0.7 1.5 Do not want treatment if CRC is found 11 0.7 1.5 Distrust screening test, organization, or process 11 0.7 1.5 Other reason, without contraindication 10 0.7 1.4 Nurse advised against colonoscopyb 7 0.5 1.0 Had a second opinion (CT colonography/MRI) 6 0.4 0.8 Dementia, mental disability, severe psychiatric issues 6 0.4 0.8 Totalc 1,502 100.0 205.8 CRC = colorectal cancer; CT = computed tomography; FIT = fecal immunochemical test; FP = family physician; MRI = magnetic resonance imaging; No. = number of times reason was mentioned; Nr = total number of respondents who reported not undergoing colonoscopy, excluding respondents with recent CRC diagnosis and respondents of whom it was unclear if they underwent colonoscopy.
Note: Reasons highlighted in bold were considered a valid contraindication for colonoscopy.30,34
% = proportion of all reasons mentioned; % of cases = proportion of Nr that mentioned reason.
↵a Thinking blood in stool was caused by hemorrhoids, fissure, constipation, medication, or other and not underlying neoplasia.
↵b Refers to care personnel, such as district nurses or homecare, without a medical degree.
↵c Most respondents reported >1 reason.
- Table 3.
Demographic Characteristics and Descriptive Statistics of CRC Knowledge Items for C and NC Groups
Characteristic Totala
(n = 1,821)Missing, % C Groupa
(n = 1,495)NC Groupa
(n = 326)P Value
(χ2)Age, mean, y 66.5 4.7 66.4 67.1 .66 Male, No. (%) 1,033 (58.9) 3.7 861 (59.7) 172 (55.5) .17 Living with partner, No. (%) 1,299 (71.3) 4.7 1,110 (74.2) 189 (58.0) <.001 Having ≥1 child, No. (%) 1,475 (84.7) 5.4 1,239 (86.4) 236 (76.9) <.001 Living in urban area, No. (%) 720 (42.4) 6.8 570 (40.5) 150 (51.7) <.001 Educational level, No. (%) 6.8 .08 Primary 90 (4.7) NA 68 (4.8) 22 (7.6) .1 Secondary 492 (26.7) NA 397 (28.2) 95 (32.8) .34 Vocational training 610 (33.6) NA 509 (36.2) 101 (34.8) .29 Higher education 504 (27.6) NA 432 (30.7) 72 (24.8) .01 Insufficient financial resources, No. (%) 191 (13.0) 19.1 140 (11.4) 51 (20.6) .002 Not born in the Netherlands, No. (%) 125 (7.2) 4.1 91 (6.3) 34 (11.0) .004 Had ≥1 CRC-related symptom at time of FIT, No. (%) 622 (34.2) NA 512 (34.2) 110 (33.7) .86 Visible blood 422 (24.5) 5.3 335 (23.6) 87 (28.5) .07 Tenesmus 176 (10.6) 9.0 156 (11.4) 20 (6.8) .02 Stool pattern change 190 (11.1) 5.9 171 (12.1) 19 (6.4) .004 Weight loss 61 (3.6) 6.5 53 (3.8) 8 (2.7) .35 CRC knowledge item, No. (%)b CRC always causes symptoms 904 (52.8) 5.9 700 (49.3) 204 (69.4) <.001 Positive FIT usually means cancer 417 (24.3) 5.8 295 (20.8) 122 (41.4) <.001 Screening is meant for persons with symptoms 562 (32.9) 6.1 414 (29.3) 148 (50.2) <.001 Negative FIT ensures absence of cancer 806 (47.0) 5.8 659 (46.4) 147 (50.0) .26 Colonoscopy has high risk of complications 647 (37.8) 6.0 460 (32.4) 187 (64.0) <.001 Having symptoms means that cure is not possible 371 (21.7) 6.0 269 (19.0) 102 (34.7) <.001 CRC does not develop over several yearsc 933 (54.4) 5.8 750 (52.7) 183 (62.5) .002 Removing polyps does not prevent CRCc 621 (36.4) 6.2 436 (32.7) 158 (53.9) <.001 CRC cannot be cured, even if it is found at an early stagec 373 (21.8) 6.0 281 (19.8) 92 (31.3) <.001 >75% of people with CRC die of it 913 (53.2) 5.8 716 (50.4) 197 (67.0) <.001 High levels of trust in ability to self-detect CRCc 251 (14.6) 5.8 152 (10.7) 99 (33.8) <.001 C = colonoscopy; CRC = colorectal cancer; FIT = fecal immunochemical test; NA = not applicable; NC = no colonoscopy no contraindication.
↵a Valid percentages (percentages left when missing data are excluded from the calculation) reported.
↵b No. = answers of “true” and “don’t know” combined.
↵c Questions were originally phrased positively (eg, “CRC develops over several years”) but were rephrased in the negative sense for readability.
Variablea β SE Sig. (P)b OR Lower
95% CIUpper
95% CIKnowledge-associated factors Alternative explanation for blood in stool sample −1.202 0.179 <.001 0.301 0.212 0.427 High trust in ability to self-detect CRC by monitoring own body −0.86 0.22 <.001 0.423 0.274 0.654 Colonoscopy has high risk of complications −0.696 0.177 <.001 0.499 0.352 0.706 Removing polyps does not prevent CRC −0.524 0.167 .002 0.592 0.427 0.821 Participant-associated factors Negative colonoscopy advice from someone outside medical setting −1.265 0.387 .002 0.282 0.13 0.616 Difficulty deciding to undergo colonoscopy −1.24 0.241 <.001 0.29 0.18 0.466 Low estimation of personal risk for CRC −0.81 0.268 .003 0.445 0.261 0.758 Know others with negative colonoscopy experience −0.688 0.24 .004 0.502 0.314 0.805 CRC-related worry (cancer worry scale) 0.096 0.038 .012 1.101 1.022 1.187 Positive colonoscopy advice from anyone 0.571 0.188 .002 1.77 1.223 2.56 Had negative colonoscopy experience 0.685 0.246 .005 1.983 1.225 3.212 Provider-associated factors Thinks that FP would support colonoscopy 1.045 0.176 <.001 2.843 2.012 4.016 Contact with FP regarding FIT outcome −0.255 0.184 .167 0.775 0.54 1.113 System-associated factors Little opportunity to discuss desirability of colonoscopy −0.796 0.238 .001 0.451 0.281 0.724 Uncomfortable with unfamiliar colonoscopy location −0.758 0.227 .001 0.469 0.3 0.733 Total trust in 3 dimensions (organization, clinic, FIT)c 0.16 0.053 .004 1.173 1.055 1.305 C = colonoscopy; CRC = colorectal cancer; FIT = fecal immunochemical test; FP = family physician; NC = no colonoscopy no contraindication; OR = odds ratio; Sig. = significance level.
↵a Nagelkerke R2 = 0.521 for pooled results.
↵b Results interpreted as statistically significant at P < .05.
↵c Cronbach α = 0.836.
SUPPLEMENTAL DATA IN PDF FILE BELOW
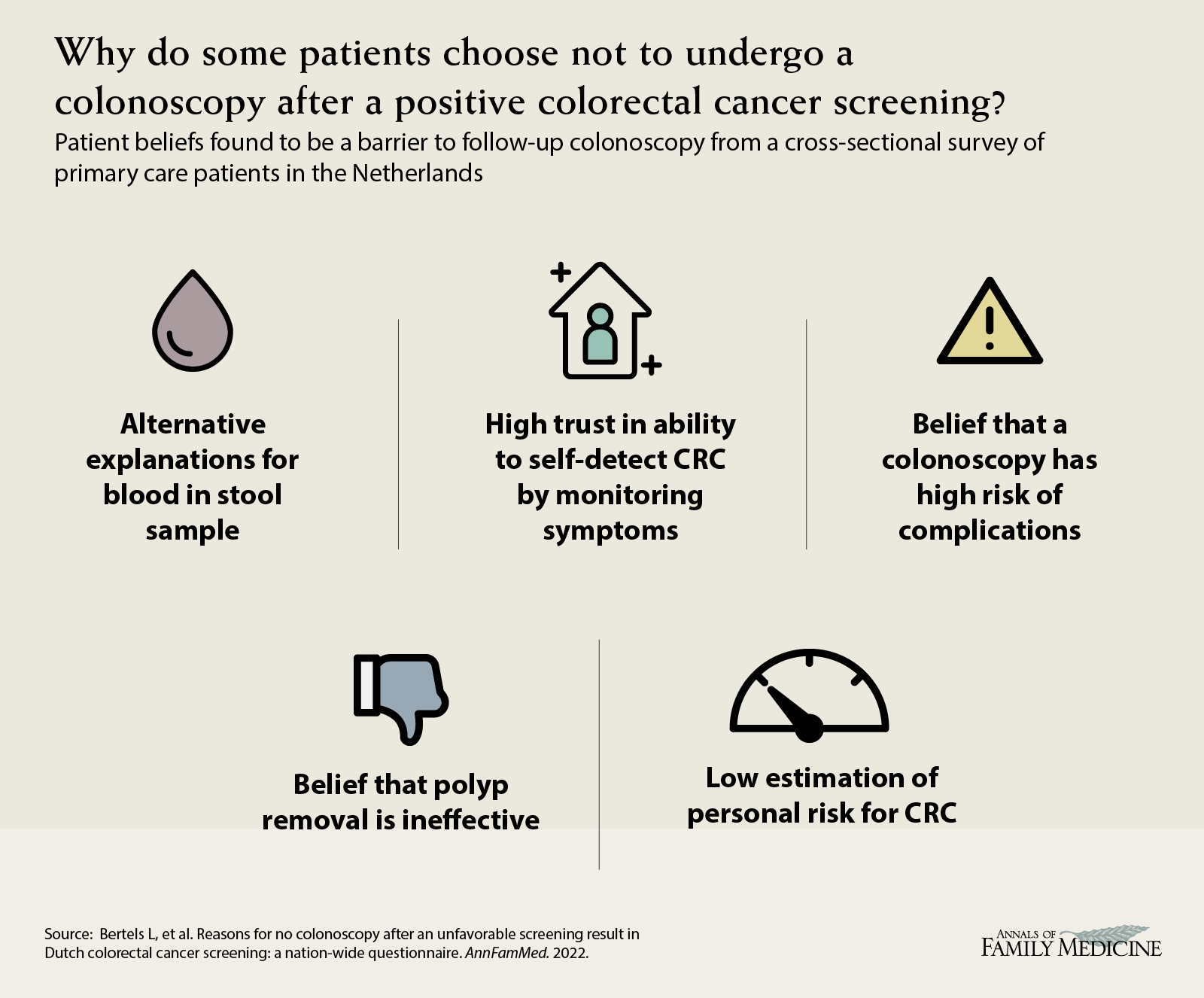
VISUAL ABSTRACT IN PNG FILE BELOW




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.