
Abstract
PURPOSE The effective integration of primary care into public health responses to the COVID-19 pandemic, particularly through data sharing, has received some attention in the literature. However, the specific policies and structures that facilitate this integration are understudied. This paper describes the experiences of clinicians and administrators in Alberta, Canada as they built a data bridge between primary care and public health to improve the province’s community-based response to the pandemic.
METHODS Fifty-seven semistructured qualitative interviews were conducted with a range of primary care and public health stakeholders working inside the Calgary Health Zone. Interpretive description was used to analyze the interviews.
RESULTS SARS-CoV-2 test results produced by the local public laboratory were, initially, only available to central public health clinicians and not independent primary care physicians. This enabled centrally managed contact tracing but meant primary care physicians were unaware of their patients’ COVID-19 status and unable to offer in-community follow-up care. Stakeholders from both central public health and independent primary care were able to leverage a policy commitment to the Patient Medical Home (PMH) care model, and a range of existing organizational structures, and governance arrangements to create a data bridge that would span the gap.
CONCLUSIONS Primary care systems looking to draw lessons from the data bridge’s construction may consider ways to: leverage care model commitments to integration and adjust or create organization and governance structures which actively draw together primary care and non–primary care stakeholders to work on common projects. Such policies and structures develop trusting relationships, open the possibility for champions to emerge, and create the spaces in which integrative improvisation can take place.
INTRODUCTION
The vast majority of COVID-19 cases and their “long COVID” sequalae1,2 have been managed in the community by primary care teams.3,4 As much as those primary care teams have been central to delivering in-community care, maintaining health system resilience5 by mitigating the overburdening of emergency and acute care facilities,4,6 supporting key public health initiatives,7,8 and delivering vaccine counselling and vaccinations,9-11 their experiences of integration into the pandemic response are not well understood. This paper provides rich descriptions of a particular integration moment in Alberta, Canada. It describes the policies, structures, and governance arrangements that supported the construction of a data bridge between independent primary care and central public health in the early stages of the pandemic.
With an eye on achieving universal health care and sustainable development, the World Health Organization has emphasized the importance of integrating primary care into broader health systems.12,13 Integration in primary care aims to bring together a diverse group of individuals and professionals to provide care to those with complex health needs while eliminating duplication or gaps in service.14,15 It may occur at micro (ie, clinical), meso (ie, professional and organizational), or macro (ie, system) levels,16 and is less a discrete concept, and more an emerging set of practices.15
In the particular case of primary care integrating with public health, commitments to collaboration, mutual empowerment, and shared accountability have been shown to enable more effective services than what might be achieved by primary care or public health acting alone.17,18,19 Further, the literature suggests effective data sharing20 and inter-sectoral coordination3,4,21 are key factors in achieving successful integration. However, under pandemic conditions, jurisdictions worldwide encountered significant challenges as they attempted to integrate primary care into their COVID-19 responses generally,3,4,22 and public health operations specifically.23-27
In this paper we present broadly applicable lessons in achieving meso-level integration. Our focus is on the policies, structures, and governance arrangements that allowed stakeholders to build a data bridge between primary care and public health under pandemic conditions. We show how the data bridge was built on the foundations of: (1) the patient medical home (PMH) care model and other integration-focused policy mandates; (2) existing organizational structures that drew otherwise siloed stakeholders together to work on integration projects, and (3) governance arrangements that created the relationships and spaces where improvisation could happen.
To describe these foundations, and so draw out generalizable lessons about achieving integration, we draw on qualitative interviews with, on the one hand, independent-contractor primary care physicians and their affiliated primary care networks (PCNs), and, on the other hand, administrators and physicians from Alberta Health Services’ (AHS) public health unit in the Calgary Zone.
Alberta’s Primary Care Context
Primary care in Alberta is financed directly by the provincial ministry of health (MoH) with most care delivered by independent family physicians who bill the government on a fee-for-service (FFS) basis. Alongside this independent FFS model of primary care delivery, the province operates the largest centralized health care system in Canada, with over 650 facilities managed by a single health authority: AHS. Alberta Health Services delivers care in 5 geographically based “health zones,” with facilities in these zones providing acute, long-term, and some urgent care.
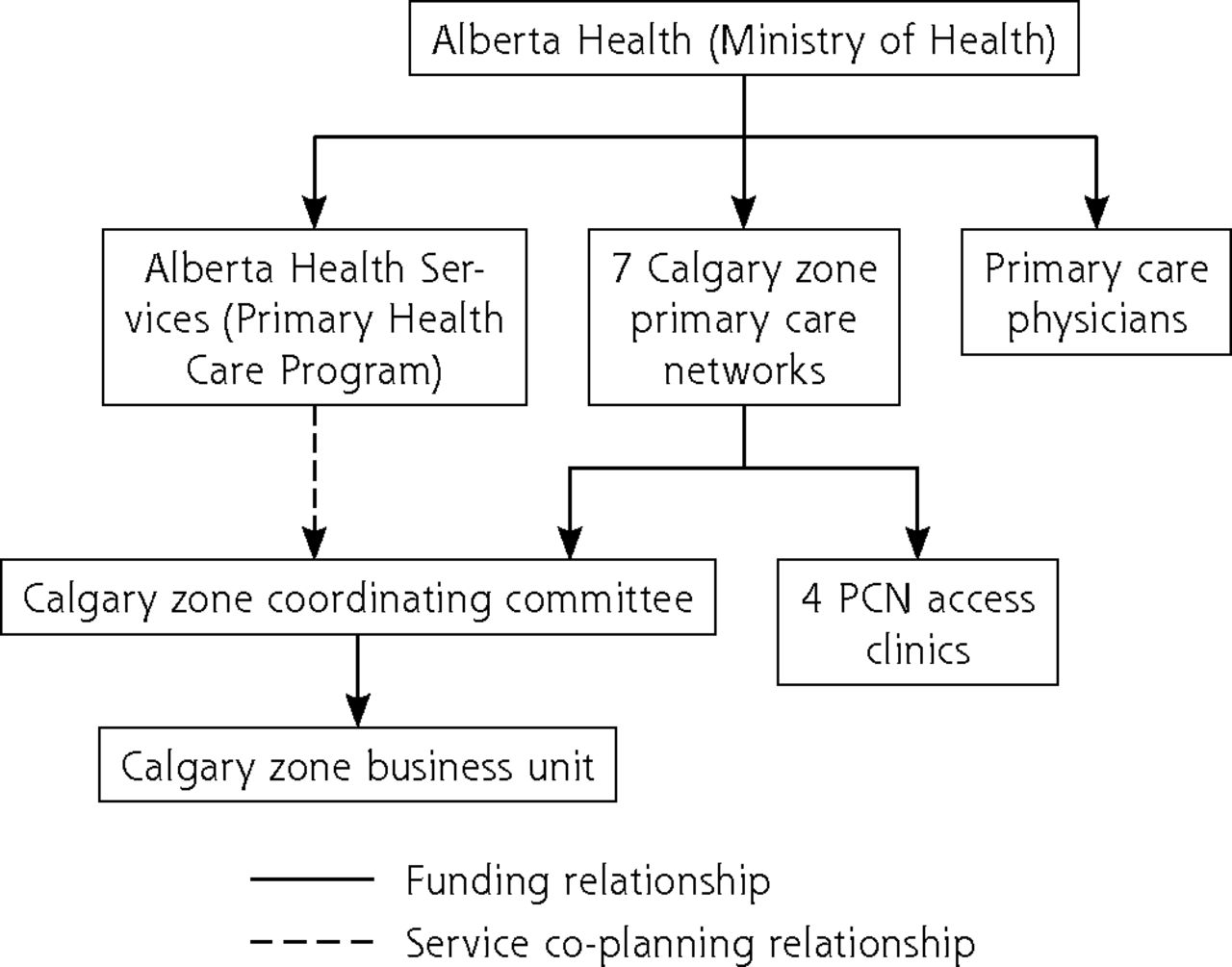
While primary care is a highly independent element of the province’s broader system, there are also significant links between it and AHS. A primary care–focused unit inside AHS (Primary Health Care Program, Figure 1) is devoted to coordinating, at provincial and zonal levels, the integration of independent primary care into the operations of the broader system. Indeed, integration of the 2 elements is a provincial policy objective,28 with the PCNs positioned as key linkage points.

Primary care organization in Alberta.
PCN = primary care network.
The PCNs have evolved into their present form over the last 2 decades29 and are composed of independent primary care physicians who opt in to become members. If the PCNs’ overarching goal is to improve, and better coordinate, patients’ access to primary health care, they also operate under specific policy mandates to deliver the PMH model of care, and ensure all Albertans are attached to a primary care physician.28 Each PCN is made up of groups of family doctors and other health providers, such as nurses, dietitians, and pharmacists, who work together with AHS to tailor and deliver services to patients.
The particular mix of programming offered by any given PCN as it pursues its care model and attachment mandates is determined at health zone level sessions. The Calgary Zone Coordinating Committee is the governing body that convenes these service co-planning meetings, with attendees from AHS, primary care, and public health, among other central system stakeholders, coming together to assess the needs of patients and populations in their zone. All of the stakeholders at the service co-planning meetings are funded by the provincial government, and so are subject to the broad policy mandates described above. In this way, the MoH does not, directly, participate in local planning but rather sets policy centrally.
The 7 PCNs in the Calgary Zone (formed by 1,700 physician members working in 450 clinics and serving a population of over 1.4 million across urban and rural communities) have elected to coordinate and execute their zone level operations through a jointly funded zone business unit (ZBU). The ZBU collects and coordinates improvement projects that touch processes and clinical activity across the 7 PCNs.
For further background on the COVID-19 pandemic in Alberta, please see Supplemental Appendix 1.25,30,31
METHODS
The qualitative data presented here are drawn from a broader research project that deployed a mixed-methods, concurrent triangulation study design. We explain in detail this design and the particular approaches taken to gather the qualitative data quoted in support of our analysis in Supplemental Appendix 2.32-34 In summary, we conducted 57 semistructured interviews using an interview guide (Supplemental Appendix 3) with participants from a range of Calgary Zone primary care organizations between January and March of 2021 (Table 1). The interviews were transcribed and subject to an interpretive description analysis.34
Study Participants
RESULTS
Building the Data Bridge
A PCN-based participant (See Quote 1 in Table 2 [Q1T2]) described the early evolution of how SARS-CoV-2 test results were handled in AHS public health and eventually shared with independent primary care.
Quotes From Qualitative Interviews
The PCN stakeholder’s account highlights key elements in the central public health, and independent primary care response, to the first wave in the Calgary Zone. The Zone’s AHS-based public health officer received test results from the provincial laboratory and leveraged an AHS-PC facility to begin managing COVID-19 patients in the community. In a separate step, the zone PCNs re-tasked their access clinics, positioning them to become bridges from the central testing system into the patient panels of independent community-based primary care physicians. This was consistent with the PCNs’ policy mandate to deliver the PMH and attach patients to primary care physicians. As such, the access clinics—which had been set up before the pandemic to attach patients—came to be seen as a “natural” place to conduct not just that work, but the work of notifying primary care physicians that their patients had tested positive; and caring for patients who did not want to be, or could not be, attached to a primary care physician, or whose physician was unavailable. PCN resources, in the form of information technology development time, were devoted not just to automating the manual efforts of the staff at the AHS PC facility, but to turning the first wave of the pandemic into an opportunity to attach patients and deliver wraparound care within the PMH. In this way the care model and related policy mandates set some of the conditions for the construction of the data bridge.
Indeed, the PCN stakeholder’s account provides glimpses of the data bridge being built, and so of public health and primary care integration happening in real-time under pandemic conditions. Another PCN stakeholder (Q2T2) described achieving “information continuity” as not “that hard to do” and in doing so downplayed the technical complexity of building the data bridge. At least from their perspective, it was not that hard to program; however, outside of the programming there was important non-technical, social activity that enabled the technical work to occur. For information continuity to be prioritized—an outcome which appeared obvious to participants in retrospect—ongoing, silo-linking conversations among end users, technology developers, and managers needed to occur while the first wave of the pandemic was hitting. As we will show, those conversations needed a well-placed champion, and to be open and trusting—rather than closed and focused on command and control—so that improvisational ideas on how to achieve continuity could emerge. Specific relationships, organizational structures (ie, existing integration-focused working committees) and governance arrangements (the Calgary Zone Coordinating Committee and ZBU) facilitated those improvisational conversations.
Integration Mechanisms: Relationships
Long-term trusted relationships and the specific backgrounds of key stakeholders were essential in the construction of the data bridge. As one AHS-based participant described it, the stakeholders did not just know one another, they trusted one another and could work together (Q3T2). Another AHS stakeholder explained how years of working together had created familiarity and trust (Q4T2).
If there was a general state of trust and possibility in the relationships shared by Calgary Zone AHS personnel and the PCNs, the specific profile of the AHS-public health officer who instigated the initial sharing of the lists was a key element in creating these conditions for improvisation and integration.
That officer was cross trained in both public health and family medicine, and as such was able to see and advocate inside the central public health apparatus for integration. A PCN stakeholder described how the officer was the 1 person inside the central public health unit who understood what independent primary care meant when it raised concerns about community management of COVID-19 that went beyond contact tracing. At those meetings primary care stakeholders would counter public health’s assumption that COVID-19 test results were primarily about notification and contact tracing, asking pointed questions about how those who tested positive were going to be managed medically and kept out of hospital (Q5T2).
Beyond their ability to see the need for more than contact tracing, the public health officer had, since arriving years before in the Calgary Zone, established a more local focus than their predecessors. A PCN leader described the public health officer’s local focus on, and championing of, primary care as instrumental in achieving integration (Q6T2).
The public health officer’s long-term focus on relationships set the conditions for the data bridge to be built. Pre-existing mutual understandings, respect, and trust among primary care and public health stakeholders were the foundations on which the public health officer could successfully advocate for greater integration generally and the successfully improvised construction of the data bridge specifically.
Integration Mechanisms: Organizational Structures
A range of organizational structures further supported the relationships described above and the integration of primary care into the public health response. Task groups set up by the Zone Coordinating Committee to pursue a range of projects moved stakeholders from merely knowing one another to working closely with one another on issues directly related to the integration of independent primary care into the central health system. Specifically, 3 task groups had been formed 7 years before the pandemic and were devoted to: (1) supporting transitions from acute to community care; (2) improving primary care integration with specialist physicians; and (3) optimizing delivery of the PMH model.
In the course of their work, each task group had already identified systems integration challenges, and each was working together with AHS to find innovative solutions. With the arrival of the pandemic, the task group engaged with supporting better transitions had a unique opportunity to leverage their existing efforts. Specifically, they were already working on how to automate notification processes so that independent primary care clinics would be aware a patient of theirs had been admitted or discharged from a centrally managed acute care facility.
While it took “years for this project” as 1 PCN stakeholder stated, all the trust, processes, and outcomes from it quickly pivoted toward facilitating the data bridge. An information technologist embedded in one of the PCNs who had worked on the previous project described how the pivot even felt “straightforward” (Q7T2).
They emphasized how an ongoing integration project made both the people and data operations of the central system familiar. With this familiarity, trust, and shared activity in place, the pivot to building a data bridge between public health laboratory data (rather than acute care admission/discharge data) and primary care was a straightforward transition.
Integration Mechanisms: Governance Arrangements
If the 3 integration-focused task groups were able to pivot rapidly toward building the data bridge, both the coordinating committee that convened those task groups in the first place, and the Calgary Zone PCNs’ choice to create a Zone Business Unit were also a key mechanisms of integration. These 2 governance arrangements, which intermingle medical and administrative elements, meant a broad range of stakeholders from across the Zone already had years of experience harmonizing action and communications between independent primary care and the central system. The structure in which they operated was repeatedly described as a key enabler of the data bridge specifically, and health system integration more generally (Q8T2).
When, in interviews, the coordinating structure broadly, and its decision-making capacity specifically, were identified as foundational to the data bridge, stakeholders singled out the ZBU as a particularly important element. An AHS stakeholder described how the ZBU had moved integration work off the sides of people’s desks into the center of activity (Q9T2).
Beyond expediting work that might otherwise have fallen to leaders to do in their spare time, the ZBU provided clear, concise communication, allowing local teams to quickly add relevant information.
DISCUSSION
The challenge engaged by the participants in our research—how to ensure SARS-CoV-2 test results generated in public health were shared with PC and used to provide follow-up care in the community—is an integration issue identified across the literature. Strong health information systems are critical to mounting an effective pandemic response generally7,35 and supporting the infection surveillance capacity of PC specifically.3,4,6,20,21,26,36 The ability to share patient data is particularly critical under circumstances where virus testing is conducted outside of primary care practice.7 Earlier studies of the 2009 H1N1 pandemic have highlighted the importance of primary care and public health sharing protocols, information, and records in a timely manner if an effective response is to be mounted.18,37 More recently, studies have shown that without information sharing, coordination, and collaboration, a successful pandemic response is out of grasp, and patients may be harmed.19,38 As such, the Calgary Zone’s efforts to bridge the divide between centrally managed public health testing and community-based primary care delivery was an example of a key integration moment in the response to the COVID-19 pandemic.
The context surrounding the information technology challenges of building the data bridge included policy, organizational, and governance elements. These elements made the bridge’s construction appear “straightforward” to some participants. On the one hand, these assessments obscure complex and intense work, and on the other, they direct attention toward how organizational and policy histories set the possibilities for chance, improvisation, and integration.
Policies seeking the attachment of patients to primary care, and directing the delivery of the PMH,29 set the conditions for the Calgary Zone’s Access Clinics to “naturally” transition to support the clinical work that the data bridge would enable. Similarly, task groups that had long drawn disparate stakeholders together to work on integration projects meant the pivot to programming the data bridge appeared “not that hard.” The Calgary Zone’s governance arrangements—it’s coordinating committee and ZBU—created a space where not only trusting relationships could be formed, but where chance could play out in integration’s favor. A public health officer turned out, by chance, to be PC trained and an advocate for PC’s in-community COVID-19 management capacity. Successfully adapting to this chance, and the many others introduced by the pandemic, required improvisation. That improvisation was carried out on the foundations set by integration-focus policies, organizational structures, and governance arrangements.
Those in other systems interested in drawing lessons from the data bridge’s construction will profitably turn their attention to creating or adjusting policies that mandate not just specific models of primary care–focused care—like the PMH—but working structures and governance arrangements that actively draw together primary care and non–primary care stakeholders. In this sense, policies and the structures they create—from PCNs, to the ZBU, to informatics working groups—are first and foremost opportunities for interaction. Those policy-induced interactions merge professional and technical siloes, allowing for the expression of the core collaborative and trust values that underpin successful integration.17 A combination of chance and judicious planning in the selection of the substantive work that the interacting groups of primary care and non–primary care stakeholders undertake can then allow for a more or less “straightforward” pivot toward meeting emergent pandemic needs.
Our findings here on the importance of governance structures in pandemic integration are aligned with other Canadian research showing that, without a functional and well-established interface between independent PC and the central health system, both pandemic responses, and everyday primary care integration efforts, are likely to suffer.5,38 In the Calgary Zone, the PCNs and their ZBU provided exactly this interface, supporting robust bi-directional communication that facilitated improvisation under pandemic conditions as well as driving sustainable PC integration under “normal” conditions. Future cross comparative research is required to understand how best to create policies, structures, and governance arrangements that allow for interaction between primary care and public health, and also forms of co-planning that provide openness to chance and improvisation.
The study’s recruitment response rate was robust, with just over 20% of the individuals identified to participate in this study (17/79), not responding to the e-mail invitation. A plausible reason for this was that interviews took place during the second COVID-19 wave, and there was a high degree of COVID-19 fatigue. As with all qualitative work, we offer a cross-sectional analysis of a particular moment in time with our research. Data collection for this project began during Alberta’s second wave, and data collection processes in the Calgary Zone were continuously being updated while we were conducting interviews.
CONCLUSIONS
The COVID-19 pandemic has emphasized the importance of integrating primary care and public health, generally, and in the sharing of data between the 2 health system elements particularly. Describing the efforts of stakeholders from both primary care and public health in Alberta, Canada as they pivoted to build a data-sharing bridge during the COVID-19 pandemic, we have identified a constellation of care model, policy, structural, and governance elements that, when aligned toward integration, are foundational for this kind of work. Our data suggest the speed and relative ease with which such a bridge can be erected are strongly influenced by this constellation of elements. Jurisdictions planning for the future may wish to consider ways to: leverage care model commitments to integration, and adjust or create working structures and governance arrangements that actively draw together primary care and non–primary care stakeholders and in doing so open the possibility for champions to emerge, trust to evolve, and integrative improvisation to take place.
Acknowledgments
This research was supported by the Foundation for Advancing Family Medicine, under the COVID-19 Pandemic Response and Impact Grant (Co-RIG) phase 1 program. The authors would like to thank the anonymous participants for their time and perspectives given, as they were, under the fraught conditions of the pandemic.
Footnotes
Conflicts of interest: authors report none.
Funding support: Foundation for Advancing Family Medicine, COVID-19 Pandemic Response and Impact Grant (Co-RIG) phase 1 program.
- Received for publication December 14, 2021.
- Revision received September 16, 2022.
- Accepted for publication September 20, 2022.
- © 2023 Annals of Family Medicine, Inc.




{kind=link}