
Abstract
PURPOSE Interprofessional primary care has the potential to optimize hospital use for acute care among people with dementia. We compared 1-year emergency department (ED) visits and hospitalizations among people with dementia enrolled in a practice having an interprofessional primary care team with those enrolled in a physician-only group practice.
METHODS A population-based, repeated cohort study design was used to extract yearly cohorts of 95,323 community-dwelling people in Ontario, Canada, newly identified in administrative data with dementia between April 1, 2005 and March 31, 2015. Patient enrollment in an interprofessional practice or a physician-only practice was determined at the time of dementia diagnosis. We used propensity score–based inverse probability weighting to compare study groups on overall and nonurgent ED visits as well as on overall and potentially avoidable hospitalizations in the 1 year following dementia diagnosis.
RESULTS People with dementia enrolled in a practice having an interprofessional primary care team were more likely to have ED visits (relative risk = 1.03; 95% CI, 1.01-1.05) and nonurgent ED visits (relative risk = 1.22; 95% CI, 1.18-1.28) compared with those enrolled in a physician-only primary care practice. There was no evidence of an association between interprofessional primary care and hospitalization outcomes.
CONCLUSIONS Interprofessional primary care was associated with increased ED use but not hospitalizations among people newly identified as having dementia. Although interprofessional primary care may be well suited to manage the growing and complex dementia population, a better understanding of the optimal characteristics of team-based care and the reasons leading to acute care hospital use by people with dementia is needed.
- dementia
- interprofessional teams, primary care
- health system performance
- coordination of care
- administrative data
- population based
- practice-based research
- professional practice
- delivery of health care
INTRODUCTION
Interprofessional primary care (IPC), a team-based primary care model whereby family physicians collaborate with nurses, nurse practitioners, social workers, pharmacists, and other health professionals, has been touted as an ideal approach for dementia care.1-3 Because the management of dementia requires support from a wide range of clinicians,4,5 IPC may provide an integrated approach to counseling, managing comorbidities and medications, and coordinating care.5,6 Intervention studies have shown that IPC teams can improve care for people with dementia compared with physician-only primary care practices.2,7-10
Interprofessional primary care may also be an effective strategy to optimize acute care hospital use in people with dementia for whom this use frequently stems from acute problems or chronic conditions potentially preventable through high-quality primary care.11 Only a few intervention studies, however, have evaluated effects of IPC on emergency department (ED) and hospital outcomes in the dementia population, finding mixed results.2,8,12,13 One study showed a modest decrease in the number of ED visits,8 whereas 3 others found no meaningful differences.2,12,13 Aside from these intervention studies, to our knowledge, no study has examined the association between IPC and hospital use for acute care in people with dementia at a population level.
In Ontario, Canada, nearly 200 IPC teams have been introduced over the past 15 years; they currently serve 1 in 5 residents and are among the most comprehensive examples of IPC in North America.14,15 This setting offers an ideal opportunity to assess the potential association between IPC and hospital use for acute care among people with dementia at the population level.15 The aim of our study was therefore to compare acute care hospital use in people with dementia enrolled in an IPC practice with those enrolled in a physician-only group practice in Ontario.
METHODS
Setting and Data Sources
We extracted demographic, health, and service use data from the linked population-based health administrative data held at ICES in Ontario. ICES is an independent, nonprofit research institute whose legal status under Ontario’s health information privacy law allows it to collect and analyze health care and demographic data, without consent, for health system evaluation and improvement. ICES data are used regularly for health research.16
The ICES databases we used were the Registered Persons Database, which contains demographics such as age and sex; the Client Agency Program Enrolment and Corporate Provider Database to identify primary care enrollment and group affiliation; the Ontario Health Insurance Plan for physician claims; the Canadian Institute for Health Information Discharge Abstract Database and National Ambulatory Care Reporting System for acute care hospital use and ED visits; the Ontario Drug Benefit and drug identification number databases for dispensed prescription drugs; the Home Care Database, Resident Assessment Instrument, Continuing Care Reporting System, and Ontario health care institutions for home and long-term care services; and the vital statistics on death database for place of death. Admissions to long-term care were also determined through the Ontario Health Insurance Plan and Ontario Drug Benefit databases. Details on data sources and operational definitions for variables in our study are available elsewhere.17 These data sets were linked using unique encoded identifiers and analyzed at ICES.
This study was approved by the Research Ethics Board of McGill University in Montreal, Canada (study no. A12-M42-18B). The use of the data in this project is authorized under section 45 of Ontario’s Personal Health Information Protection Act and does not require review by a research ethics board.
Design and Population
We used a repeated cohort design to extract separate yearly cohorts of community-dwelling older adults, aged 65 years and older, in Ontario, newly identified with dementia between April 1 and March 31 from 2005 to 2015.18 Newly identified people with dementia were considered those with dementia identified in the 2 years before the start of each yearly cohort. The date of dementia diagnosis was ascertained from a previously validated algorithm based on health administrative data and corresponded to the earliest date of any of 3 physician encounter criteria occurring in the 2 years before April 1 of each yearly cohort: (1) at least 1 hospitalization with a dementia diagnosis code, (2) at least 3 physician claims with a dementia diagnosis code at least 30 days apart, or (3) a prescription for dementia medication.19 Cohorts were followed for up to 1 year or until death or long-term placement. As such, cohort periods were distinct with no overlap in individuals between cohort years. We excluded individuals with missing age, sex, or health identification number; nonresidents of Ontario; and those living in a long-term care facility on the date of dementia diagnosis.
Exposure
Individuals enrolled in a Family Health Team (FHT) on the date of dementia diagnosis constituted the IPC group. FHTs are physician-directed medical practices wherein family physicians work in collaboration with a wide range of nonphysician health professionals who can include nurses, nurse practitioners, social workers, pharmacists, dietitians, occupational therapists, and other clinicians, in order to provide timely, integrated, and comprehensive care to their patients. Team composition and roles vary from team to team based on capacity and needs, but the roles generally involve supporting physicians in conducting patient assessments, prevention, management, education, and health system navigation.20,21 Programs within FHTs vary depending on local community needs, but all generally focus on chronic disease management, health promotion, and disease prevention activities.
Individuals enrolled in a Family Health Organization (FHO), a physician-only primary care practice that is group based but does not use interprofessional care, constituted the non-IPC group. FHOs were selected as the comparator group among the set of other primary care models in Ontario because they were the most similar to FHTs in terms of patient, clinician, and remuneration characteristics—factors that have been previously discussed as major sources of confounding in comparisons between primary care models.22 FHOs were the largest among primary care models from which physicians could apply to transition their practice to an FHT and receive funding to recruit salaried health care professionals.22 Indeed, 54% of FHTs consist of FHOs that have transitioned into the team-based model.21 FHOs transitioning into FHTs retain the same structural elements, such as the payment model (blended capitation), use of electronic health records, extended hours, and access to 24/7 nurse telephone triage services; the only difference is the addition of nonphysician health care professionals. As a result, compared with FHOs, FHTs have more formalized chronic disease management plans and a focus on patient-centered care in line with the principles of patient-centered medical homes. Overall, FHTs and FHOs account for nearly one-half of registered patients in Ontario, with FHTs serving approximately 1 in 4 residents.
Enrollment in an FHT or FHO was determined through the Client Agency Program Enrolment and Corporate Provider Database, a database that identifies the primary care model in which an individual is enrolled. Given the difficulties in obtaining a family physician in Ontario as well as the formal rostering of patients to their family physicians, we considered the likelihood of patients switching between practice models over the 1-year follow-up period to be negligible.
Outcomes
The primary outcome was the occurrence of at least 1 ED visit in the year following dementia diagnosis. As many of the most frequent reasons for ED visits in the dementia population relate to reasons potentially preventable through better access to primary care or disease management,11 we hypothesized that receiving care from an IPC team would result in reduced use of the ED. Secondary outcomes included at least 1 nonurgent ED visit, all-cause hospitalization, and a potentially avoidable hospitalization in the follow-up year. A nonurgent ED visit was defined as a less urgent visit (level 4) or nonurgent visit (level 5) according to the Canadian Acuity Triage Scale.23 A potentially avoidable hospitalization was defined as one for which the chief diagnosis was an ambulatory care–sensitive condition: asthma, cardiac heart failure, chronic obstructive pulmonary disease, diabetes, hypertension, angina, or seizures.24
Potential Confounders and Other Covariates
We developed a causal diagram of the factors involved in the relationship between IPC and ED use to identify potential confounders and predictors (Supplemental Figure 1). The diagram was informed by the literature and consultations with more than 20 stakeholders, including representatives of people living with dementia, family physicians, and managers.
We obtained baseline data on covariates (age, sex, income, residence on the rural-urban spectrum, recent immigrant status, comorbidity, number of physician visits in the year before the date of dementia diagnosis, and prior resource use). Neighborhood-level income quintiles and residence (urban vs rural region) were determined from the 2011 national census.25 A rural area was defined as one having a community size of 10,000 people or fewer.26 Recent immigrant status was based on first registration into the Ontario health system within the past 10 years.25 We used the Johns Hopkins Adjusted Clinical Group (version 10) system27 to measure comorbidity and extent of resource use, and comorbidity was categorized using the Aggregated Diagnosis Group: 0 to 5 (low comorbidity), 6 to 10 (medium), or 11 and higher (higher comorbidity). Prior health resource use was measured by the number of prior physician visits and by the Resource Utilization Band, a measure of overall morbidity and cost based on quintiles of expected resource use: 0 (nonusers) and 1 (least expected use) to 5 (highest expected use).27 Comorbidity and resource use were calculated using data in the 2 years before the date of dementia diagnosis.
Analyses
We computed descriptive statistics for each study group. Propensity score–based inverse probability weighting was used to balance the IPC and non-IPC groups on measured confounders, creating a weighted sample mimicking a randomized sample.28,29 The propensity score was calculated using logistic regression analysis. Covariate balance was verified by comparing the propensity score and weight distributions in both groups and based on standardized mean differences of less than 0.01 between groups for each covariate.29 We derived risk differences, relative risks, and corresponding 95% CIs for the study outcomes from the weighted sample through bootstrap aggregating of the effect estimates from 1,000 bootstrapped samples. The number needed to treat was calculated as the inverse of the risk difference.
Data on marital and caregiver status, dementia severity, behavioral symptoms, functional status, self-reported health status, and receipt of antipsychotic medications were available for the subset of individuals who had received a Resident Assessment Instrument for Home Care for long-stay home care services and/or long-term care home placement.30 These additional covariates were extracted for individuals with assessment dates within 3 months before dementia diagnosis and used for sensitivity analysis.
We performed 3 sensitivity analyses for the primary outcome of overall ED use. First, we conducted a sensitivity analysis stratifying by residence to account for possible residual confounding given its importance as a potential confounder in the relationship between IPC and ED use.14,31 Second, we used propensity score calibration to incorporate additional data on covariates available for only a subset of the population (Supplemental Appendix).32 Third, we assessed the robustness of the estimated effect using the E-value (Supplemental Figure 2).33
All analyses were performed using SAS software, version 9.4 (SAS Institute Inc) and R software, version 3.4.2 (R Foundation for Statistical Computing).34
RESULTS
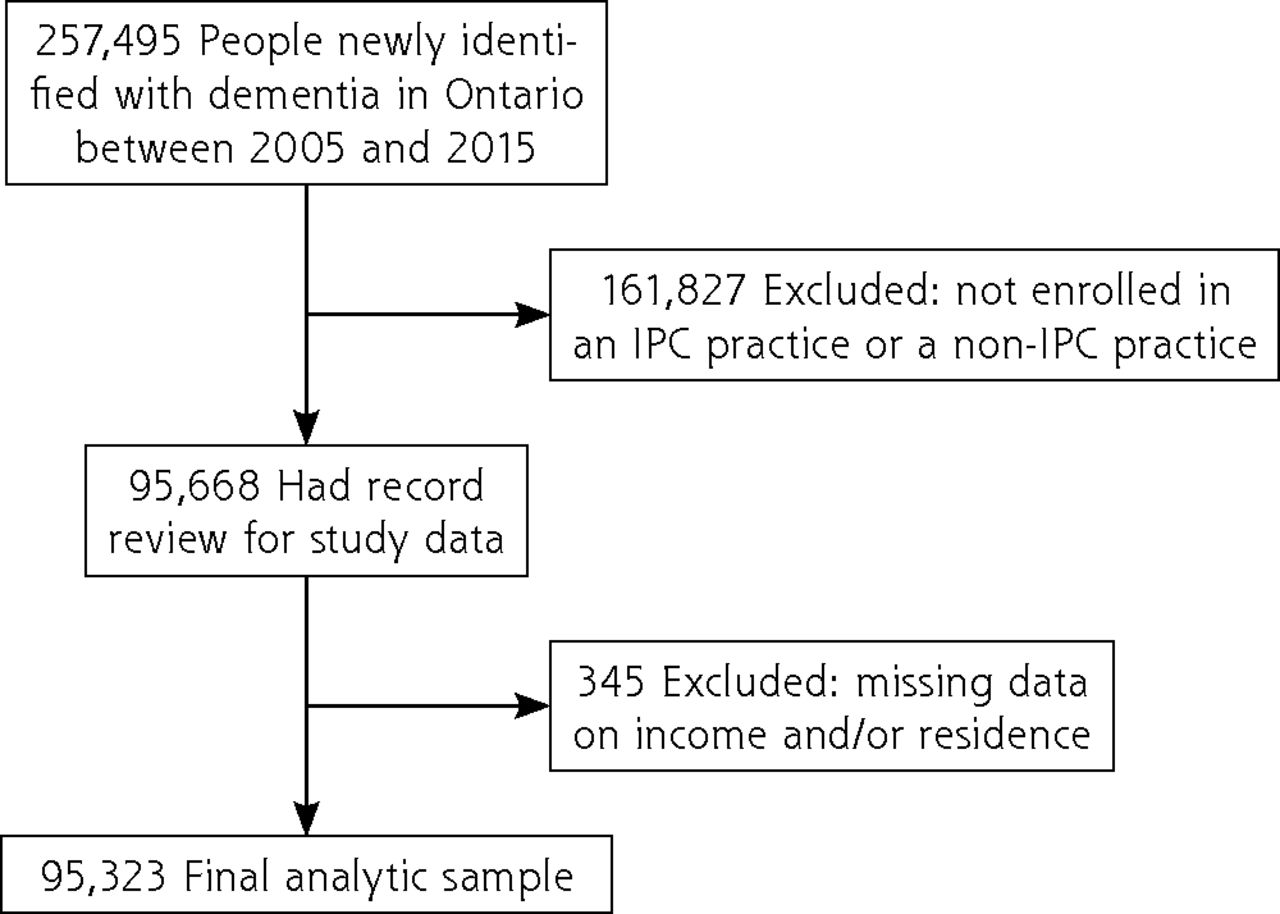
We determined that 257,495 community-dwelling people were newly identified with dementia in Ontario during 2005-2015 (Figure 1). Of these, 95,668 were enrolled in either an IPC practice or a non-IPC practice. The final analytic sample comprised 95,323 people after exclusion of those with missing data (0.3%). Among this sample, median follow-up was identical for both groups (1 year); 17.6% in the IPC group and 17.1% in the non-IPC group were admitted to long-term care or died during the 1-year follow-up period.

Flow diagram showing identification of study analytic sample.
IPC = interprofessional primary care.
Table 1 presents the baseline characteristics of the original (unweighted) sample. The groups were of similar age and sex with small variations in terms of recent immigration status, income, comorbidity, and overall resource use. Those in the IPC group more frequently resided in a rural area and had fewer prior physician visits than counterparts in the non-IPC group. After weighting, the distribution of the propensity score and stabilized weights were well balanced between the 2 groups (Supplemental Figure 3) and the absolute standardized mean differences were negligible (Supplemental Figure 4).
Characteristics of the Study Population of People Newly Identified With Dementia in Ontario, by Group
During the year following dementia diagnosis, in the weighted sample, people with dementia in the IPC group had a 3% higher likelihood of making ED visits overall (relative risk [RR] = 1.03; 95% CI, 1.01-1.05) and a 22% higher likelihood of making nonurgent ED visits (RR = 1.22; 95% CI, 1.18-1.28) (Table 2). There was no evidence of an association between IPC and the likelihood of 1-year hospitalization overall (RR = 1.03; 95% CI, 1.00-1.06) or hospitalization for an ambulatory care–sensitive condition (RR = 1.06, 95% CI, 0.95-1.19).
ED Visits and Hospitalizations in the Year Following Dementia Ascertainment
In sensitivity analyses, the greater use of EDs by individuals in the IPC group was evident among urban residents but not among rural residents (Supplemental Table 1). The association between IPC and ED use persisted when the augmented set of confounders was used for propensity-score calibration in the subgroup who had had an assessment with the Resident Assessment Instrument for Home Care for long-stay home care services and/or a long-term care home placement (Supplemental Appendix). Finally, we found that an unmeasured confounder associated with both IPC and overall ED use with a relative risk of 1.21 or higher could explain away the estimated relative risk of 1.03 for ED visits in the main analysis (Supplemental Figure 2).
DISCUSSION
This study examined the association between enrollment in a practice using the IPC team model and acute care hospital use among people newly identified with dementia. We found that IPC was associated with greater overall and nonurgent ED use in the year following dementia diagnosis. No relationship was found between IPC and hospitalization outcomes.
Findings in Context
These results add to a scarce and mixed body of literature on the potential benefits of IPC over physician-only practices in older populations. We found ED use to be 3% higher for people with dementia cared for by an IPC team compared with those cared for by a non-IPC team, which, although statistically significant, may not represent a meaningful difference from a health system and clinical perspective. It may therefore be more in line with prior intervention studies in this population that found no evidence of an association between IPC and ED use; however, our study contrasts with other studies that found a modest decrease in ED visits with the interprofessional model of care.2,8,12,13,35 Our findings on hospitalization outcomes were consistent with those of previous intervention and population-based studies in populations that were older or had multimorbidity.2,12,13,36-38
Given the multifaceted needs of people with dementia, we hypothesized that access to IPC would be associated with decreased ED use. Several factors may explain the absence of evidence of this relationship in our study. First, it is possible that the observed increase in overall and nonurgent ED use was the result of an increase in appropriate ED use. Improved patient-centered care in IPC teams may have led to better patient or caregiver awareness of symptoms. Increased access to primary care may also have fueled demand for other unmet needs.39 This phenomenon, referred to elsewhere as supply-induced demand, has been observed in other evaluations of health reforms.40 Second, the observed overall association of IPC with hospital use for acute care among people with dementia in our study may not reflect the heterogeneity in the characteristics of IPC teams.41 Team functioning, colocation, and clinician continuity, which have been shown to be important predictors of health service use,38,42-47 may differ across IPC teams and may influence the degree or even direction of effect of IPC on patient outcomes. For people with dementia who see a wide range of professionals for their physical, cognitive, and social needs, clinician continuity of care may in fact be reduced within IPC teams compared with physician-only practices.38 A lack of clinician continuity may inadvertently lead to more fragmented care, impeding the establishment of therapeutic, trusting relationships in this population. Finally, IPC, without systematic training or support for dementia care, may not be sufficient to impact use of EDs and other health services at a population level.48 Studies showing IPC to be effective in improving dementia care and health service use have used dementia-specific interventions, including a nurse with training in geriatric or dementia care, a dementia care navigator, and/or support from cognition specialists.2,7,49 Although the IPC model in Ontario aimed to provide better prevention and management of a variety of chronic diseases, dementia might not have been prioritized among other chronic conditions, which might have led to a diminished effect of IPC for dementia. This possibility is consistent with literature citing the lack of consideration of dementia among chronic diseases in older adults.50
Future research should assess decision-making pathways leading to ED use among people with dementia. An examination of the influence of team characteristics in the relationship between IPC and health service use in this population may also help uncover the conditions under which IPC can be most effective. The extent to which dementia care, which relies primarily on management rather than therapeutic intervention, may be more present in team-based primary care models compared with physician-only models warrants further investigation, to quantify the added value of nonphysician team members to dementia care. Overall, the findings of our study highlight the need to bring dementia management to the forefront of chronic disease management in primary care.
Strengths and Limitations
There are notable strengths and limitations of our study. It used novel causal inference methods at both the design and analysis stage to minimize bias in the assessment of IPC among people with dementia and their health service use. For example, the choice of our comparator group and the elaboration of a directed acyclic graph informed by clinicians and others allowed a thorough assessment and control of potential sources of confounding. We also used novel and underused methods in causal inference such as propensity score calibration and the E-value to ascertain the robustness of our results. Nevertheless, heterogeneity in the IPC team characteristics was not considered and may have moderated the effect of IPC on the study outcomes. Another important limitation is the lack of nonphysician encounter data in the health administrative data. Such data would have allowed us to uncover the extent and type of services provided by nonphysician team members to people with dementia. Finally, although we made every effort to limit bias due to confounding in our analysis, the possibility of unmeasured confounding remains. Specifically, some confounders measured, such as residence and factors pertaining to socioeconomic status, were available only as either binary or quintile variables in part because of privacy requirements to ensure individuals could not be identified. These factors are known to be important predictors of team membership, and the availability of continuous data would have helped better correct for confounding. Other physician-related factors, such as years in practice, physician sociodemographic factors, or activities around collaboration, for which data were not available, may have also played a role in the management of patients and the rates of health service use.
Conclusion
In our study, IPC was associated with increased overall and nonurgent ED use. Although IPC may be well suited to manage the growing and complex dementia population, a better understanding of the optimal characteristics of team-based care and the reasons leading to hospital use for acute care by people with dementia is needed.
Acknowledgments
We would like to acknowledge Dr Howard Bergman for his insight on the interpretation and validation of results. We also sincerely thank Ms Kavita Metha, CEO of the Association of Family Health Teams of Ontario for her insight on the structure and functioning of Family Health Teams. We also acknowledge the assistance of Ms Mary Henein in formatting the tables and graphs in this manuscript as well as Ms Laura Maclagan for her support with ICES data–related queries and Ms Georgia Hacker for formatting the manuscript for submission. All people who have contributed substantially to this work have been listed as authors.
Footnotes
Conflicts of interest: authors report none.
Author contributions: Nadia Sourial made substantial contributions to the conception and design, analysis, interpretation of data, and the drafting, revisions, and final approval of the manuscript. Dr Sourial had full access to all the data in the study, conducted and was responsible for the data analysis, and takes responsibility for the integrity of the data and the accuracy of the data analysis. Tibor Schuster contributed to the conception and design, interpretation of data, revision, and final approval of the manuscript. Susan E. Bronskill contributed to the conception and design, interpretation of data, revision, and final approval of the manuscript. Claire Godard-Sebillotte contributed to the conception and design, interpretation of data, revision, and final approval of the manuscript. Jacob Etches contributed to the acquisition of data, analysis, interpretation of data, revision, and final approval of the manuscript. Isabelle Vedel contributed to the conception and design, interpretation of data, drafting, revision, and final approval of the manuscript.
Funding support: This work was funded through Canadian Institutes of Health Research (CIHR) Vanier Canada Graduate Scholarships. The Canadian Consortium on Neurodegeneration in Aging, which is supported by a grant from CIHR with funding from several partners (ID No. CNA-137794) also supported this work. This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and information compiled and provided by the Ontario MOH and MLTC, the Canadian Institute for Health Information, IMS Brogan Inc, and the Ontario Association of Community Care Access Centres.
Disclaimer: The analyses, conclusions, opinions, and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
Previous presentations: Some preliminary methods and preliminary results were presented at the following conferences: Society for Epidemiologic Research, June 18-21, 2019, Minneapolis, Minnesota; North American Primary Care Research Group meeting, November 16-20, 2019, Toronto, Ontario, and November 20-24, 2020 (virtual); Canadian Association for Health Services and Policy Research, May 29-31, 2019, Halifax, Nova Scotia, and 2020 (virtual); Canadian Consortium on Neurodegeneration in Aging, October 2019, Quebec; and Quebec Network for Research on Aging, October 2019, Montreal.
- Received for publication November 27, 2021.
- Revision received May 31, 2022.
- Accepted for publication June 20, 2022.
- © 2022 Annals of Family Medicine, Inc.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.