
Article Figures & Data
Figures
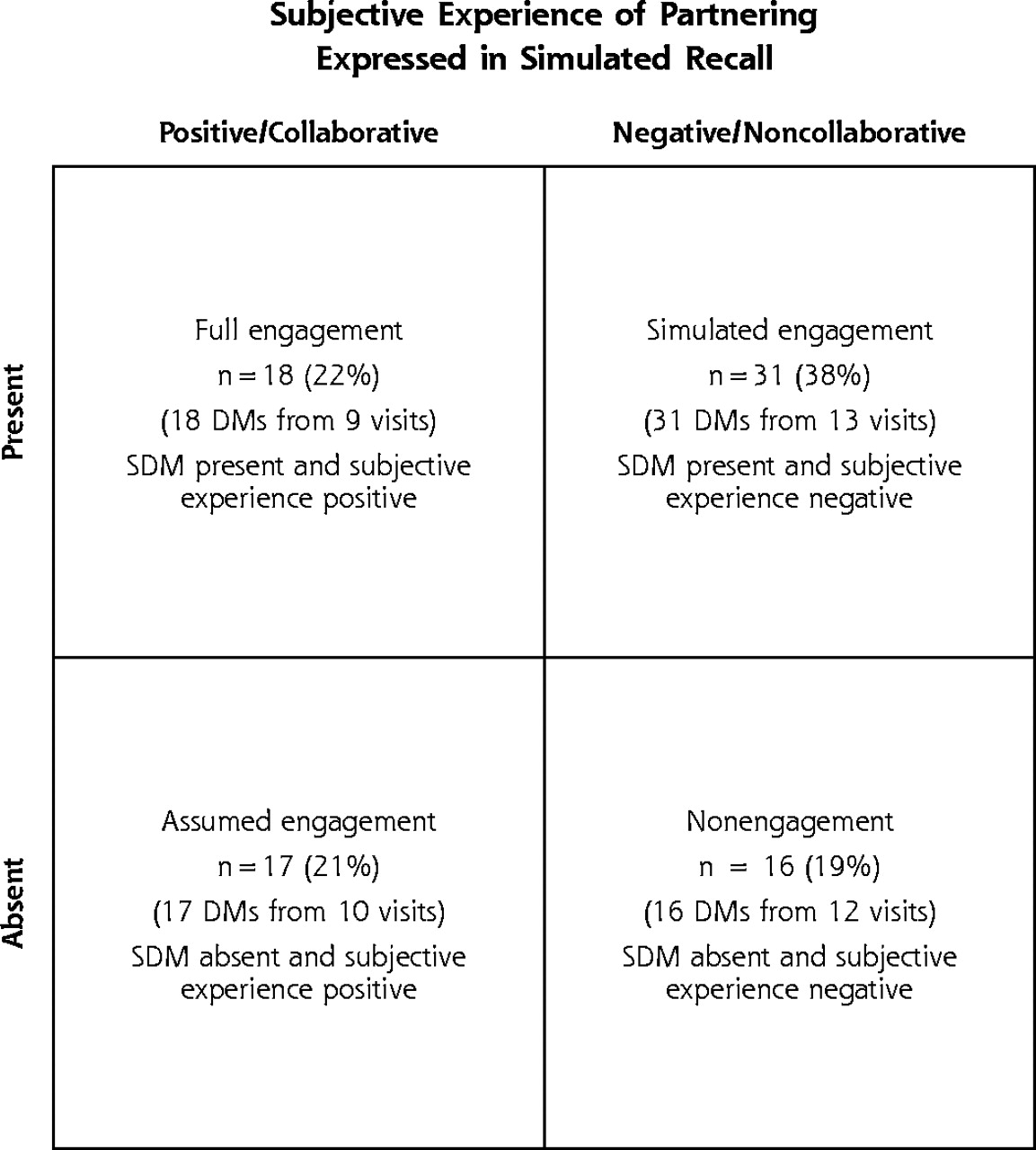
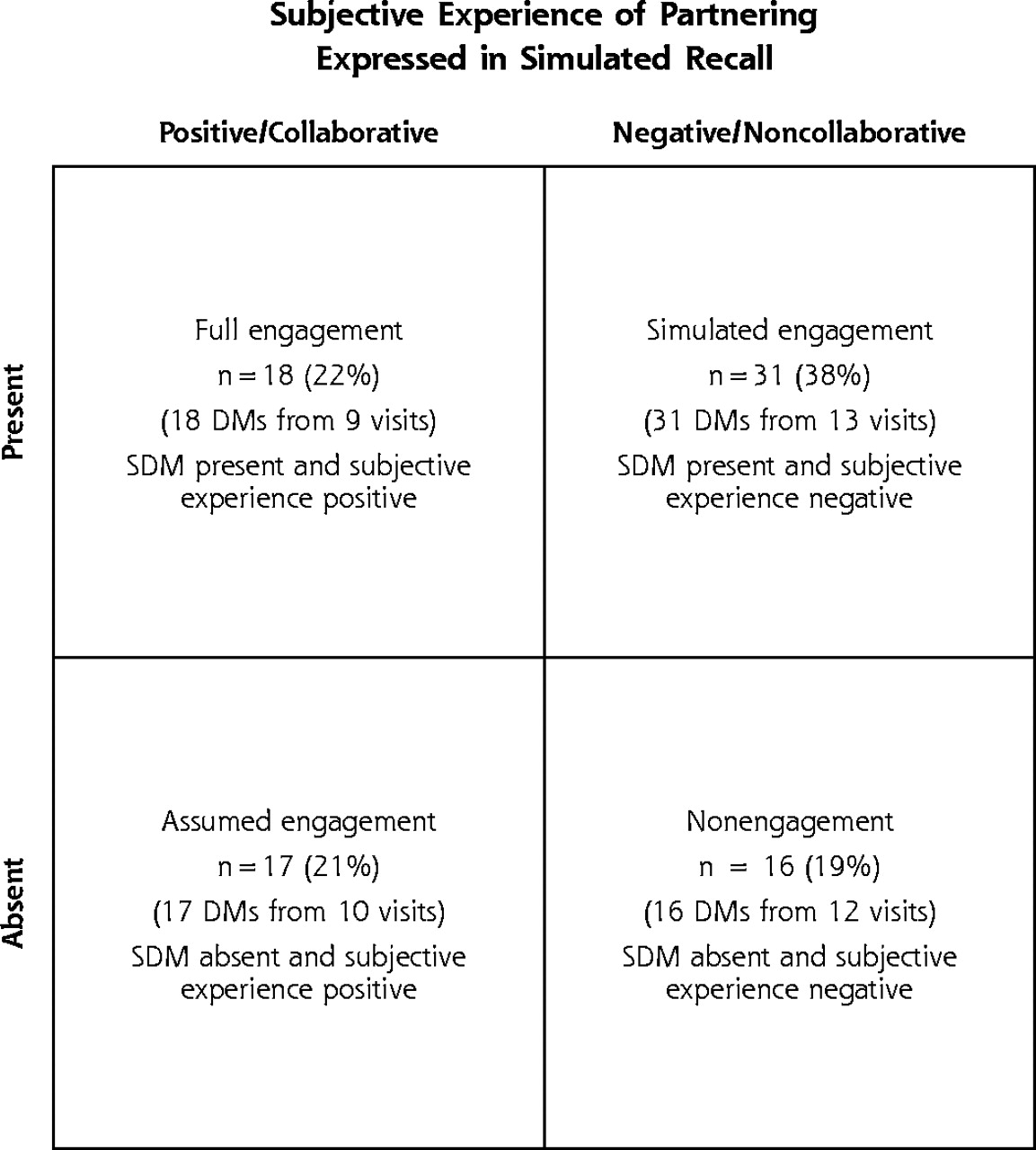
- Figure 1.
The 4 archetypes of engagement in decision making.
DM = decision moment
Tables
Characteristics Patient characteristics (n = 18) No. (Range) Physician characteristics (n = 18) Age, years, mean 62 (42–78) Sex Female 7 Male 11 Race/ethnicity, self-reported African American 7 Asian 3 Latino 5 White 3 Education, years, mean 10 (0–18) Language spoken English 15 Spanish 3 Physician characteristics (n = 10) Age, years, mean 44.6 (37–60) Sex Female 6 Male 4 Race/ethnicity, self-reported African American 1 Asian 1 Latino 1 White 7 Time in practice, years, mean 14 (8–40) Patient-physician relationship (n = 18) Continuity, years, mean 6 (0.5–15) Characteristic Decision Moments No. (%) SDM = shared decision making. *Among the subset of decision moments available for combined analysis. Topic Medication 41 (33) Self-management and lifestyle 28 (22) Referrals 24 (19) Tests 20 (16) Other treatments 12 (10) Total 125 (100) Distribution of SDM scores 0–2 25 (20) 3–5 38 (30) 6–8 43 (35) 9–10 19 (15) Total 125 (100) Distribution of subjective experiences* Positive 35 (43) Negative 47 (57) Total 82 (100) Nature of the negative subjective experiences Both physician and patient negative 8 (17) Only physician negative 25 (53) Only patient negative 14 (30) Total 47 (100) Variation of Archetypes Within a Visit No. of Visits (n = 18) All decision moments in visit coded as the same archetype (eg, all decision moments in Visit 23 were coded as simulated engagement) 2 Majority (60%–90%) of the decision moments in visit coded as the same archetype 8 No majority of decision moments in visit coded as the same archetype 8 - Table 4.
Communication Behaviors and Relationship Themes Characteristic of Archetypes of Engagement in Decision Making
Archetype Communication Behaviors Relationship Themes Clinical Example SDM = shared decision making. Full engagement: SDM present and both participants found experience positive Physicians and patients: Negotiated decisions Used flexible decision-making style Physicians and patients: Felt listened to and understood Trusted each other Expressed differences of opinion Agreed to disagree about some decisions Patient requested an anxiolytic medication to cope with a divorce. Ensuing conversation included all 10 of the elements of SDM, and stimulated recall revealed a mutually positive experience. [Visit 23] Patient: “She trusts me. She believes I wouldn’t abuse it. She believes in me, and that’s a big thing. I would never do that to her anyway. Some addicts would play their doctors; I’ve never played her like that. She really cares for me. We are pretty straightforward with each other; I always tell her the truth. She’s never given up on me.” Physician: “She’s going through a big thing [leaving her husband]. She’s more paranoid about getting addicted again than I am; so I decided to give it [the Valium]. I didn’t want her to think I don’t trust her. Thirty Valium is not that big of a deal to me in our relationship or in her care.” Simulated engagement: SDM present and 1 or both of the participants found experience negative Physicians and patients: Did not disclose relevant clinical information Did not disclose emotional reactions Did not check assumptions Assumed what other person was thinking Physicians and patients: Mistrusted that clear communication would be useful Experienced sense of hopelessness Patients: Feared negative judgment Felt disrespected Physician and patient considered how weight loss might improve the patient’s diabetes. The SDM score was relatively high (6/10), yet both the patient and the physician found the experience negative. Here, the patient did not disclose relevant clinical information, assuming that the physician would be angry at her if she revealed this information. [Visit 37] Patient: “I haven’t told him [the physician] I am eating pastries.… I don’t want to disappoint him and run the risk that he says I’ve done a lot for you and you are not doing your part.… I can’t afford to lose him. I’m not being honest.” Physician: who chose to not display his emotions about a challenging situation, saying, “Talking about weight reduction is another big topic, and although important, it’s not a priority issue here. I had other important issues to talk about, so to talk about another nonpressing matter without a satisfactory conclusion is frustrating. My vision of her is a lot of loose ends that are just kept loose.” Assumed engagement: SDM absent and both participants found experience positive Physicians and patients: Assumed understanding each other and why other person acted the way he/she did Did not check out assumptions Physicians and patients: Trusted each other Felt listened to and understood Were confident they were on the same wavelength Patient requested medication to help her sleep. SDM did not occur (score = 1/10), but both the physician and patient found the experience positive. In this situation, the patient had an inaccurate assumption about why her physician acted a certain way. [Visit 12] Patient: “He didn’t just give me stronger medicine or say, ‘Well, I think we should increase your dose, or we should do this.’ He didn’t go there. That makes me feel like he’s concerned about me medical-wise and pain-wise, because he’s not going just take my say-so and give me something.” Physician: “There wasn’t time at the end, so I wasn’t going to get into the sleep issue with her.” The physician expresses satisfaction in being able to keep the discussion during the visit focused on what he considered more pressing issues. Nonengagement: SDM absent and 1 or both participants found experience negative Physicians and patients: Did not disclose relevant clinical information Did not disclose emotional reactions Did not check assumptions Assumed what other person was thinking Assumed how other person would respond if told the truth Physicians and patients: Mistrusted that clear communication would be useful Experienced sense of hopelessness Patients: Feared negative judgment Felt disrespected A decision moment that focused on adherence to dietary restrictions for a diabetic patient had low SDM (score = 4/10), and both partners had a negative experience. The patient’s stimulated recall revealed that he did not disclose relevant clinical information and believed his views would be discounted by his physician. The physician’s stimulated recall revealed his feeling of hopelessness in providing care [Visit 8]. Patient: (commenting on the physician’s instruction not to eat flan and to throw out unwanted desserts) “Back in the Philippines, my parents said not to waste food and throw it away. I have relatives who are physicians who tell me not to worry too much about my diet. They know it’s hard to have diabetes and say it’s okay to have a beer, a light beer, and relax. I know my doctor is concerned about my health, so I don’t tell him. You want to enjoy your life. If I tell him, he will just tell me what will happen to my body.” Physician: “He’s never been adherent to a diabetic diet, and here he is obviously blatant about not being adherent. I was trying to plant a seed, but I have some frustration and a sense of almost futility with this patient.”
Supplemental Appendixes
Supplemental Appendix 1. Coding Instrument for Do of Visits. Supplemental Appendix 2. Illustrative Quotes for the Archetypes of Engagement in Decision Making.
Files in this Data Supplement:
- Supplemental Appendixes - PDF file, 3 pages, 91 KB
The Article in Brief
Shared Decision Making and the Experience of Partnership in Primary Care
George W. Saba, PhD , and colleagues
Background The goal of this study is to learn more about shared decision making, in which patients and physicians make decisions after openly exchanging information and exploring beliefs. The study looks at how the communication behavior of shared decision making is related to patients� and physicians� experience of partnership. The study also tests new research strategies for understanding the relationship between communication skills and personal experience.
What This Study Found Communication behavior and relationship factors influence personal experiences of partnership between patients and doctors. In many (41%) of the decision moments, there was agreement between participants� perception and the study�s ratings of shared decision making. But for most (59%) decision moments, communication behaviors and personal experience were not aligned. In 38% of decision moments, patients and physicians exchanged information and beliefs and appeared to make joint decisions; however, their relationship was characterized by mistrust, withholding of crucial information, or mutual frustration. In 21% of decision moments, patients and physicians collaborated in decision making despite a limited amount of clear communication.
Implications
- Communication is more complex than a set of communication behaviors.
- Shared decision making can appear successful, but when the process is not truly collaborative, important information can be withheld, and participants may have different intentions about a care plan.
- Efforts to strengthen patient-physician communication, especially among disadvantaged populations, must focus on both communication behavior and personal interactions.




{kind=link}
Jump to section
Related Articles
Cited By...
- Primary Care Practices' Implementation of Patient-Team Partnership: Findings from EvidenceNOW Southwest
- How often do both core competencies of shared decision making occur in family medicine teaching clinics?
- Clinical decisions presented to patients in hospital encounters: a cross-sectional study using a novel taxonomy
- What is a medical decision? A taxonomy based on physician statements in hospital encounters: a qualitative study
- Older patients and their GPs: shared decision making in enhancing trust
- Evidence-based patient information programme in early multiple sclerosis: a randomised controlled trial
- How Much Shared Decision Making Occurs in Usual Primary Care of Depression?
- Video Elicitation Interviews: A Qualitative Research Method for Investigating Physician-Patient Interactions
- Shared Mind: Communication, Decision Making, and Autonomy in Serious Illness
- The Values and Value of Patient-Centered Care
- Why The Nation Needs A Policy Push On Patient-Centered Health Care
- 'Another Compelling Idealized Model That Is Drastically Altered by the Ugly Facts on the Ground'
- In This Issue: Diabetes Quality of Care