
Abstract
PURPOSE This study examined differences in Quitline treatment enrollment, engagement, and smoking cessation outcomes among primary care patients preferring Spanish and English using the evidence-based tobacco treatment Ask-Advise-Connect.
METHODS Ask-Advise-Connect was implemented April 2013 through February 2016 in a large safety-net health system to connect smokers with treatment via a link in the electronic health record. Rates of treatment enrollment, engagement, acceptance of nicotine replacement therapy, and smoking abstinence (self-reported and biochemically confirmed) were compared at 6 months among patients who received treatment in Spanish and English using χ2 tests. Logistic regression examined language and nicotine replacement therapy and their interaction as predictors of abstinence.
RESULTS The smoking status of 218,915 patients was assessed and recorded in the electronic health record. Smoking prevalence was 8.4% among patients preferring Spanish and 27.0% among those preferring English. Spanish-preferring patients were less likely to enroll in treatment (10.7% vs 12.0%, χ2 = 12.06, P = .001) yet completed more counseling calls when enrolled (median = 2 vs 1, P <.001). Patients who received treatment in Spanish (vs English) were twice as likely to be abstinent at 6 months (self-reported: 25.1% vs 14.5%, odds ratio [OR] = 1.98, 95% CI, 1.62-2.40; biochemically confirmed: 7.6% vs 3.7%, OR = 2.13, 95% CI, 1.52-2.97). Receipt of nicotine replacement therapy increased abstinence for all patients and language did not interact with nicotine replacement therapy to predict abstinence.
CONCLUSIONS Automated point-of-care approaches such as Ask-Advise-Connect have great potential to reach Spanish-preferring smokers. Those who received tobacco treatment in Spanish (vs English) demonstrated better engagement and cessation outcomes.
INTRODUCTION
Cigarette smoking is the leading cause of preventable death in the United States. Although the prevalence of smoking has declined to 14% among adults, it has become more concentrated among vulnerable populations such as racial/ethnic minorities and those with low socioeconomic status.1 Hispanic/Latino/a/x/e persons (hereafter referred to as Hispanic individuals) constitute 18% of the US population and smoking-related illnesses (eg, cancer, heart disease, stroke) are the leading causes of death within this population.2,3 Unfortunately, in part due to the lack of health insurance coverage and language barriers, Hispanic individuals are less likely than non-Hispanic White individuals to be screened for tobacco use and receive advice to quit in primary care settings. Those in the Hispanic population are also less likely to use evidence-based cessation aids, such as nicotine replacement therapy (NRT), when attempting to quit.4-8
Although tobacco cessation rates are generally equivalent for Hispanic and non-Hispanic White patients, cessation interventions specifically targeting Spanish-preferring smokers are scarce, appear to have only modest effects at the end of treatment, and are mixed in longer-term efficacy.9-12 Therefore, providing cessation resources tailored to language preferences and reducing tobacco use among Hispanic individuals are critically important public health priorities.
All state Quitlines offer treatment in Spanish. While Spanish-language telephone counseling is effective and acceptable to participants,11-13 Quitline-delivered treatment for Hispanic individuals (0.44% to 0.80% annually) is approximately 2 to 4 times lower than for the general population of smokers (1% to 2% annually).14,15 Thus, efforts are needed to improve reach within this underserved population of smokers. Ask-Advise-Connect (AAC) is an approach developed to seamlessly connect smokers in primary care settings with Quitline-delivered treatment through an automated link within the electronic health record (EHR).16-18 Two large group-randomized trials found that AAC was associated with a 13- to 30-fold increase in treatment enrollment compared with an Ask-Advise-Refer control condition, in which smokers received referral cards and encouragement to call the Quitline on their own.16,17
An AAC implementation trial was conducted within a large safety-net health care system.19 The patient population served by this system is racially/ethnically diverse: 58.9% identify as Hispanic and approximately 50% prefer use of Spanish. This study is a secondary data analysis comparing rates of Quitline treatment enrollment, engagement, and effectiveness among patients preferring Spanish vs English.
METHODS
Participants
Participants were adult patients (aged 18 years or older) who presented for care at any of the 13 Harris Health primary care clinics during the implementation period (April 2013 through February 2016). Participants were given a written study information sheet and provided verbal consent to have their contact information sent to the Quitline, which was documented in the EHR. The study was approved by the Institutional Review Boards at The University of Texas MD Anderson Cancer Center, Harris Health, and the Texas Department of State Health Services.
Procedure
Ask-Advise-Connect
Licensed vocational nurses were trained to assess and record the smoking status of all patients at all visits in the EHR at the time vital signs were collected, deliver brief advice to all smokers to quit, and offer to immediately send each smoker’s name, telephone number, and language preference to the Quitline so that they could be contacted and offered treatment. The contact information of those who agreed to be connected was sent to the Quitline through an automated system in the EHR and also sent to our research team for tracking purposes. The Quitline called smokers within 48 hours. Quitline staff made 5 call attempts over a period of 2 weeks before patients were classified as unreachable.
Quitline-Delivered Treatment
The Quitline was funded by the State of Texas, operated by Optum, and staffed by trained counselors who were available 24 hours a day, 7 days a week, and most holidays. Counseling was offered in Spanish and English and could be provided in other languages through a third party. Smokers who enrolled in treatment were given the opportunity to receive the standard treatment protocol consisting of up to 5 counseling calls to provide practical support for developing problem-solving and coping skills, securing social support, and planning for successful cessation and long-term abstinence.
The initial call helped patients identify a quit date and follow-up calls occurred a day or 2 after the quit date, 1 week post quit date, and at subsequent 2- to 3-week intervals. Participants were able to call an 800 number as needed for support between counseling calls. A 2-week supply of NRT (eg, patch, gum, lozenge) was offered to some participants based on the Quitline’s standard operating procedures (ie, resident of a tobacco coalition county in Texas and when adequate funding was available).
Informed Consent for Follow-Up Assessment and Biochemical Verification
At treatment enrollment, participants were asked by Quitline staff if they were willing to be contacted about their smoking status in 6 months. Verbal consent was recorded and consent to complete the follow-up assessment was obtained by our research team just before completion of the assessment.
To biochemically verify smoking status, participants who reported abstinence for the previous 7 days were mailed a saliva collection kit within 24 hours that contained the following: the informed consent document, instructions on providing the cotinine sample, the saliva collection kit, and a prepaid return envelope. Research staff contacted participants by telephone to ensure receipt of the packets, review the contents, and guide participants in the saliva collection and return procedures. Participants who returned a sample were compensated with a $25 gift card.
Outcome Measures
Primary outcomes included (1) treatment enrollment (ie, proportion of identified smokers that enrolled in Quitline treatment); and (2) biochemically confirmed, self-reported 7-day point-prevalence abstinence from smoking at 6 months. Additional outcomes included (1) treatment engagement (ie, number of counseling calls completed); and (2) whether NRT was provided. Smoking cessation outcomes were examined using an intent-to-treat approach in which participants who did not complete the 6-month follow-up were classified as smoking. Those who reported being abstinent but returned saliva samples with cotinine levels of 20 ng/ml or more were classified as smoking.20
Statistical Analysis
First, the prevalence of smoking was examined by preferred language among all patients. Next, proportions of patients enrolled in Quitline treatment were calculated by preferred language. Patients who received Quitline treatment in Spanish were classified as Spanish-preferring and those who received treatment in English were classified as English-preferring. Third, abstinence rates at 6 months (self-reported and biochemically confirmed) were calculated and compared among patients who received treatment in Spanish and in English and who agreed to be contacted for follow-up. These proportions were compared using χ2 tests.
Counseling call completion rates were categorized as 0, 1, 2, or 3 or more calls. The median number of counseling calls completed was compared among those who received treatment in Spanish vs English using the Wilcoxon-Mann-Whitney U test. Logistic regression analyses examined: (1) the language in which treatment was received (Spanish vs English) and (2) the provision of NRT as predictor of smoking abstinence. Interaction terms were included in the logistic regression models to examine whether treatment language (1) by number of counseling calls completed and (2) by NRT receipt, influenced smoking cessation outcomes.
RESULTS
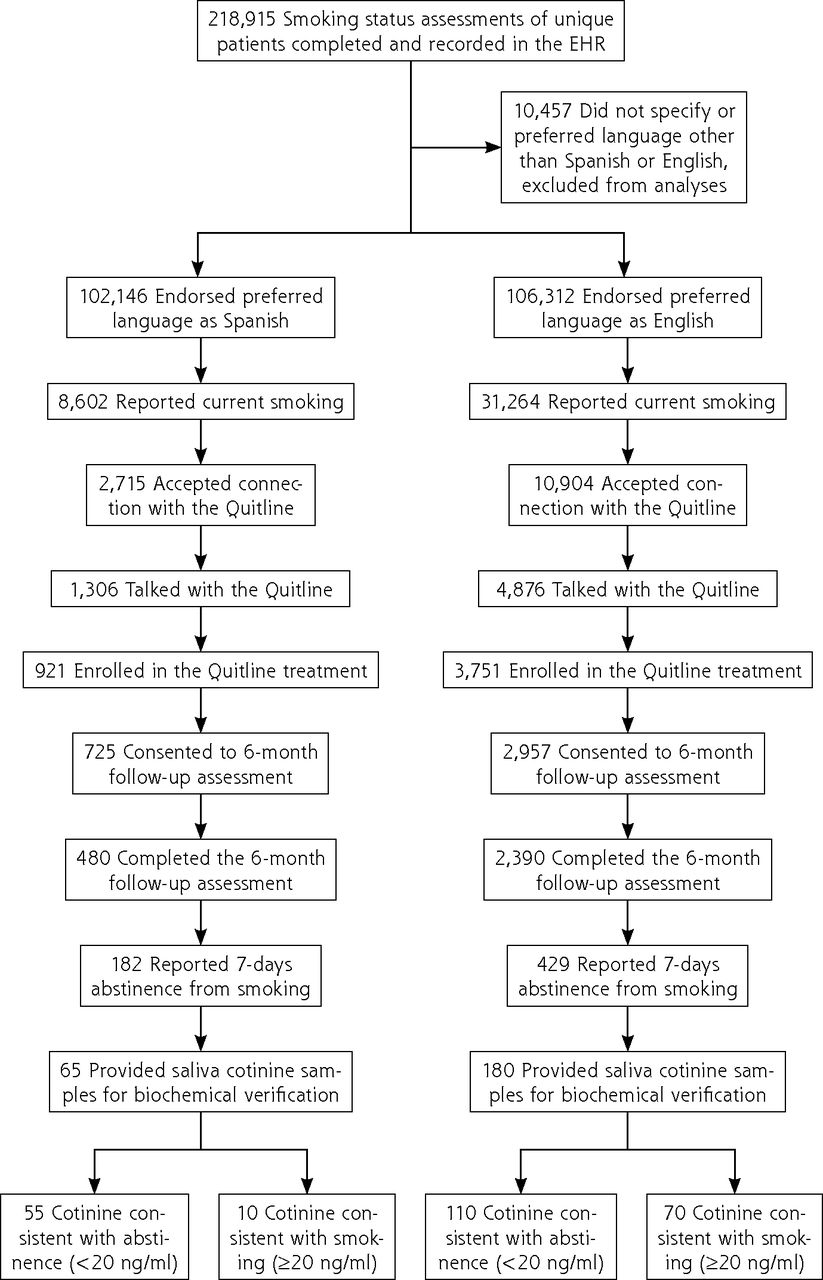
The smoking status of 218,915 unique patients across all 13 clinics was assessed and recorded in the EHR during the study. The prevalence of smoking among English-preferring patients was 27.0% (31,264/115,747) and the prevalence of smoking among Spanish-preferring patients was 8.4% (8,602/102,146) (Table 1, Figure 1).
Enrollment, Receipt of Treatment, and 6-Month Abstinence Rates by Language Preference (N = 39,866)

Flowchart of participants and smoking abstinence outcomes.
EHR = electronic health record.
Quitline Treatment Enrollment and Agreement to Be Contacted for Follow-Up
Smokers with a documented language preference of English were significantly more likely to enroll in Quitline treatment (12.0%, 3,751/31,264) than those with a documented preference of Spanish (10.7%, 921/8,602; χ2 = 12.06, P = .001). At the time of Quitline treatment enrollment, 78.7% (725/921) of participants who received treatment in Spanish and 78.8% (2,957/3,751) of participants who received treatment in English agreed to be contacted for follow-up (χ2 = 0.006, P = .94).
Quitline Treatment Engagement (Counseling Calls)
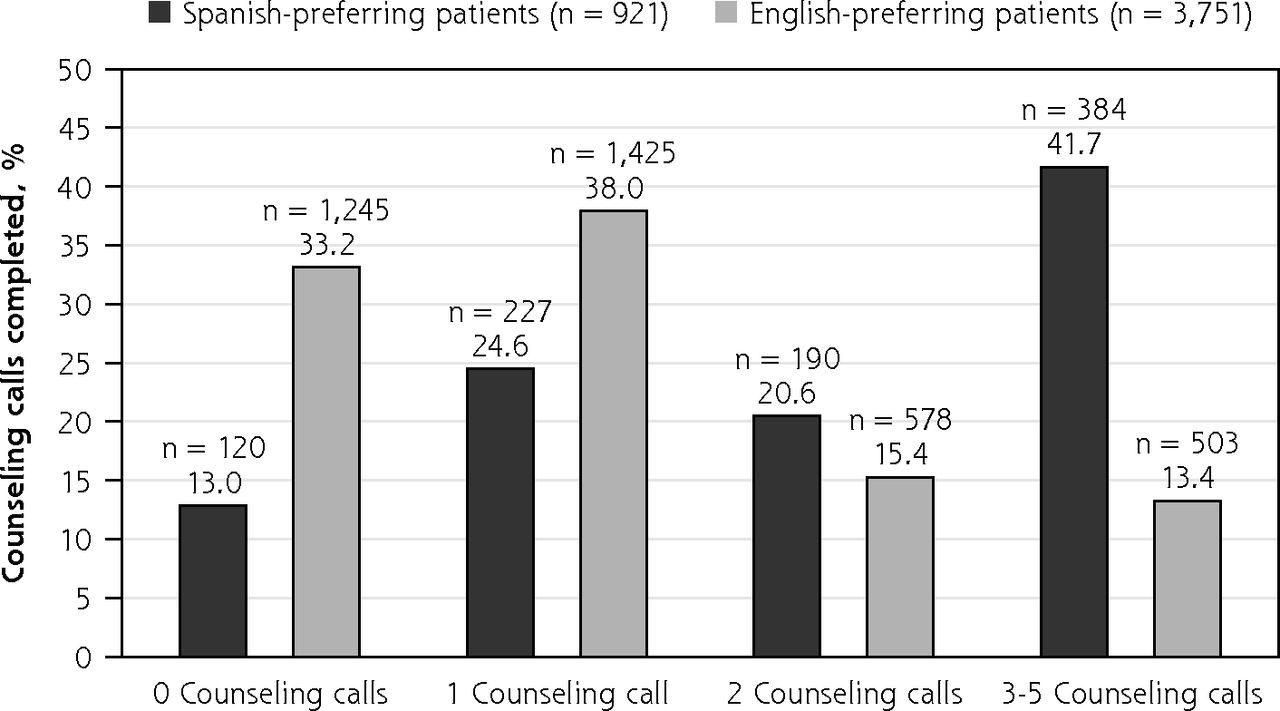
The majority of those treated in English completed 0 or 1 call (71.2%, 2,670/3,751), while the majority of those treated in Spanish completed 2 to 5 calls (62.2%, 574/921) (Figure 2). Thus, those treated in Spanish (vs English) completed twice as many counseling calls (median: Spanish = 2, English = 1; Wilcoxon-Mann-Whitney U = 1769488.50, P <.001). Completing more counseling calls was associated with better cessation outcomes for patients preferring either Spanish or English (Table 2). Counseling calls did not interact with language preference to predict cessation outcomes (P >.35).

Quitline treatment engagement by language preference.
Smoking Abstinence Rates at 6 Months by Language Preference and Treatment Engagement (N = 4,672)
Smoking Abstinence Rates by Treatment Language Preference
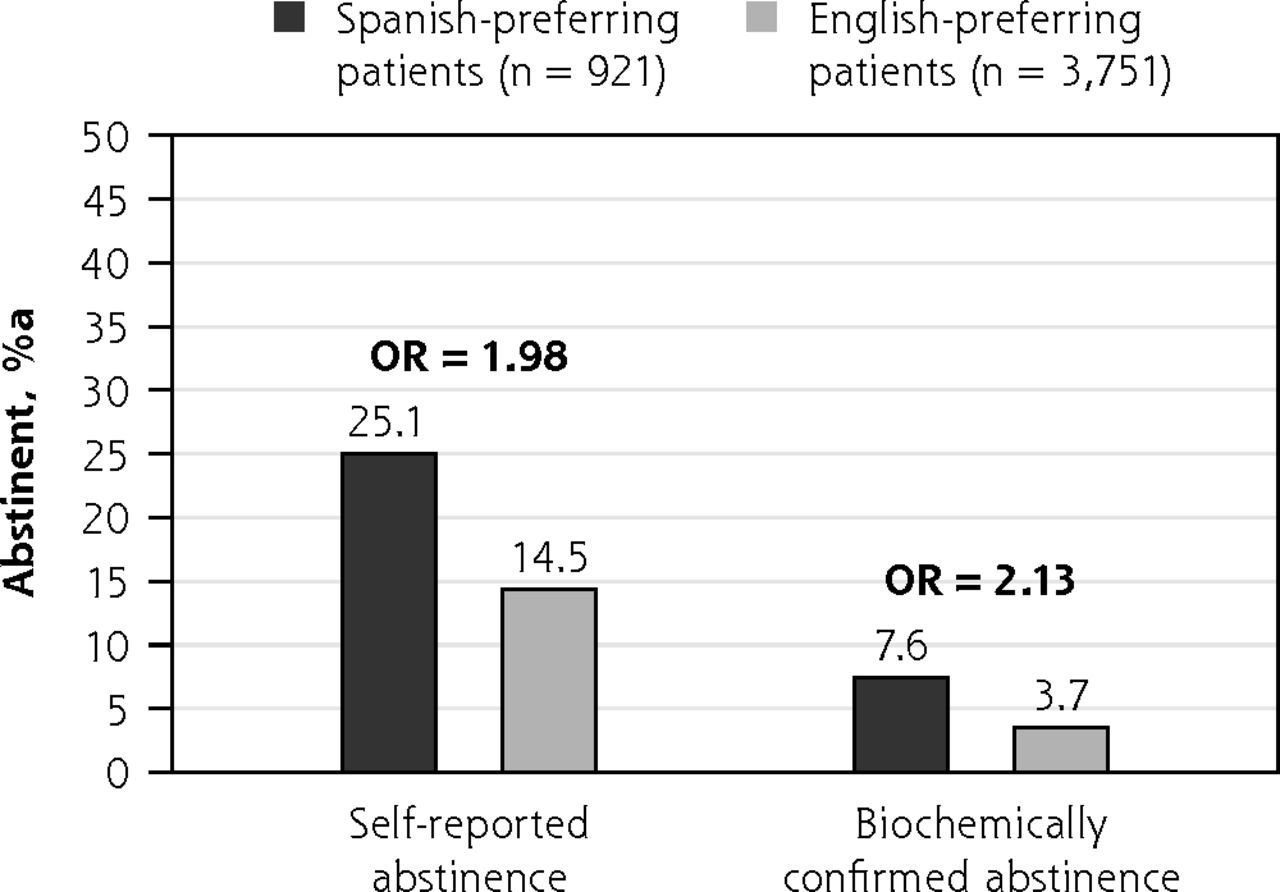
Self-reported abstinence at the 6-month follow-up among those who received treatment in Spanish was 25.1% (182/725) compared with 14.5% (429/2,957) for those who received treatment in English. Logistic regression analysis revealed those who received treatment in Spanish vs English were significantly more likely to report abstinence (odds ratio [OR] = 1.98, 95% CI, 1.62-2.40) (Figure 3). Biochemically confirmed abstinence (cotinine levels <20 ng/mL) was substantially lower than self-reported abstinence: 30.2% (55/182) for those preferring Spanish and 25.6% (110/429) for those preferring English (Figure 1). Biochemically confirmed abstinence was significantly higher among those preferring Spanish (7.6%; 55/725) than among patients preferring English (3.7%, 110/2,957; OR = 2.13, 95% CI, 1.52-2.97) (Figure 3).

Smoking abstinence rates at 6 months for Quitline treatment by language preference.
OR = odds ratio.
a Abstincence percentage based on self-report of abstinence for the previous 7 days.
Smoking Abstinence Rates by Receipt of NRT
During the study period 77.2% (560/725) of those who received treatment in Spanish and 51.6% (1,526/2,957) of those who received treatment in English were eligible for and accepted an offer of a 2-week supply of NRT (patch, gum, or lozenge) from the Quitline. Those who received treatment in Spanish vs English were more likely to be provided NRT (OR = 3.18, 95% CI, 2.64-3.84). NRT provision was significantly associated with abstinence at 6 months such that Spanish-preferring smokers who were (vs were not) provided with NRT were more likely to self-report abstinence at 6 months (OR = 2.06, 95% CI, 1.31-3.26) and to have biochemically confirmed abstinence (OR = 3.14, 95% CI, 1.23-8.00). Similarly, English-preferring smokers who were (vs were not) provided with NRT were more likely to self-report abstinence (OR = 1.57, 95% CI, 1.27-1.93) and to have biochemically confirmed abstinence (OR = 1.89, 95% CI, 1.27-8.83). There was no interactive effect of NRT and language on self-reported (P = .29) or biochemically confirmed smoking abstinence (P = .33).
DISCUSSION
In this real-world AAC implementation study, we examined differences in Quitline treatment enrollment, engagement with Quitline counseling, receipt of NRT, and long-term smoking abstinence among patients preferring Spanish and English in a large health care system serving predominantly uninsured or underinsured, low income, racial/ethnic minority persons with diverse language preferences. Smokers with a documented preferred language of English (vs Spanish) enrolled in Quitline treatment at a significantly higher rate, although the absolute difference was relatively small (12.0% vs 10.7%) and may not be clinically meaningful. Patients who received treatment in Spanish completed significantly more counseling calls and had significantly and substantially higher self-reported and biochemically confirmed abstinence rates than those preferring English. An important caveat is that patients who received treatment in Spanish were also more likely to be provided with NRT. Nonetheless, our findings suggest that streamlined, automated approaches to linking smokers with preferred-language treatment in primary care settings have great potential to reach, engage, and substantially improve cessation outcomes for patients preferring treatment in Spanish.
The provision of NRT improved self-reported and biochemically confirmed smoking cessation outcomes for both groups of smokers. Although we did not collect data regarding the proportion of individuals who declined NRT when offered, most Spanish-preferring patients who enrolled in treatment (77%) were eligible and accepted free NRT when offered. Our study adds to the literature indicating that Hispanic smokers are willing to accept NRT when offered at no-cost and that NRT provision is effective in increasing smoking cessation.7,10,21-25
Patients preferring Spanish (vs English) demonstrated markedly better treatment engagement, often completing 3 or more of the 5 counseling calls offered (Figure 1). This is meaningful given that 3 calls is the minimum number recommended by the Quitline for effective treatment14 and aligns with prior work indicating that completing more Quitline calls is associated with better cessation outcomes.26-28 Previous research also indicates Hispanic smokers value personal contact as a part of intervention delivery,29-31 which may account for the increased treatment call engagement and subsequently higher abstinence rates for Spanish-preferring patients. Another potential explanation is that Spanish-preferring individuals may have had higher treatment engagement rates because they simply perceived few alternative treatment options. That is, it may be that Spanish-preferring patients placed a higher value on Quitline-delivered treatment because they were not aware of potential viable alternatives available in Spanish. It is also possible that the Quitline counselors who delivered treatment in Spanish were more effective at developing a strong rapport and facilitating engagement with their patients. Finally, Spanish-preferring Hispanic individuals tend to smoke fewer cigarettes and be less nicotine dependent than non-Hispanic White individuals, which may have contributed to higher abstinence rates.6,26,32
An additional finding that warrants attention is that patients preferring Spanish (vs English) were less likely to complete the follow-up assessment. Figure 1 reflects that 66% of those who received treatment in Spanish and 81% who received treatment in English completed the assessment. This pattern is consistent with prior studies which have had similar challenges with effectively engaging Spanish-preferring patients in research.33 The retention of Spanish-preferring patients is likely influenced by multiple factors including possible mistrust in government-funded research and worries about deportation among undocumented immigrants.34 These factors may have contributed to the lower observed follow-up rates among patients preferring Spanish observed in our study. Further research is needed to more clearly elucidate potential reasons for these differences and their potential implications.
Several limitations should be considered when interpreting our findings. First, results may not be generalizable to Spanish-preferring smokers who receive Quitline treatment in states other than Texas. Most Spanish-preferring individuals in Texas are Mexican or Mexican-American, and considerable heterogeneity exists in smoking behavior among Hispanic individuals of different national origins (eg, Mexican/Mexican Americans are more likely to be lighter smokers than Puerto Ricans).6,7,35,36 A number of studies, however, have found no differences in smoking cessation outcomes between Hispanic individuals of different national origin groups.6,10,11 Therefore, given that our study did not include a full spectrum Spanish-preferring persons representing all national origins, we are unable to conclude that Spanish-preferring patients in general are likely to have better treatment engagement and cessation outcomes than English-preferring patients. Second, there are limitations that exist due to the real-world nature of this study. Ask-Advise-Connect was implemented with all patients as a part of routine practice. To reduce clinic burden, we did not collect patient-level data (eg, demographics, dependence, motivation), which restricts our ability to investigate other potentially important predictors of treatment engagement or cessation outcomes such as education, employment, and marital status. Patient-level factors such as motivation to quit may have also influenced call completion. Future research should explore whether motivation, rather than the counseling received, influences abstinence. Additionally, we were only able to confirm receipt of NRT and, thus, we do not have information regarding the proportions of patients who accepted/declined NRT when offered, NRT use or adherence, or duration of use beyond the 2-week supply provided by the Quitline. Finally, Spanish-preferring patients were substantially more likely to be provided with NRT, and this unbalanced access to NRT makes it challenging to separate the beneficial effects of counseling vs NRT.
CONCLUSION
This study demonstrates that automated, point-of-care approaches such as AAC can effectively reach and enroll Spanish-preferring smokers in evidence-based tobacco treatment. Once enrolled, those who received treatment in Spanish had significantly higher rates of treatment engagement, were receptive to accepting NRT when available, and had substantially better cessation outcomes. Therefore, connecting smokers to state Quitlines in primary care settings has great potential for reducing tobacco-related health disparities among Spanish-preferring Hispanic individuals. Examining optimal methods of engaging Spanish-preferring smokers in treatment is a critically important priority for future research.
Footnotes
Conflicts of interest: authors report none.
Funding support: This work was supported by a grant from the Cancer Prevention Research Institute of Texas (PP120191; PI: J.I. Vidrine), the Oklahoma Tobacco Settlement Endowment Trust (092-016-0002; PI: J.I. Vidrine), the Stephenson Cancer Center’s Cancer Center Support Grant (P30CA225520; PI: Mannel), the Moffitt Cancer Center’s Cancer Center Support Grant (P30CA076292; PI: Cleveland), and the NIH T32 Behavioral Oncology Training Program at Moffitt Cancer Center (T32CA090314-18, PIs: Brandon, Vadaparampil).
Disclaimer: The study was approved by the Institutional Review Boards at The University of Texas MD Anderson Cancer Center, Harris Health, and the Texas Department of State Health Services. Participants were given a written study information sheet and provided verbal consent to have their contact information sent to the Quitline, which was documented in the EHR.
Previous presentation: Partial results of this paper presented at the 2018 AACR Conference on the Science of Cancer Health Disparities in Racial/Ethnic Minorities and the Medically Underserved; November 2-5, 2018; New Orleans, Louisiana.
- Received for publication December 3, 2021.
- Revision received May 19, 2022.
- Accepted for publication June 30, 2022.
- © 2022 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.