
Abstract
PURPOSE We assessed the impact of the severe influenza vaccine shortage of 2004 on individual physicians’ immunization performance.
METHODS Using 1998–2004 Medicare claims data, we monitored the physician continuity rate (proportion of patients receiving influenza immunization from a physician in 1 year who received a subsequent immunization from the same physician the subsequent year) and other clinician rate (proportion of patients with claims from 1 physician in 1 year with a claim from another clinician the subsequent year) in West Virginia Medicare beneficiaries from 2000–2004. We examined vaccine claim trends by clinician and surveys of self-reported immunization to determine whether patients received vaccine from nonphysician clinicians or went without immunization each year.
RESULTS Claims-based influenza vaccination rates increased from 35.5% to 41.3% from 2000–2003, reflecting historical trends, before declining 14.1% in 2004. Median continuity rates among the 723 to 849 physicians claiming 25 or more influenza immunizations from 2000–2003 increased from 47% in 2000–2001 to 54% in 2002–2003; then fell to 3% in 2003–2004. The number of physicians filing 100 or more claims declined from 337 in 2003 to 130 in 2004. More than 25% of physicians had no repeat vaccinations of the same beneficiaries in 2004. Trends in clinician type and survey data indicated a shift of many beneficiaries to mass vaccinators and institutional providers; however, compared with previous years, there was an estimated 8% increase in 2004 in the number of West Virginia beneficiaries who did not receive vaccine.
CONCLUSIONS The 2004 vaccine shortage had a severe impact on influenza immunization rates in private physician’s offices, disrupting continuity of care.
INTRODUCTION
Annual influenza vaccination has been recommended for preventing influenza and its complications in older Americans for years. Medicare covers this preventive service without a deductible or copayment. The Centers for Medicare & Medicaid Services (CMS) considers influenza immunization rates a measure of quality of care in various settings, and it has charged its quality improvement organization contractors with promoting vaccination.
West Virginia has historically lagged behind in the United States in indicators of influenza vaccine use in older residents.1–3 Individual practitioners in West Virginia are believed to provide the bulk of influenza immunizations to Medicare beneficiaries. The West Virginia Medical Institute (WVMI, a Medicare quality improvement organization) has conducted projects aimed at improving rates of influenza immunization in West Virginia since the mid-1990s. Recognizing the importance of individual physicians in influencing patient behavior, WVMI has targeted increasing the vaccination rates of these physicians, both directly through audit and feedback and professional education, and indirectly through media and individualized communications with beneficiaries.
There have been several disruptions of influenza vaccine supplies affecting West Virginia physicians in recent years. In 2000, vaccine supplies were delayed.4 In 2004, there was a severe shortage of influenza vaccine in the United States, resulting in a recommendation to limit vaccination to persons in high-risk groups, including those older than age 65 years who make up the bulk of Medicare beneficiaries.5 Although subsequent self-reports suggest patients and physicians may have responded appropriately to this recommendation when vaccine was available at all,6 it is not clear how widespread shortages affected individual physician practices or the patients they serve.
There have been a few studies of patient behavior when confronted with vaccine shortages. The Medicare Current Beneficiary Survey recorded vaccine unavailability as a reason for nonreceipt of influenza vaccine for the first time in the 2000 season, when an estimated 4.3% of the population aged 65 years and older did not get vaccine for this reason.7 Zimmerman and colleagues8 observed no reduction in self-reported influenza immunization rates in an inner-city population with good access to vaccine in 2000, but respondents’ attitudes about influenza vaccine changed for the worse. The Harvard School of Public Health conducted a national survey of patients’ experience trying to get influenza vaccine during the 2004 shortage, finding that 37% of adults aged 65 years and older and 54% of adults younger than 65 years with chronic disease had been unable to get the vaccine.9 The investigators neither reported whether physicians had advised low-risk individuals to defer vaccination nor described other physician responses to shortage.
There is less information available about physician responses to vaccine shortages. In 2002, Davis and colleagues reported on physicians’ self-reported influenza immunization behavior and practice capacity to support immunization.10 These researchers predicted problems in the event of an influenza vaccine shortage because of an inability to identify patients most needing immunization. Zimmerman’s group identified vaccine shortage as a likely reason for decline in influenza immunization rates in 2000 and 2001, but their work focused mainly on how traditional physician office operational and attitudinal factors influenced immunization rates.11 The Centers for Disease Control and Prevention reported the apparent redirection of much of the 2004 influenza vaccine supply to persons in high-priority groups but did not collect or report information on physician response to vaccine shortages.12
We describe changes in immunization quality measures in West Virginia physicians who bill Medicare individually. We assessed the likely impact of influenza vaccine shortages on physician performance as measured by repeat immunization rates in West Virginia Medicare beneficiaries and explored simultaneous changes in mix of clinicians providing immunizations that may be a consequence of the shortage.
METHODS
We hypothesized that periods of vaccine shortage would have disrupted continuity of care, as patients who were unable to get vaccine from their personal physicians either sought and received vaccine elsewhere or did not get immunized at all. We focused on continuity of care measured by repeat vaccination rates, because it would not have been feasible to enumerate physician pratice populations to calculate practice-specific absolute immunization rates in a fee-for-service environment, and because we believed a measure of continuity of care would be relevant to primary care physicians. We examined trends in proportions of vaccine claims by clinician type to see whether some beneficiaries might be shifting to sources of influenza vaccine other than physicians, and we compared survey results with claims to assess changes in proportions of beneficiaries receiving vaccine from nonbilling clinicians.
We used files of influenza claims that the CMS provides their quality improvement organizations annually to compute physician-level rates of reimmunization of individual beneficiaries by the same physician in consecutive years. This physician continuity rate is a quality of care measure that encompasses both a vaccination rate in a group of patients with demonstrated willingness to undergo vaccination as well as a practice’s success in retaining patients in a preventive regimen for the long term.
CMS influenza claims files contain one record for each Medicare beneficiary in the state during the vaccination year, as well as information on the clinician and claim particulars for an influenza vaccination given between September 1 and December 31 if a claim was submitted before March 1 of the following year. We examined influenza claims for missing unique physician identifier numbers for each year; missing physician identifier numbers were imputed based on associations with physician profiling numbers in the data. We cross-referenced beneficiary claim numbers against the CMS national enrollment database to account for changes in numbers across years, and cross-referenced claims with physician identifiers on the beneficiary number for 2 consecutive years. Before 2000, CMS supplied influenza claims in a different format, and we derived the West Virginia denominator from the enrollment database, identifying beneficiaries who had died, left the state, or joined a managed care program between the initial and final year of the period.
We included only physician identifier numbers for individual physicians (A00000 through H99999). Group physician identifier numbers are infrequently coded in West Virginia, and nonphysician clinicians account for a very small proportion of billed immunizations. Only a minority of West Virginia beneficiaries are enrolled in managed care programs (eg, there were 20,185 beneficiaries in 2004, or 7.6% of 263,730 beneficiaries older than 65 years with Part B coverage in October); they are not included in this analysis because managed care programs do not submit claims to CMS. Patients of rural health centers and federally qualified health centers are also not included for the same reason. We estimated that 10.2% of West Virginia Medicare beneficiaries used federally qualified health centers in 2001.13
For all beneficiaries with claims submitted under an individual physician identifier number in the first year, we determined whether the beneficiary was still in the denominator the second year. We calculated rates based on the number of beneficiaries who received immunizations from a single physician who were still living within West Virginia and in the fee-for-service program the subsequent year. We calculated the physician continuity rate as the number of beneficiaries with an immunization claim from the same physician identifier number the second year as in the first, divided by the number of beneficiaries with claims from that physician identifier number in the first year. The other clinician rate was calculated similarly from beneficiaries with claims from physician identifier numbers other than the first-year identifier number, and the no-claim rate was the remainder of beneficiaries with claims from the physician the first year but no claim from any clinician in the second. Beneficiaries without claims could have received a vaccination from nonbilling clinicians.
In the main analysis, we included only physicians with 25 or more influenza vaccination claims in the initial year of each pair to assure reasonably stable quality indicator rates; consequently, the population of physicians included in the analysis may vary from year to year and does not include all physicians who filed claims. We tabulated trends of numbers of physicians with 25 or more influenza vaccine claims; physician continuity, other clinician, and loss rates; and average claims per physician between 1997 and 2004.
We compared trends in these quality indicators in individual physician offices with other sources of information about influenza immunization in the West Virginia fee-for-service Medicare population during the same time. We used the Behavioral Risk Factor Surveillance System trends in self-reported influenza immunization rates in persons 65 years old and older to gauge the proportion of persons immunized in the entire population. We assumed that the immunization rate of beneficiaries receiving managed care or federally qualified health center services was the same as in the fee-for-service population, based on the results of the 2001 analysis showing that they were statistically indistinguishable that year.13 Using estimates of sensitivity and specificity of a telephone survey of managed care patients compared with medical record documentation of influenza vaccination reported by Mac-Donald et al,14 we estimated the proportion of West Virginia Medicare beneficiaries actually immunized in the previous year from Behavioral Risk Factor Surveillance System results, when available. We compared this estimate with Medicare claims. We reasoned that the claims rate of influenza immunization would be equal to the estimated rate from the survey data in the absence of nonbilling clinicians, assuming that West Virginia beneficiaries’ responses to the Behavioral Risk Factor Surveillance System questions were comparable to Minnesotans’ answers to a similar survey item. The difference would represent the proportion of beneficiaries using nonbilling clinicians.
We analyzed time trends in the proportion of Medicare beneficiaries who received influenza shots from different types of clinicians. We classified each paid influenza claim as institutional (Part A) or out-patient (Part B). Institutional claims were divided into hospital, nursing home, home health, and other Part A according to the value of the facility type code on the claim. Outpatient claims were considered to be from physicians if their identification number fields were between A00000 and H99999, or if their fields were blank with a place of service code of 11, or with an identifier number between W00000 and Y99999 with a place of service code other than 01, 60, or 71. The outpatient claims were considered to be from mass vaccinators if their identifier number fields were blank or between W00000 and Y99999 with a place of service code of 01, 60, or 71. Otherwise, we considered the claims to be submitted by other Part B clinicians, eg, individually billing nurse-practitioners.
RESULTS
Table 1⇓ shows the specialty distribution of the 799 physicians with 25 or more claims in 2003. Almost 80% were in primary care specialties (general practice, family practice, or internal medicine). More than 70% (573) of the physicians had 25 or more claims in each of the 3 previous years.
Specialty Distribution of West Virginia Physicians Providing Influenza Immunization, 2004
Table 2⇓ shows the number of influenza vaccine claims for individual physicians from 1999 through 2004. Total claims, number of physicians, and claims per physician were relatively stable through 2003. In 2004 total claims and number of physicians with 25 or more claims declined by more than 50% from the previous year, and average claims per physician declined by almost one third.
West Virginia Physicians with Medicare Claims for Influenza Immunization, 1999–2004
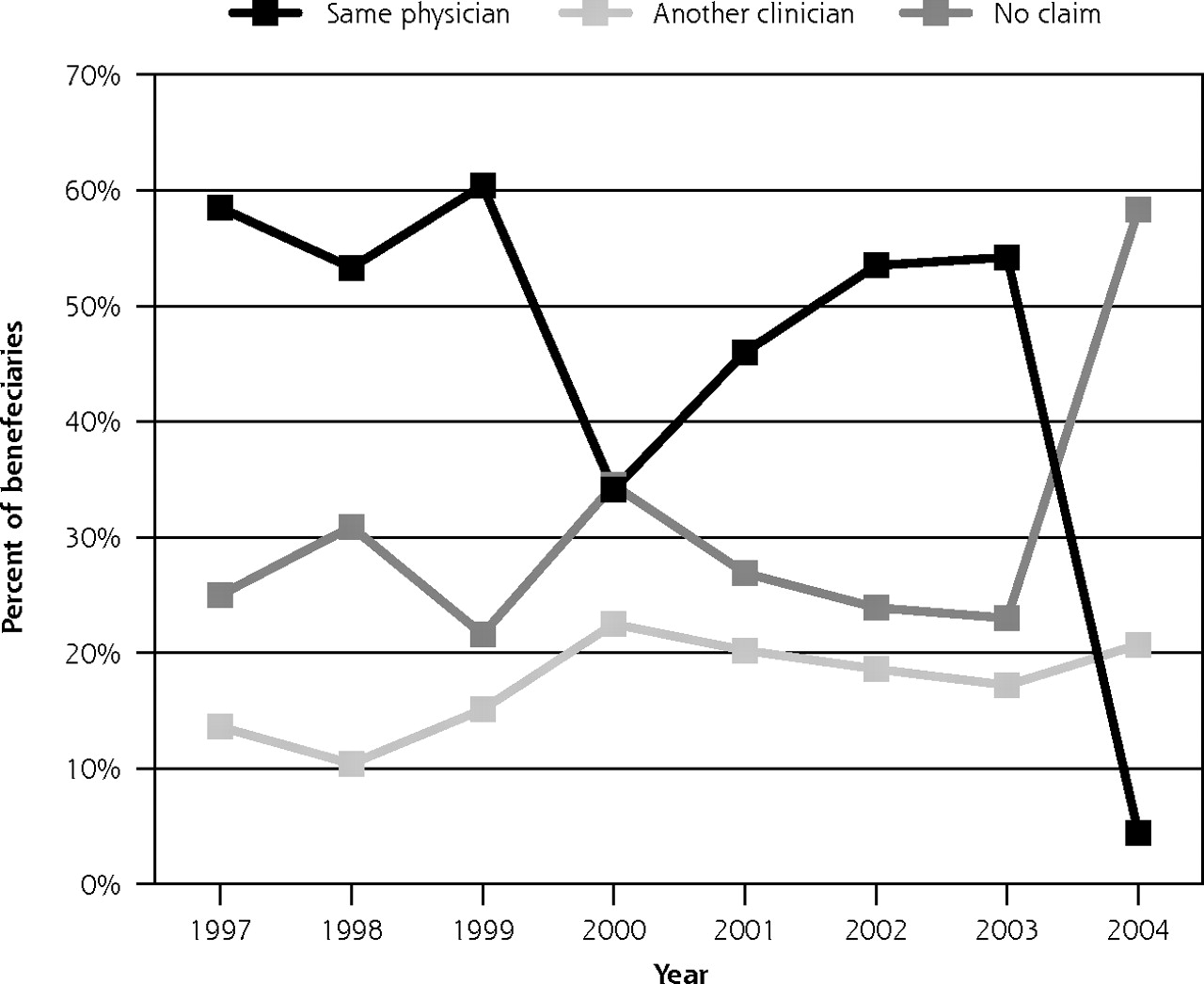
Figure 1⇓ shows the time trends of the practice-level indicators. In 2000, the physician continuity rate, which had been slowly increasing, fell by an absolute 25%. During the next 3 years it recovered before a decline from more than 50% in 2003 to 4.4% in 2004. Between 2003 and 2004 the other clinician rate increased by 3%; most vaccinees in 2003 had no claims for influenza vaccine in 2004.
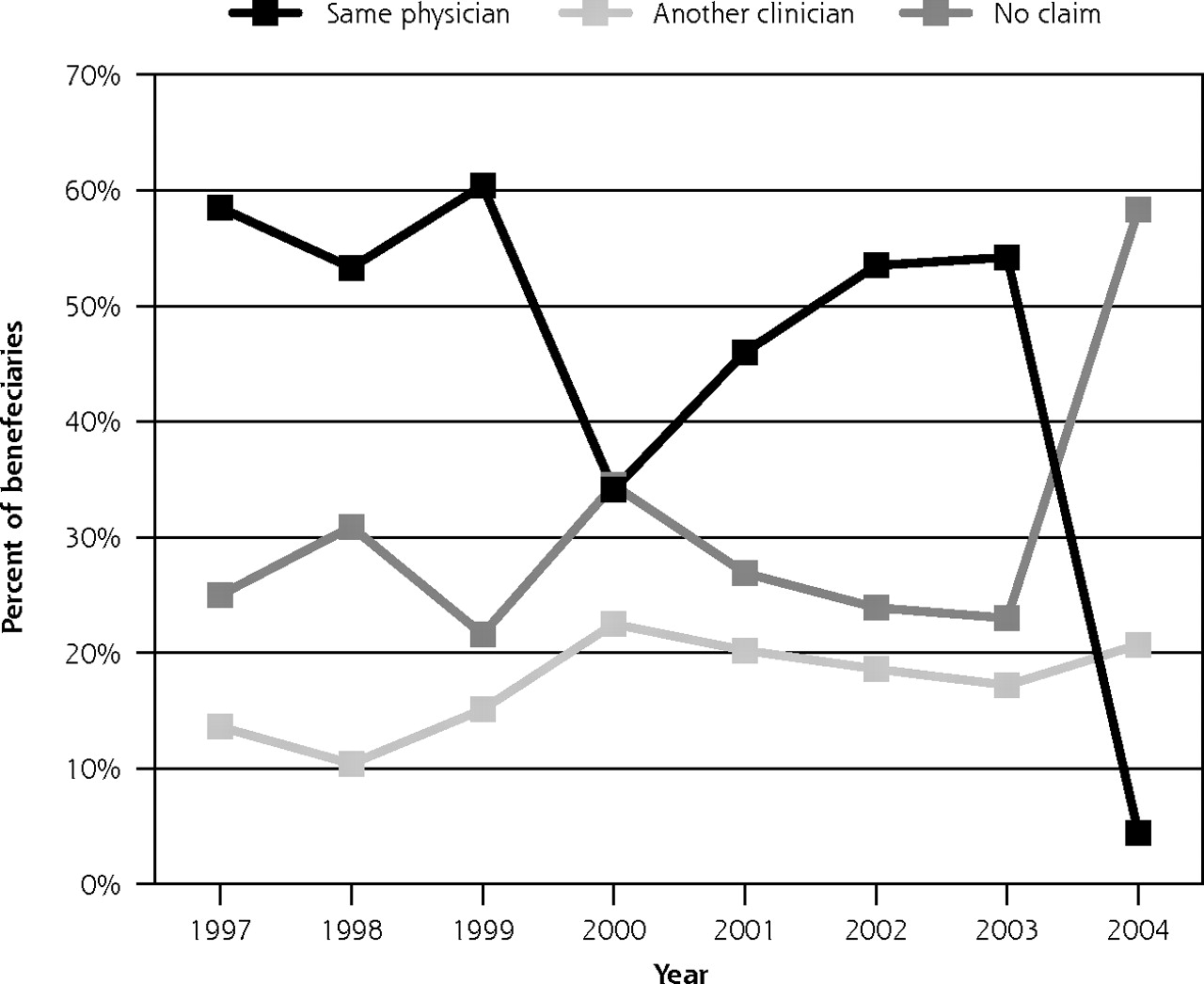
Claims rates for influenza immunization from the same physician, another clinician, or no clinician, by year.
Annual median percentages of fee-for-service Medicare beneficiaries =65 years with claims for influenza immunization the previous year having current year claims from the same physician, another clinician, or no claim. Figure is based on claims reported to the Centers for Medicare & Medicaid Services by unique physician identifying numbers for West Virginia and includes physicians claiming at least 25 immunizations between September 1 and December 31 of each year. The percentages represent the median for each indicator across all such physicians in a given year.
The numbers and proportions of vaccine claims by source from 1999 through 2004 appear in Table 3⇓. The number of physicians differs from that in Table 2⇑ because Table 2⇑ includes all physicians who could be identified from a unique identification number, regardless of where they performed a service, whereas this table uses place of service as a primary determinant of clinician type. Institutional clinicians’ numbers of immunizations generally increased with time, as did their market share of billings, except that nursing home clinicians gave 28% fewer immunizations in 2004 than in 2003. Physicians were the largest vaccinator type at all times, but the absolute number of immunizations varied widely, declining sharply in 2000 and 2004. In 1999, 4 of 5 billed influenza vaccinations were in private physician offices, decreasing in 2004 to only 1 of 2. Mass vaccinators had increased their numbers of shots and proportion of billings gradually until 2004, when the number doubled and market share tripled from the previous year.
Claims for Influenza Immunization Among West Virginia Medicare Beneficiaries Aged 65 Years and Older, by Provider Type, 1999–2004
Table 4⇓ presents information on the mass vaccinators billing for shots to West Virginians from 1999 to 2004. The number of mass vaccinators has increased steadily and is dominated by a few large clinician vaccinators, as more than 90% of the claims originated from clinicians who billed for 100 or more shots. The number of such clinician vaccinators increased by almost one third from 1999, whereas their number of claims doubled, owing principally to a sudden increase between 2003 and 2004.
Mass Vaccinator Clinicians and Claims, West Virginia Medicare Claims for Influenza Immunization, 1999–2004
Table 5⇓ shows the proportion of West Virginians aged 65 years and older who said they received influenza vaccination in the previous 12 months based on the Behavioral Risk Factor Surveillance System survey, compared with the proportion of beneficiaries with claims for vaccine the same year, and the estimated proportion of the population actually immunized based on the same survey of the following year. During the period from 1999 to 2004, the estimated proportion of West Virginia beneficiaries receiving shots from nonbilling clinicians increased from 10.9% to 23.1%, with the largest increase between 2003 and 2004. The estimated number of such beneficiaries in 2004 would have been approximately 60,000.
Medicare Influenza Immunization Rates, West Virginia, 1993–2004
DISCUSSION
This study describes physician practice performance longitudinally in a panel of physicians who submitted 25 or more claims for influenza immunization of Medicare beneficiaries in a single year. The panel was relatively consistent between 1999 and 2003. Vaccine shortages in 2000 and 2004 appear to have affected physician performance as measured grossly by total numbers of immunizations claimed, and at the practice level by physician continuity measures; the impact was more severe in 2004 than 2000.
Based on Behavioral Risk Factor Surveillance System data, the Centers for Disease Control and Prevention concluded that immunization for high-priority groups in 2004 reached levels approximating historical coverage.12 We doubt that was the case for West Virginia’s Medicare beneficiaries aged 65 years and older, although our analysis does suggest that many patients found alternative suppliers, given the increased quality indicator rate for other clinicians, the market share data, and the estimated increase in the proportion of patients using nonbilling clinicians. Use of alternative vaccinators was not enough, however, to prevent a decline in the population reached, estimated to be at least 8% from its peak in 2002.
We do not know the health impacts of the shortage on West Virginia beneficiaries. In previous work15 study authors have found a higher risk of death for unvaccinated persons with diabetes in the year after the opportunity to immunize; the high prevalence of diabetes in our state makes the potential health impact of influenza vaccine shortage in this population especially troubling.
A more important consequence of the vaccine shortage to primary care quality is disruption of continuity of care. It is generally believed that continuity of care in the ambulatory setting confers important benefits, including improved health and reduced health care costs.16–18 Both in 2000 and in 2004, our evidence indicates substantial disruption of continuity of care from previous patterns. In such circumstances, the most vulnerable individuals, eg, those who lack transportation or who are too chronically ill to locate an alternative clinician, would be the most likely not to get vaccine. Mass vaccinators may be convenient to many, but they lack the outreach and follow-up capability that is known to improve immunization uptake.19 Furthermore, in West Virginia, where mountains, poor roads, and lack of public transportation can make travel difficult, it is not credible that a decline of more than 400 physician practices with available vaccines can be offset by an increase of only 9 mass vaccinator sites.
To attempt to explain a marked decline in physician continuity rates in 2000, we conducted a survey of selected West Virginia physicians in 2002, choosing those whose number of vaccinations had declined from more than 25 to less than 5 between 1999 and 2000.20 Although only 49 of 144 physicians responded to our survey, of that group 10 indicated that they were not planning to resume offering the vaccine because of price and availability issues. That finding was consistent with the slow recovery of physician vaccinator numbers in 2001 and subsequent years. How a small decline in numbers will translate into behavior after the 2004 disaster is open to speculation. At a minimum, we might expect several years of performance recovery. For example, after the suspension of the birth dose of hepatitis B vaccine was lifted because a thimerosal-free formulation became available, Orum and colleagues documented a 35% decrease in hospital nurseries that routinely offered hepatitis B immunization 1 year after the recommendations were made.21 Similarly discouraged physicians could create a hole in the public health infrastructure, reducing availability and potentially reducing vaccine coverage for years to come.
Reversing these trends will require intervention at the policy level. Physicians have told us they need a predicable supply of vaccine at a reasonable price if they are to continue giving influenza immunizations to their patients. There is a working model for such a program: the Vaccine for Children (VFC) program, which now provides some 40% of all vaccine used for routine immunizations of children in the United States. According to Centers for Disease Control and Prevention, “by decreasing referrals to public health departments, the VFC program has improved the continuity of care, promoted the ‘medical home’ concept, and contributed to high vaccination coverage levels.”22 When will we have a Vaccine for Adults program?
Limitations
The study was limited to physicians serving fee-for-service Medicare beneficiaries in a single state and might not be applicable to the entire country or to the managed care population. Even so, we know of no reason to expect that a physician in an open-panel managed care plan would treat managed care patients differently from fee-for-service patients when there are vaccine shortages. We also have no reason to believe that West Virginia’s vaccine shortage was markedly more or less severe than elsewhere in the country.
Estimation of nonbilling clinicians depends on whether the sensitivity and specificity of findings from another survey can be applied to the Behavioral Risk Factor Surveillance System survey data. Other researchers have determined different specificity of survey data when compared with actual records, eg, Zimmerman and colleagues,23 but their lower specificity yielded negative rates of individuals vaccinated during some years in West Virginia and was thus clearly not applicable, whereas the estimates used were at least consistent and plausible. The low specificity of the Zimmerman et al study may be a consequence of using medical record abstraction in an open system, and could also reflect use of nonbilling clinicians, whereas MacDonald et al captured managed care organization patient data.
Our findings add to the body of literature that documents the multiple public health impacts of vaccine shortages. Delays and shortages in influenza vaccine had a marked negative effect on West Virginia primary care physicians’ ability to provide this important preventive service to their patients. Many, but not all, patients received vaccine from alternative clinicians, most commonly mass vaccinators. Physician continuity appears to be especially sensitive to influenza vaccine supply disruption.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: This material was prepared by the West Virginia Medical Institute (WVMI), the Medicare Quality Improvement Organization for West Virginia, under contract with the Centers for Medicare & Medicaid Services, an agency of the US Department of Health and Human Services, publication No. 8SOW-WV-1D-06-04. The contents presented do not necessarily reflect Centers for Medicare & Medicaid Services policy.
Portions of this study were presented as Physician Response to Influenza Vaccine Price, Supply and Delivery During the 2000–2001 Flu Season: Discouraged Providers Speak Out, at the Tri-Regional Conference, St. Petersburg Beach, FL, June 12, 2003; as the poster Wipeout: Impact of Flu Vaccine Shortage on Physician Offices at the Preventive Medicine 2006 meeting, Reno, February 2006; and as Wipeout: Impact of Flu Vaccine Shortage on Physician Offices, at the Tri-Regional Conference, St. Petersburg Beach, FL, June 16, 2006.
- Received for publication June 12, 2006.
- Revision received September 8, 2006.
- Accepted for publication September 27, 2006.
- © 2006 Annals of Family Medicine, Inc.




{kind=link}