
Article Figures & Data
Figures
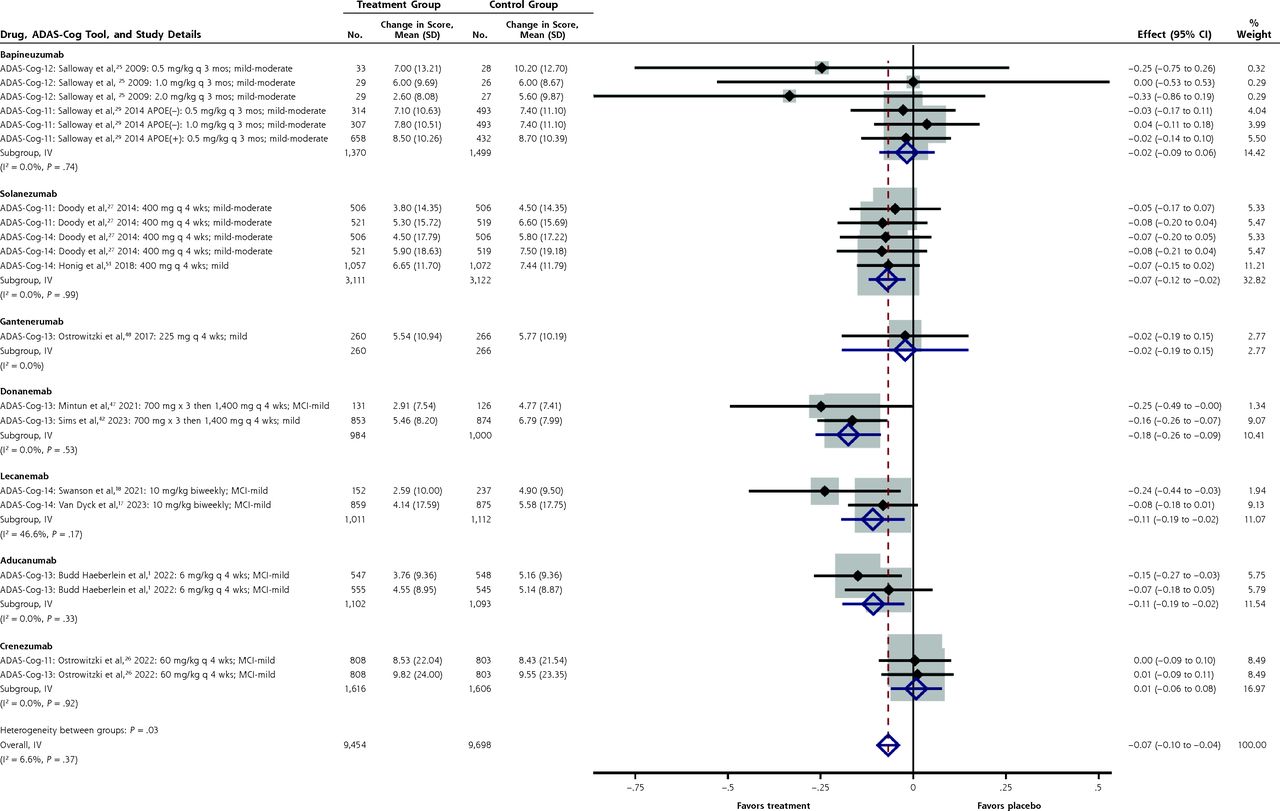
- Figure 1.
Forest plot for the standardized mean differences in ADAS-Cog-11 through ADAS-Cog-14 scores.
ADAS-Cog-11 = Alzheimer’s Disease Assessment Scale–Cognitive Subscale-11 items; ADAS-Cog-12 = Alzheimer’s Disease Assessment Scale–Cognitive Subscale-12 items; ADAS-Cog-13 = Alzheimer’s Disease Assessment Scale–Cognitive Subscale-13 items; ADAS-Cog-14 = Alzheimer’s Disease Assessment Scale–Cognitive Subscale-14 items; IV =interstudy variance; MCI = mild cognitive impairment.
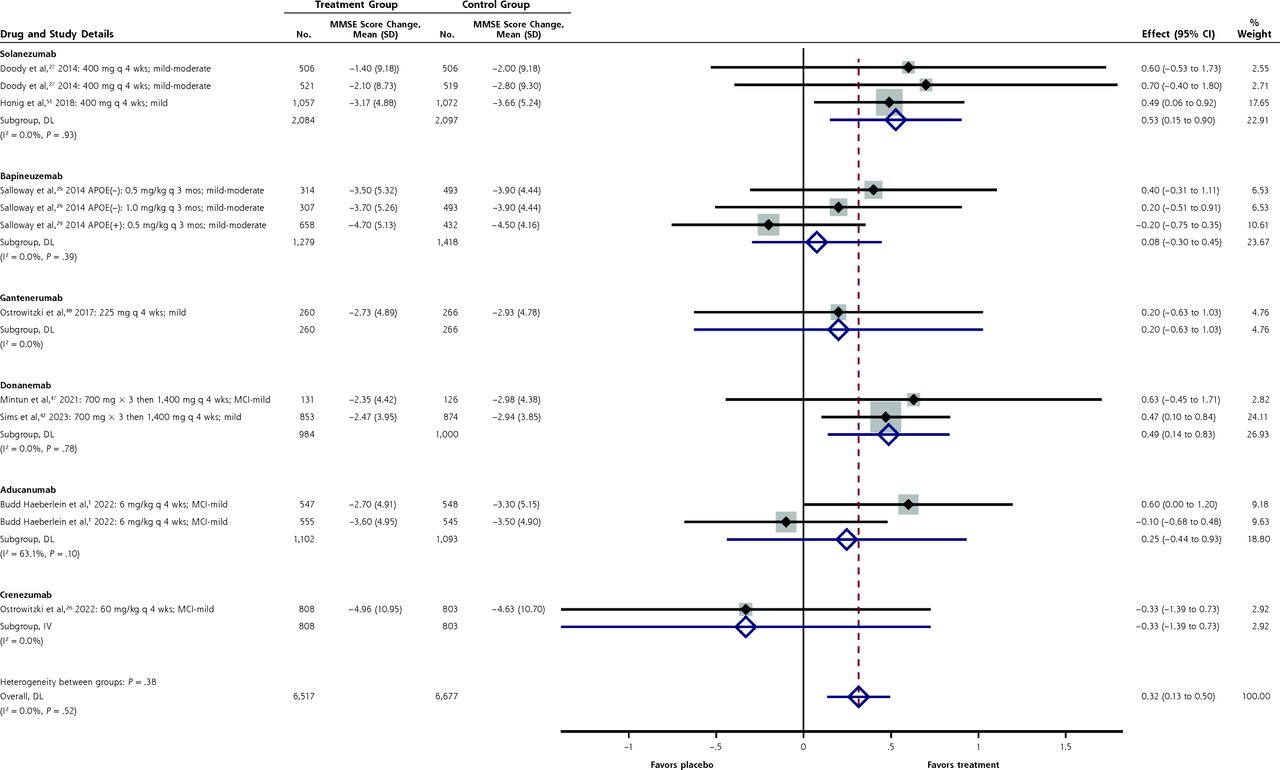
- Figure 2.
Forest plot for the mean differences in Mini Mental State Examination scores.
APOE = apolipoprotein E; DL = DerSimonian-Laird; MCI = mild cognitive impairment; MMSE = Mini Mental State Examination.
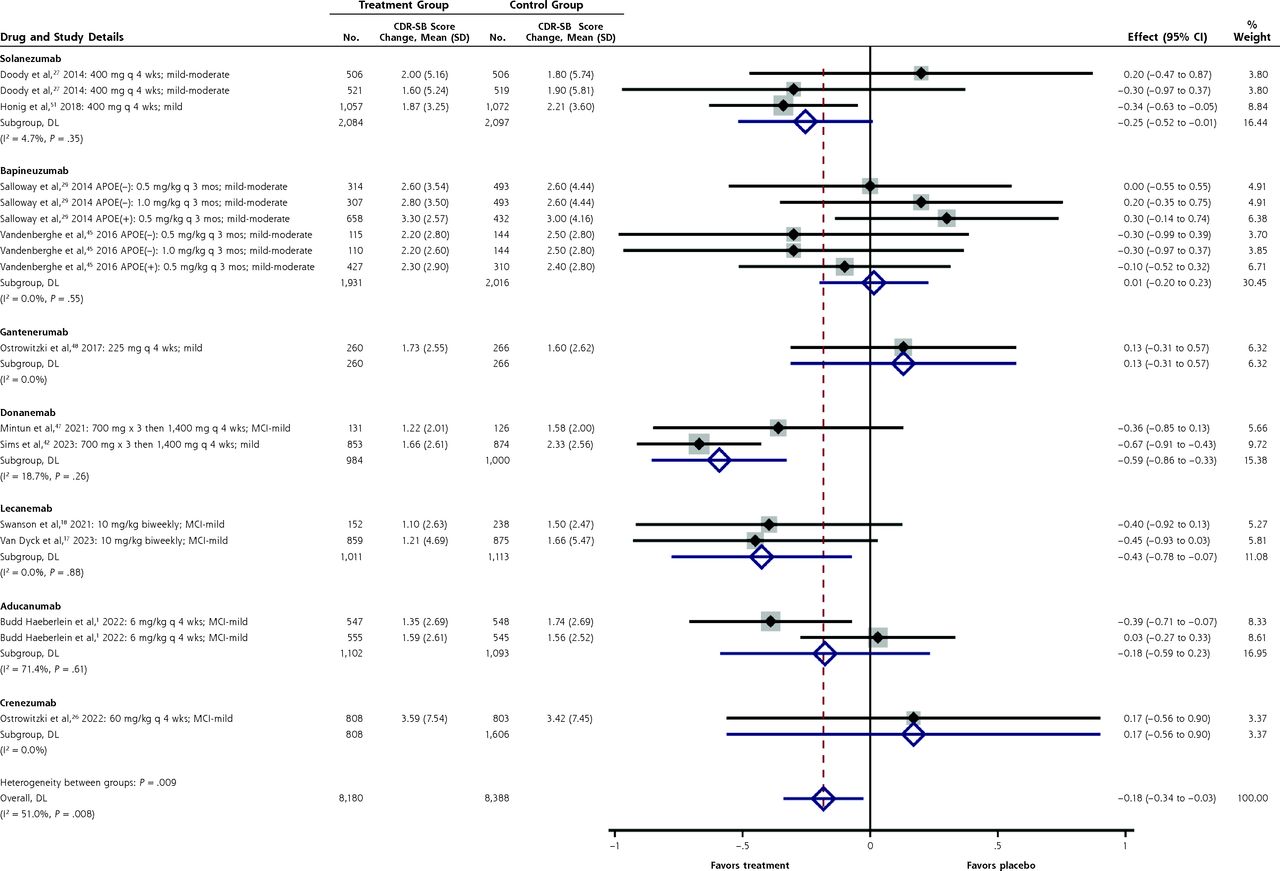
- Figure 3.
Forest plot for the mean differences in the Clinical Dementia Rating–Sum of Boxes scale.
APOE = apolipoprotein E; CDR-SB = Clinical Dementia Rating–Sum of Boxes scale; DL = DerSimonian-Laird; MCI = mild cognitive impairment.
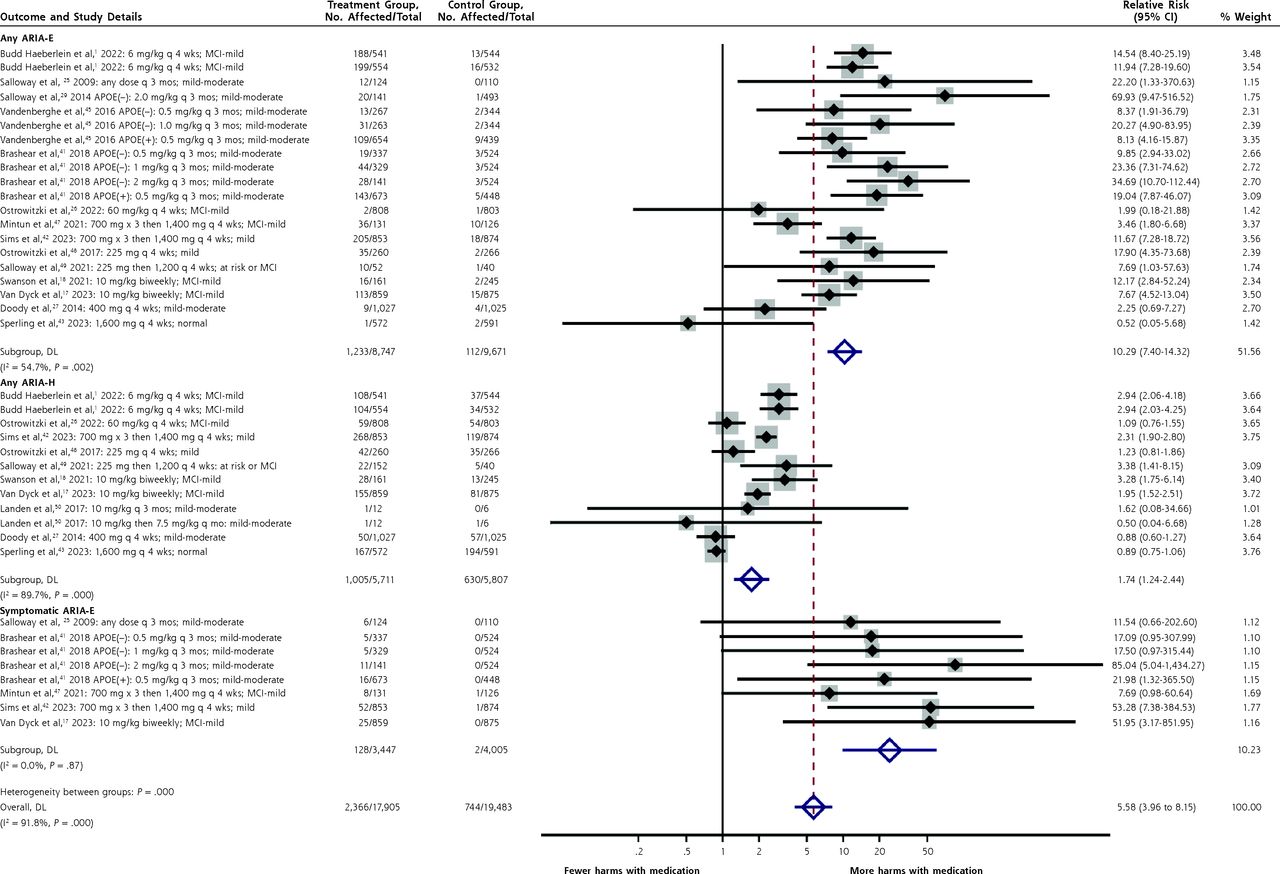
- Figure 4.
Forest plot for differences in any ARIA-E, any ARIA-H, and symptomatic ARIA-E.
APOE = apolipoprotein E; ARIA-E = amyloid-related imaging abnormalities of edema; ARIA-H = amyloid-related imaging abnormalities of hemorrhage; DL =DerSimonian-Laird; MCI = mild cognitive impairment. Note: Separate plots stratified by drug are given in Supplemental Figures 14-16.




Tables
Scoring Tool Range, Points MCID, Points Interpretation Cognitive assessments ADAS-Cog-11 0 to 7024 324 Lower is better ADAS-Cog-12 0 to 8025 3.5a Lower is better ADAS-Cog-13 0 to 8526 3.75a Lower is better ADAS-Cog-14 0 to 9027 4a Lower is better ADCOMS-overall 0 to 1.9728 0.14b Lower is better Neuropsychological test battery Z scale29 0.5 SD Higher is better MMSE 0 to 3030 1 to 330 Higher is better Functional assessments ADCS-ADL 0 to 78 5.5b Higher is better ADCS-ADL-MCI 0 to 5317 3.7b Higher is better DAD 0 to 100c31 7b,c Higher is better Behavioral disturbance NPI-Question 0 to 3632 832 Lower is better Combined or global assessments CDR-SB 0 to 1830 1 to 230 Lower is better iADRS 0 to 146 8.8b Higher is better Dependence scale 0 to 1533 1.5 to 233 Lower is better ADAS-Cog-11 = Alzheimer’s Disease Assessment Scale–Cognitive Subscale-11 items; ADAS-Cog-12 = Alzheimer’s Disease Assessment Scale–Cognitive Subscale-12 items; ADAS-Cog-13 = Alzheimer’s Disease Assessment Scale–Cognitive Subscale-13 items; ADAS-Cog-14 = Alzheimer’s Disease Assessment Scale–Cognitive Subscale-14 items; ADCOMS = Alzheimer’s Disease Composite Score; ADCS-ADL = Alzheimer’s Disease Cooperative Study–Activities of Daily Living; ADCS-ADL-MCI = ADCS-ADL for patients with Mild Cognitive Impairment; CDR-SB = Clinical Dementia Rating–Sum of Boxes scale; DAD = Disability Assessment for Dementia; iADRS = integrated Alzheimer’s Disease Rating Scale; MCID = minimal clinically important difference; MMSE = Mini Mental State Examination; NPI = neuropsychological inventory; SD = standardized difference.
↵a By extension from study of the ADAS-Cog-11.
↵b Estimated as 7% of the total range for the score.
↵c Percentages (not points).
Study and Year Substudya Drug and Dosing Duration, Mos Disease Severity Treatment Group, No. Placebo Group, No. Age, Mean, Y Budd Haeberlein et al,1 2022 ENGAGE and EMERGE Aducanumab 3 mg/kg q 4 wks 18 MCI or mild AD (MMSE score ≥24) 1,082 1,076 70.4 Aducanumab 6 mg/kg q 4 wks 1,096 1,076 Salloway et al,25 2009 Bapineuzumab 0.15 mg/kg q 3 mos 18 Mild to moderate AD (MMSE score 16-26) 31 26 69.1 Bapineuzumab 0.5 mg/kg q 3 mos 33 28 Bapineuzumab 1.0 mg/kg q 3 mos 29 26 Bapineuzumab 2.0 mg/kg q 3 mos 29 27 Salloway et al,29 2014 Study 301 APOE(−) Bapineuzumab 0.5 mg/kg q 3 mos 18 Mild to moderate AD (MMSE score 16-26) 314 493 72.5 Bapineuzumab 1.0 mg/kg q 3 mos 307 493 Bapineuzumab 2.0 mg/kg q 3 mos 141 493 Study 302 APOE(+) Bapineuzumab 0.5 mg/kg q 3 mos 658 432 Lacey et al,44 2015 Study 301 APOE(−) Bapineuzumab 0.5 or 1.0 mg/kg q 3 mos 18 Mild to moderate AD (MMSE score 16-26) 621 493 72.5 Study 302 APOE(+) Bapineuzumab 0.5 mg/kg q 3 mos 658 432 72.2 Vandenberghe et al,45 2016 APOE(−) Bapineuzumab 0.5 mg/kg q 3 mos 18 Mild to moderate AD (MMSE score 16-26) 267 344 70.5 Bapineuzumab 1.0 mg/kg q 3 mos 263 344 APOE(+) Bapineuzumab 0.5 mg/kg q 3 mos 18 Mild to moderate AD (MMSE score 16-26) 654 439 Brashear et al,41 2018 Study 301 APOE(−) Bapineuzumab, 0.5 mg/kg q 3 mos 19 Mild to moderate AD (MMSE score 16-26) 337 524 72-74 Bapineuzumab, 1 mg/kg q 3 mos 329 524 Bapineuzumab, 2 mg/kg q 3 mos 141 524 Study 302 APOE(+) Bapineuzumab, 0.5 mg/kg q 3 mos 673 448 Cummings et al,46 2018 Crenezumab 15 mg/kg q 4 wks 17 Mild to moderate AD (MMSE score 18-26) 165 82 70.6 Crenezumab 300 mg q 2 wks 122 62 Ostrowitzki et al,26 2022 CREAD and CREAD2 Crenezumab 60 mg/kg q 4 wks 24 Prodromal or mild AD (MMSE score ≥22) 808 803 70.7 Mintun et al,47 2021 TRAILBLAZER-ALZ Donanemab 700 mg × 3 then 1,400 mg q 4 wks 19 Early or mild AD 131 126 75.2 Sims et al,42 2023 TRAILBLAZER-ALZ 2 Donanemab 700 mg × 3 then 1,400 mg q 4 wks 18 MCI or mild AD 860 876 74 Ostrowitzki et al,48 2017 Gantenerumab 105 mg q 4 wks 24 Mild AD (MMSE score ≥24) 271 266 70.4 Gantenerumab 225 mg q 4 wks 260 266 Salloway et al,49 2021 Gantenerumab 225 mg then 1,200 mg q 4 wks 24 Normal but at elevated risk or early AD 52 40 43.8 Swanson et al,18 2021 Lecanemab 10 mg/kg biweekly 18 MCI or mild AD 152 237 72b Lecanemab 10 mg/kg monthly 253 245 Van Dyck et al,17 2023 Lecanemab 10 mg/kg biweekly 18 MCI or mild AD 859 875 71.2 Landen et al, 50 2017 Cohort M Ponezumab 10 mg/kg then 7.5 mg/kg q month 18 Probable AD 12 6 67.8 Cohort Q Ponezumab 10 mg/kg q 3 mos 12 6 Doody et al,27 2014 EXPEDITION 1 Solanezumab 400 mg q 4 wks 18 Mild to moderate AD (MMSE score 16-26) 506 506 74.7 EXPEDITION 2 Solanezumab 400 mg q 4 wks 521 519 72.5 Farlow et al,36 2012 Solanezumab 100 mg q 4 wks 12 Mild to moderate AD (MMSE score 15-26) 10 10 NR Solanezumab 100 mg weekly 11 10 Solanezumab 400 mg q 4 wks 10 10 Solanezumab 400 mg weekly 11 10 Honig et al,51 2018 Solanezumab 400 mg q 4 wks 18 Mild AD (MMSE score 20-26) 1,057 1,072 73.0 Sperling et al,43 2023 Solanezumab 1,600 mg q 4 wks 54 Normal cognition with amyloid deposition 564 583 72 AD = Alzheimer disease; APOE = apolipoprotein E; APOE(+) = carriers of the ApoE mutation; APOE(−) = noncarriers of the ApoE mutation; MCI = mild cognitive impairment; MMSE = Mini Mental State Examination (score range is 0-30); NR = not reported.
↵a Shown where a study had an identifiable name or subgroup other than by dose.
↵b Median.
Study and Year Sequence Generation Allocation Concealment Blinding of Personnel and Patients Blinding of Outcome Assessors Incomplete Outcome Data (% Missing) Selective Outcome Reporting Other Sources of Bias Overall Risk of Bias Brashear et al,41 2018 Low Low Low Low Low (0.4) Low Low Low Budd Haeberlein et al,1 2022 Low Low Low Low Low (0.6) Low Low Low Cummings et al,46 2018 Low Low Low Low High (26) Low Low High Doody et al,27 2014 Low Low Low Low High (24.7) Low Low High Farlow et al,36 2012 Low Unclear Low Low Low (4) Low Low Unclear Honig et al,51 2018 Low Unclear Low Low High (14) Low Low High Lacey et al,44 2015 Low Low Low Low High (29) Low Low High Landen et al,50 2017 Low Unclear Low Low Low (5.5) Low Low Unclear Mintun et al,47 2021 Low Low Low Low High (32) Low Low High Ostrowitzki et al,48 2017 Low Low Low Low High (53.8) Low Low High Ostrowitzki et al,26 2022 Low Low Low Low Low (7) Low Low Low Salloway et al,25 2009 Low Low Low Low High (23.5) Low Low High Salloway et al,29 2014 Low Low Low Low High (29) Low Low High Salloway et al,49 2021 Low Unclear Low Low Low (6) Low Low Unclear Sims et al,42 2023 Low Low Low Low High (24) Low Low High Sperling et al,43 2023 Low Low Low Low High (28) Low Low High Swanson et al,18 2021 Low Unclear Low Low Low (6.5) Low Low Unclear Van Dyck et al,17 2023 Low Low Low Low High (17) Low Low High Vandenberghe et al,45 2016 Low Low Low Low High (49) Low Low High
SUPPLEMENTAL MATERIALS IN PDF FILE BELOW
- Ebell-Supp.pdf -
PDF file
- Ebell-Supp.pdf -
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Co-activation of selective nicotinic acetylcholine receptor subtypes is required to reverse hippocampal network dysfunction, fear memory loss, and amyloid pathology in Alzheimers disease
- Assessing the clinical meaningfulness of slowing CDR-SB progression with disease-modifying therapies for Alzheimer disease