
Abstract
PURPOSE Primary care practices manage most patients with diabetes and face considerable operational, regulatory, and reimbursement pressures to improve the quality of this care. The Enhanced Primary Care Diabetes (EPCD) model was developed to leverage the expertise of care team nurses and pharmacists to improve diabetes care.
METHODS Using a retrospective, interrupted-time series design, we evaluated the EPCD model’s impact on D5, a publicly reported composite quality measure of diabetes care: glycemic control, blood pressure control, low-density lipoprotein control, tobacco abstinence, and aspirin use. We examined 32 primary care practices in an integrated health care system that cares for adults with diabetes; practices were categorized as staff clinician practices (having physicians and advanced practice providers) with access to EPCD (5,761 patients); resident physician practices with access to EPCD (1,887 patients); or staff clinician practices without access to EPCD (10,079 patients). The primary outcome was the percentage of patients meeting the D5 measure, compared between a 7-month preimplementation period and a 10-month postimplementation period.
RESULTS After EPCD implementation, staff clinician practices had a significant improvement in the percentage of patients meeting the D5 composite quality indicator (change in incident rate ratio from 0.995 to 1.005; P = .01). Trends in D5 attainment did not change significantly among the resident physician practices with access to EPCD (P = .14) and worsened among the staff clinician practices without access to EPCD (change in incident rate ratio from 1.001 to 0.994; P = .05).
CONCLUSIONS Implementation of the EPCD team model was associated with an improvement in diabetes care quality in the staff clinician group having access to this model. Further study of proactive, multidisciplinary chronic disease management led by care team nurses and integrating clinical pharmacists is warranted.
- chronic disease
- diabetes
- integrated health care delivery
- health care team
- nurse
- pharmacist
- quality of care
- organizational change
- practice-based research
INTRODUCTION
In the United States, 37.3 million people or 11.3% of the population were reported to be living with diabetes in 2020.1 With the continued increase in disease prevalence and high burden of multimorbidity that calls for comprehensive diabetes care, the majority of patients with diabetes are managed in the primary care setting.2,3 Primary care practices, particularly those operating within Accountable Care Organizations, are faced with mounting regulatory and financial pressures to improve diabetes care quality.4,5 Given the complexity of caring for patients with diabetes, the high and increasing workload in primary care practices,6 and urgent need to improve the quality of diabetes care,6,7 innovative care delivery models are needed to support comprehensive diabetes management in the primary care setting.8,9 Collaborative practice models, such as the Chronic Care Model, are endorsed by the American Diabetes Association to improve adherence to standards of care and deliver comprehensive patient-centered diabetes care.10,11 Implementation of collaborative care models is challenging, however, because of staffing and resource constraints in many primary care practices.
A wide range of programs and practice initiatives have been proposed to address the gaps in diabetes care processes and health outcomes. A meta-analysis of 66 trials evaluating 11 strategies for improving glycemic control found that team changes (adding team members, expanding team member roles, developing multidisciplinary teams) and case management (care in collaboration with or supplementary to the primary care clinician) produced the most robust improvements.12 Another systematic review found that interventions that increase nurse involvement in patient care are more likely to improve glycemic control, timely laboratory testing, and screening for complications.13 Consistent with this literature, multiple interventions that leverage nursing expertise have been implemented within the primary care setting, including diabetes-specific clinics,14 case management,15,16 use of nurse protocols for adjustment of diabetes medications,17 and multidisciplinary group visits.18
Despite the abundance of primary care interventions proposed to improve diabetes care quality, there is little guidance on how to implement these interventions without additional resources, specifically, how to realign existing primary care resources to deliver comprehensive diabetes care—not just achieve glycemic control—by empowering team members to practice at the top of their licensure and proactively engage highest-needs patients. We developed and implemented a comprehensive approach to diabetes management that is centered around care team nurses and activates, as needed, other members of the multidisciplinary care team. This nurse-led Enhanced Primary Care Diabetes (EPCD) model was designed to be implemented within existing team infrastructure without requiring incremental resources. We evaluated the impact of the EPCD among practices within an integrated health care delivery system that did or did not implement the model.
METHODS
Design
We retrospectively analyzed electronic health record (EHR) data from 32 practices—13 Mayo Clinic Rochester (MCR) practices and 19 Mayo Clinic Health System (MCHS) practices in Southeast Minnesota—using an interrupted-time series study design to evaluate the effectiveness of the EPCD model. This study was deemed exempt by the Mayo Clinic Institutional Review Board as it is focused on practice and quality improvement.
Setting
Mayo Clinic is an integrated health care delivery system serving local, regional, national, and international patients with a hub in Rochester, Minnesota. MCR includes practices in family medicine, internal medicine, and pediatrics, caring for more than 150,000 local residents, Mayo Clinic employees, and their dependents. Medical resident trainees in family medicine and internal medicine practice as part of separate care teams located in MCR (there are no residents in MCHS). MCHS is a regional network of community clinics throughout southeast and south-central Minnesota and northwest and southwest Wisconsin. In both MCR and MCHS, clinicians and their support staff are organized into care teams, and all patients are empaneled (assigned) to a physician, nurse practitioner, or physician assistant and that clinician’s care team. Both MCR and MCHS practices have access to endocrinology specialists in a referral practice. Panel management is conducted by the primary clinician with ad hoc support from other members of the clinical team.
EPCD Model and Study Groups
The EPCD model workflow has been previously described.19 A detailed explanation of the model’s development, workflow, and implementation is given in Supplemental Appendix 1. The process algorithm that nurses used to assess each patient and facilitate progress toward meeting the composite all-or-none 5-component diabetes quality indicator (the D5 indicator, described below) is detailed in Supplemental Appendix 2.
The EPCD model was first pilot tested in a single MCR clinic (a family medicine trainee practice), then implemented in a staggered fashion throughout the rest of MCR between March 1 and April 30, 2019. The order of implementation by individual clinics was voluntary and not based on D5 performance. Because trainee practices have different patient and care team continuity compared with staff clinician practices, we examined these 2 groups separately. The MCHS Southeast Minnesota practices did not implement the EPCD model until May 2021 and were examined as the comparator group.
The 32 included practices were thereby categorized into 3 groups. A total of 11 were EPCD staff clinician practices (those having physicians and advanced practice providers with access to the model); 2 were EPCD trainee practices (those having resident physicians with access to the model); and 19 were non-EPCD staff clinician practices (those having physicians and advanced practice providers without access to the model).
Independent Variables
Baseline patient characteristics of the study practices were ascertained from the EHR and included patient age, sex, race, ethnicity, English proficiency, and diabetes type. English proficiency was established using a flag in the EHR specifying patient preference for having an interpreter available during medical appointments. Diabetes type was established using International Diagnosis Codes present in the EHR problem list. Patient race and ethnicity were ascertained from the EHR based on patient self-report at the time of registration.
Outcomes
The primary outcome was the composite all-or-none D5 quality indicator of diabetes care, which is publicly reported by all health care practices in the state through Minnesota Community Measurement for patients aged 18 to 75 years.20,21 The indicator consists of targets for glycated hemoglobin (HbA1c), blood pressure, and low-density lipoprotein cholesterol (with statin use if indicated); aspirin use if indicated; and tobacco-free status (Supplemental Appendix 1); all 5 components must be met. Patients missing data for a component, such as those not having an HbA1c value available during the measurement year, were classified as not meeting that indicator.
Secondary outcomes were the individual components of the D5 indicator. For the 2 groups having access to the EPCD, we also quantified the percentage of empaneled patients who had an episode of care started by the nurse, indicating that the patient was officially touched by the EPCD program.
Statistical Analysis
We calculated overall frequencies (percentages) and means with SDs for baseline patient characteristics. Practice performance on the D5 indicator was ascertained on the first day of each month from an EHR report. Indicator data were assessed monthly for a 7-month preimplementation period (August 1, 2018 through February 1, 2019) and a 10-month postimplementation period (May 1, 2019 through March 1, 2020). We used Poisson regression analysis for the interrupted-time series analyses to estimate preimplementation and postimplementation trends, the change in the percentage of patients meeting the given criterion at the time of EPCD implementation, and the change in slope from preimplementation to postimplementation.22 All analyses were performed using R version 4.0.3 (R Foundation for Statistical Computing), and 2-sided P values <.05 were considered statistically significant.
RESULTS
Patient Characteristics
As of May 1, 2019, there were 5,761 eligible patients empaneled to the EPCD staff practices, 1,887 to the EPCD trainee practices, and 10,079 to the non-EPCD staff practices. Table 1 summarizes patient characteristics for the 3 groups at the time of EPCD implementation. During the postimplementation period, the percentage of empaneled patients formally touched by the staff or trainee EPCD programs increased steadily from 2.8% to 9.2%.
Patient Characteristics by Practice Group
Trends Within Groups
Within-group results are summarized in Table 2. At the beginning of the preimplementation period, more patients met the D5 composite indicator as well as the individual component indicators of glycemic (HbA1c) control, blood pressure control, and tobacco abstinence in the EPCD staff group.
Summary of Patients Meeting Diabetes Quality Indicators by EPCD Period
During the preimplementation period, there was no significant change in patients meeting the D5 composite indicator in any group, although all 3 groups had a significant downward trend in the percentage of patients meeting the blood pressure indicator.
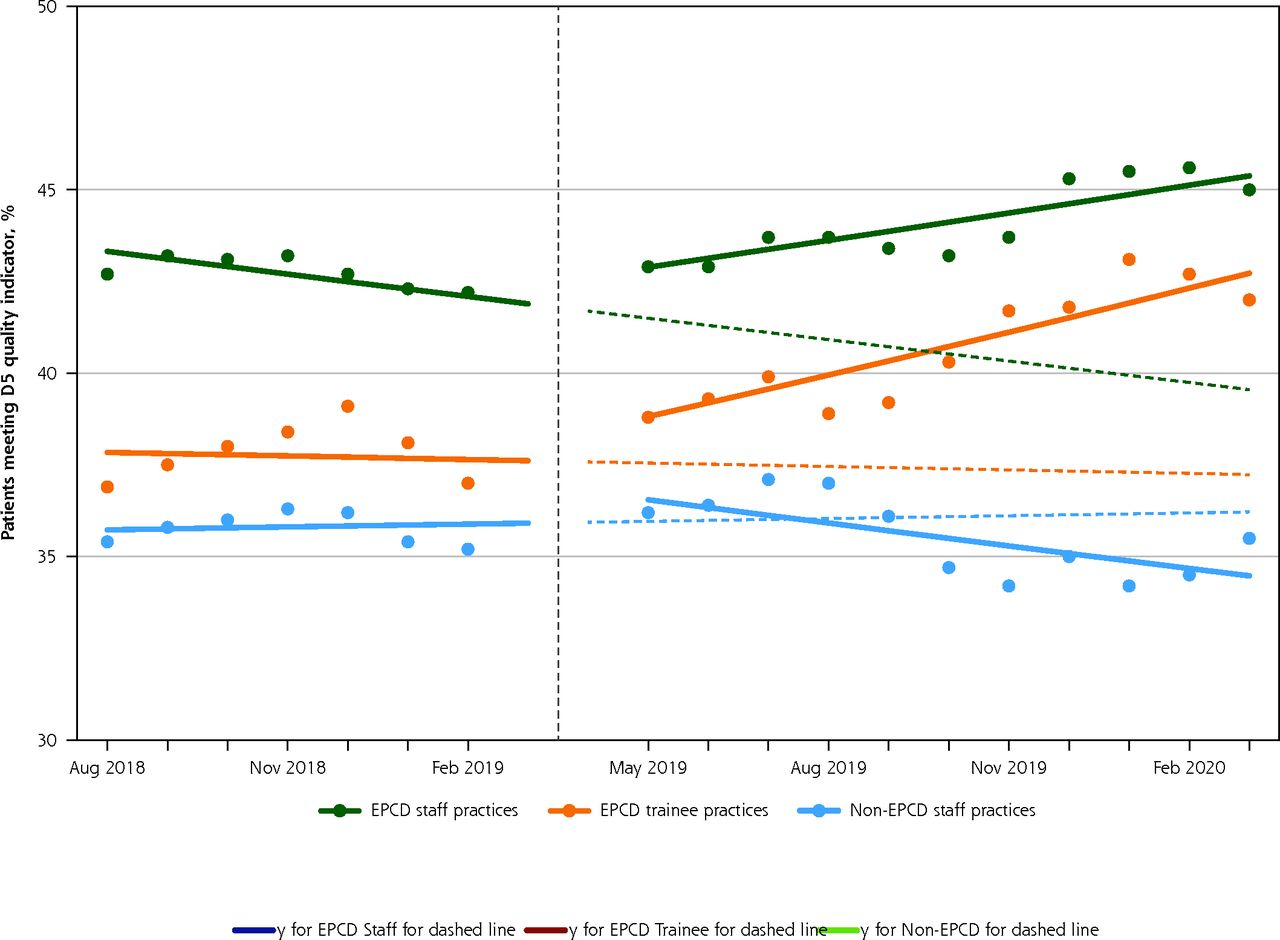
During the postimplementation period, the proportion of patients meeting the D5 indicator increased from 42.9% to 45.0% (incident rate ratio [IRR] = 1.005; P = .001) in the EPCD staff group and increased from 38.9% to 42.0% (IRR = 1.011; P = .003) in the EPCD trainee group, but decreased from 36.2% to 35.5% (IRR = 0.994; P < .001) in the non-EPCD staff group. The percentage of patients meeting the glycemic control indicator decreased in the non-EPCD group, while the percentage meeting the blood pressure indicator increased in both EPCD groups.
When comparing the preimplementation trend with the postimplementation trend, there was a significant improvement in attainment of the D5 composite indicator in the EPCD staff group (change in IRR from 0.995 to 1.005; P = .01) (Figure 1). No significant change was seen in the EPCD trainee and non-EPCD groups. The change in trend from preimplementation to postimplementation in the blood pressure indicator showed improvement in all 3 groups, but it was more pronounced in the EPCD groups than in the non-EPCD group. The non-EPCD group had a trend toward worsening of both the glycemic control and tobacco-free indicators.
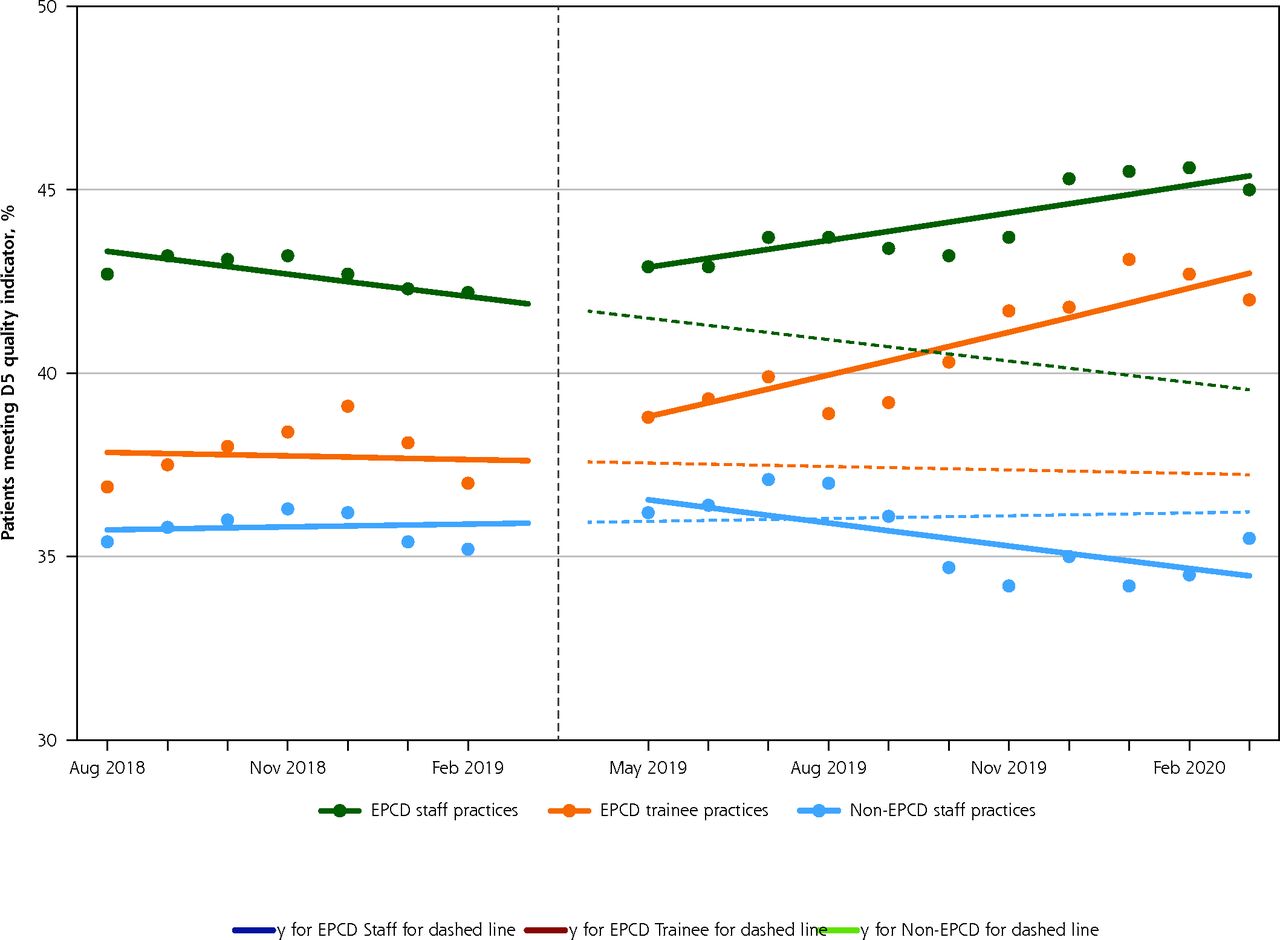
Percentage of eligible patients meeting the D5 quality indicator during the study period, by group.
D5 = all 5 diabetes components (glycemic control, blood pressure control, low-density lipoprotein cholesterol control, aspirin use if indicated, and tobacco-free status); EPCD = Enhanced Primary Care Diabetes.
Note: Dashed vertical line denotes transition from preimplementation period to postimplementation period. Solid colored lines show actual trends. Dashed colored lines show projection of preimplementation trends into postimplementation period for comparison.
Direct Comparisons Between Groups
When the groups were directly compared, there were no significant differences in the preimplementation trends in the D5 indicator (Table 3). Postimplementation, there was a positive trend in the percentage of patients meeting the indicator in the EPCD staff group compared with the non-EPCD group (IRR = 1.013; P < .001) and the EPCD trainee group compared with the non-EPCD group (IRR = 1.017; P < .001). Results were similar in the direct preimplementation-to-postimplementation analysis, with a positive trend for the D5 indicator in the EPCD staff group and EPCD trainee group compared with the non-EPCD group (IRR = 0.017; P < .001 and IRR = 0.017; P = .03, respectively).
Direct Comparison of Groups on Patients Meeting D5 Quality Indicator
DISCUSSION
Improving the quality of diabetes care is a high priority for patients, health systems, and society. With the greatest burden of diabetes management falling on primary care practices, effective, efficient, and sustainable care delivery models to support optimal diabetes care in the primary care setting are urgently needed. Herein, we describe an analysis of the EPCD model, which is led by care team nurses without the addition of incremental resources. At a time when patients cared for with the usual care approach saw a decline in their diabetes care quality, patients in the EPCD staff practices saw significant improvements and patients in the EPCD trainee practices were able to reverse their prior decline and remain stable. Importantly, the EPCD model promotes and facilitates comprehensive diabetes care beyond glycemic control alone.
Several factors likely underlie the improvements in diabetes care quality seen with implementation of the EPCD model. Proactive care delivery was enabled by the care team nurses who used population health tools within the EHR to identify and engage patients not meeting goals and initiate the EPCD algorithm, rather than reactively relying on patient presence in the clinic. Panel management meetings between the nurse and primary care clinician allowed for synchronous discussion and strategizing on patients not moving toward quality goals, while asynchronous communication prompted by nurse record review and patient contact allowed for real-time improvements. More consistent engagement with patients outside of office visits and among the care team members helped keep all parties motivated and accountable. The EPCD model also promoted multidisciplinary care with the use of decision support tools for nurses enabling them to consult or engage other team members in the patient’s care based on clinical scenario. These team members included clinical pharmacists,23 who were consulted for expert recommendations, reducing the probability of therapeutic inertia. The addition of a pharmacist to the care team has been beneficial in other large health care organizations such as Kaiser Permanente and the Veterans Affairs,24,25 and our work demonstrates how pharmacists can be leveraged through asynchronous communication outside of scheduled visits. On the basis of the improvement in the composite D5 indicator attainment in the EPCD staff practices without increasing incremental resources, we hypothesize that care team nurses, with the trust of a primary care clinician, can effectively manage diabetes panels.
In contrast to the EPCD staff practices, the EPCD trainee practices did not significantly improve on the D5 composite indicator after EPCD implementation, although the previously observed decline in this indicator over time was reversed and care quality stabilized. We hypothesize this pattern may have been due to the schedule of trainee primary care clinicians, with inconsistent availability on the floor and only 3 years’ practice time, which makes fostering a collaborative care team model challenging. These clinics may need to further leverage care team resources, such as clinical pharmacists, to help manage patients when trainees rotate out of the clinic. Importantly, the non-EPCD staff practices were increasingly less likely to meet the D5 goal during the postimplementation period, with a persistent decline in D5 attainment over time. We are not aware of any unique practice challenges impacting MCHS after EPCD implementation in MCR that would explain this finding. All primary care practices in MCR and MCHS experienced shortages of staff, particularly of nursing staff, during the study period, which further underscored the importance of thoughtful care team redesign to improve care quality without incremental resource allocation.
Changes in attainment of several of the D5 component indicators deserve individual attention. All 3 groups saw a negative trend in patients attaining blood pressure control preimplementation, which improved significantly during the postimplementation period. This shift was likely due to focused attention on hypertension across all sites as a separate Accountable Care Organization measure during the postimplementation period outside the EPCD initiative. Still, the improvement was most pronounced in the EPCD groups, reinforcing the model’s success. High baseline rates of patients meeting the low-density lipoprotein cholesterol, aspirin, and tobacco abstinence indicators may have limited the opportunity for improvement and dampened the urgency of addressing those metrics by the EPCD practices. The glycemic control indicator worsened in the non-EPCD group, while the EPCD groups saw a nonsignificant increasing trend going from the preimplementation period to the postimplementation period. This trend may have represented the beginning of a meaningful change in the EPCD groups limited by a lack of adequate time to modify the HbA1c level, which is measured only every 3 months in patients not meeting glycemic goals.
The EPCD model is distinguished from previously published nurse-led primary care models for diabetes management in several important ways. First, although the EPCD model is led by nurses, it is team-centered and multidisciplinary, allowing all members of the primary care team to work cohesively and in real time to meet the patients’ needs. Second, our focus was on addressing all components of the D5 indicator, and not glycemic control alone as is the focus of many diabetes quality improvement programs.13,26 Our study is further strengthened by the inclusion of a large population of patients cared for within 32 internal medicine and family medicine practices, with both staff and trainee clinicians, in both urban and rural areas. Included clinics ranged widely in their size and resource availability, increasing the generalizability of our findings. Our analytic approach allowed us to examine the impacts of an institutional improvement effort to address gaps in diabetes care quality that are widespread. The EPCD model itself is generalizable, efficient, and effective, and can serve as a framework for other primary care practices seeking to improve the management of diabetes.
Our study also has several limitations. The COVID-19 pandemic shifted organizational focus and primary care targets away from chronic disease management, leading us to stop our analyses in March 2020 (10 months after EPCD program implementation). By that time, only 9.2% of patients had been formally evaluated by a nurse; we expect that as more patients are touched by the EPCD model, their attainment of the D5 indicator will similarly improve. We plan to reexamine model effectiveness in all primary care practices across Southeast Minnesota MCHS in 2023, as the model was scaled to the non-EPCD practices in 2021. All clinics are part of a single integrated health care system in the upper Midwest; as such, the health care delivery practices and patients served may not generalize to more urban areas in the United States. Yet, this homogeneity allowed for the comparative interrupted-time series analyses that would not have otherwise been possible. Our analyses also did not adjust for granular patient-level information such as socioeconomic status and multimorbidity because our objective was to assess the impact on population-level care quality and because our analytic data set—obtained from an EHR report—did not include this information. Some of these differences may be clinically relevant; however, they do not clearly favor any one group. Although the risk of confounding exists in all observational study designs, the interrupted-time series study design reduced the likelihood of confounding of results by differences in patient characteristics among groups.27-29 We are unaware of other concurrent large-scale initiatives to improve diabetes care in the population, but smaller local initiatives at any site may have also influenced our findings.
In conclusion, the EPCD model, which leverages the expertise of nurses, pharmacists, and other members of the multidisciplinary care team, and does not require new resources, provides a successful template that health care systems can build on to improve the quality of diabetes care they provide to patients.
Footnotes
Conflicts of interest: In the last 36 months, Dr McCoy has received research support from NIDDK, PCORI, and AARP. She has also received speaking honoraria from the American Diabetes Association and served as a consultant to Emmi (Wolters Kluwer) on developing patient-facing educational materials related to diabetes. The other authors report no conflicts of interest.
Funding support: J.R.H. received internal funding from the Mayo Midwest Pharmacy Research Committee for research time and data retrieval services. R.G.M. is funded by the National Institutes of Health (NIH), National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) grant number K23DK114497.
Disclaimer: The views expressed are solely those of the authors and do not necessarily represent official views of the authors’ affiliated institutions or funders.
- Received for publication January 4, 2022.
- Revision received April 27, 2022.
- Accepted for publication June 15, 2022.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}