
Abstract
PURPOSE The possible mechanisms of action of emergency contraception (EC) include preventing ovulation, fertilization, or implantation of an embryo. Differences in the use of terminology between medical personnel and the general public could be misleading to patients who would use EC. This cross-sectional survey evaluated women’s beliefs regarding pregnancy and EC’s possible mechanisms of actions.
METHODS An anonymous questionnaire was developed and pilot tested for an appropriate reading level and ease of analysis. It collected information on demographics and beliefs about pregnancy and EC. During an 8-week period, the questionnaire was given to a convenience sample of female patients aged 18 to 50 years visiting 2 academic family medicine clinics in the southeastern United States. Descriptive statistics and logistic regression models were used for analysis.
RESULTS A total of 178 women completed questionnaires. Nearly one-half (47%) of respondents believed that pregnancy begins with fertilization; however, less than one-third (30%) believed that life begins with fertilization. Thirty-eight percent of respondents stated that they would use EC only if they believed it worked before fertilization or implantation. Generally similar proportions thought that EC works before fertilization (24%) and before implantation (36%), or were unsure about when it works (34%). Younger age was associated with higher odds of believing that EC works before fertilization; none of the other demographic factors studied conferred either higher or lower odds.
CONCLUSIONS Many women are uninformed about the possible mechanisms of action of EC, and we found no reliable predictors for those who were better informed. This study raises questions regarding women’s understanding of EC and demonstrates the need to better educate them about its possible mechanisms of action.
- Emergency contraception
- postcoital contraceptives
- Plan B
- morning-after pill
- pharmacology: mechanism of action
- unwanted pregnancies
- decision making
- informed consent
- patient education
INTRODUCTION
Emergency contraception (EC) is defined as any method women can use after intercourse to prevent pregnancy.1 The differing methods of EC include the use of intrauterine devices and hormone pills, such as the over-the-counter hormonal method known as Plan B.2 Several mechanisms of action have been suggested in the literature for the effectiveness of EC. One possible mechanism of action is the inhibition or delay of ovulation.3–6 A second possible mechanism is a histologic or biochemical alteration of the endometrium that impairs endometrial receptivity to implantation of a fertilized egg.4,7–13 Other studies, however, dispute this claim and suggest that there is no effect on the endometrium.3,14,15 Despite the other suggested mechanisms of action of EC, prevention of implantation is accepted as a possible mechanism and is listed as such in major drug databases16 and the Plan B package insert.17
Patient understanding of the terminology surrounding the mechanisms of action of EC has not been previously studied. Differences in the understanding of terminology between patients and physicians could raise questions regarding the quality of informed consent when patients are told that EC will not act as an abortifacient and will not work once a woman is pregnant. One study looked at the acceptance and use of EC with a standardized counseling intervention and found that one-half of the women who received counseling accepted a prescription for EC in advance of a possible need for EC.18 This counseling did not change their overall use of EC, however.
Additionally, the topic of EC involves moral implications for patients concerning their beliefs about the beginning of life. A public opinion poll of more than 15,000 people showed that almost 50% of the population believe that life begins at conception, or when the sperm and egg join.19
In this study, we investigated women’s beliefs surrounding conception and the beginning of pregnancy. We also evaluated women’s willingness to use EC based on its possible mechanisms of action.
METHODS
This cross-sectional survey took place in 2 academic family medicine clinics in the southeastern United States. One clinic predominately serves an urban population and is staffed by medical school faculty. The other clinic is in a suburban area and is staffed primarily by family medicine residents. The survey was conducted during an 8-week period (February through April and October through November) in 2006.
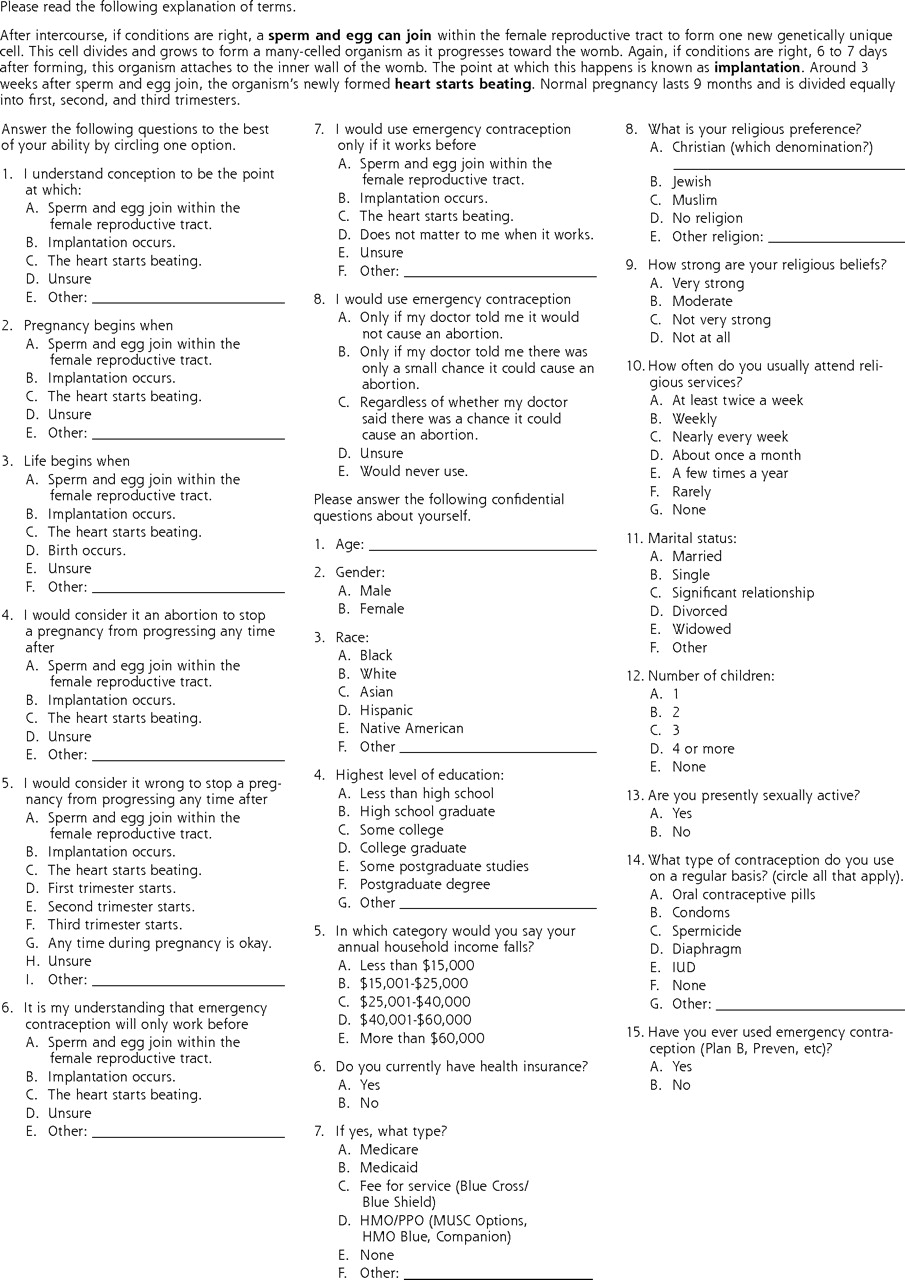
We developed and pilot tested a questionnaire for an appropriate (6th-grade) reading level and for ease of analysis. The questionnaire (Figure 1⇓) was approved as exempt research by the Institutional Review Board at the Medical University of South Carolina. It was administered anonymously to a convenience sample of female patients by the clinic registration staff. Participation was restricted to women aged 18 to 50 years.
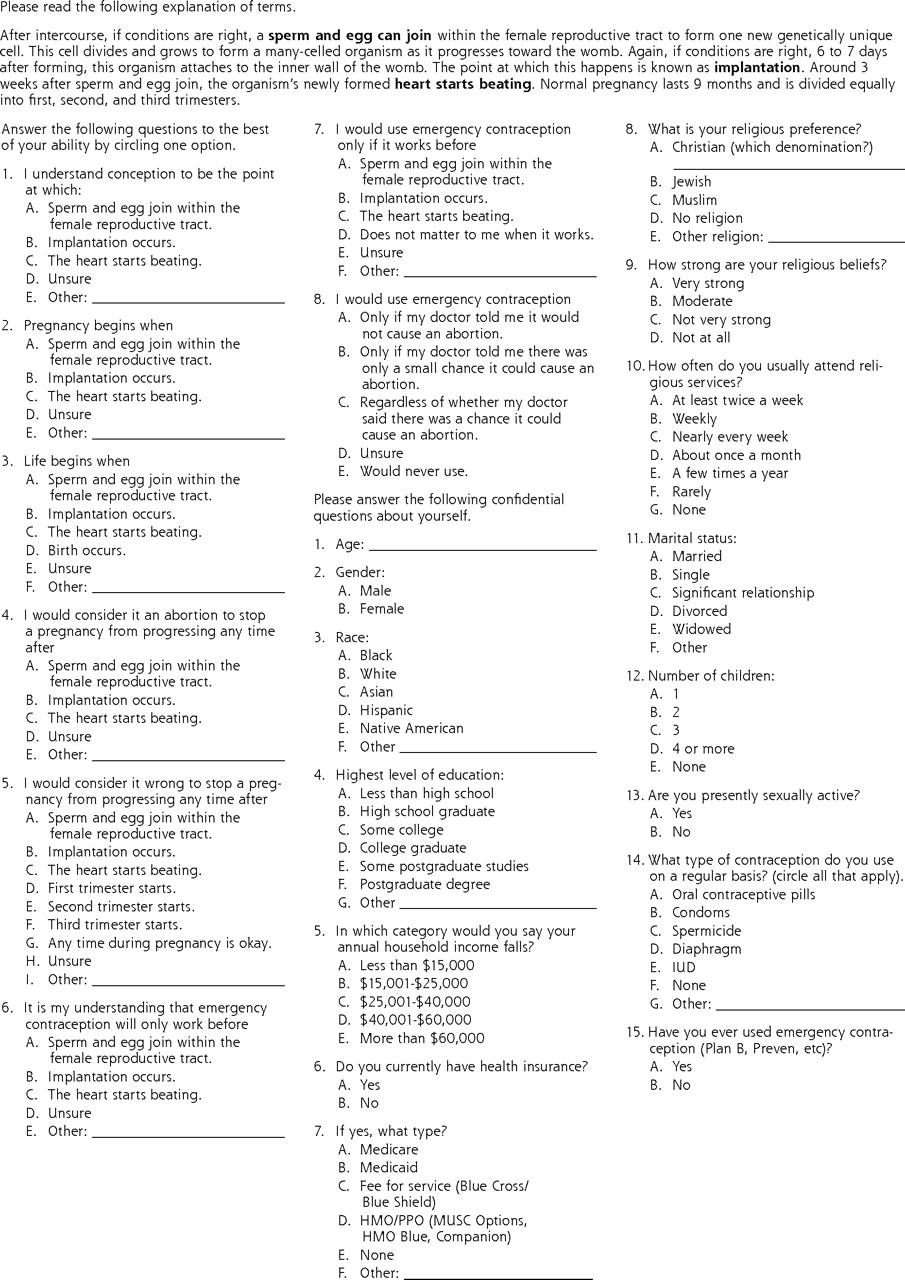
Questionnaire.
HMO = health maintenance organization; PPO = preferred provider organization; MUSC = Medical University of South Carolina; IUD = intrauterine device.
Some questions asked patients about their beliefs regarding the beginning of life, conception, and pregnancy. Other questions were designed to gain insight into patients’ understanding of the possible mechanisms of action of EC. The questionnaire also requested demographic information, including respondents’ age, sex, race, education, income, marital status, children, religious affiliation, strength of religious belief, and any use of contraception.
The data were analyzed with SAS software (SAS Institute, Cary, North Carolina) and by the use of descriptive statistics and logistic regression analysis.
RESULTS
A total of 178 women completed questionnaires. The demographic characteristics of the respondents are shown in Table 1⇓. Compared with clinic patients overall, respondents were younger but of similar races.
Demographic Characteristics of Survey Respondents (N = 178)
Table 2⇓ shows the responses to the questions about conception, pregnancy, and EC. The majority (81%) of respondents agreed that conception occurs when the sperm and egg join. The respondents’ beliefs were split, however, regarding when pregnancy begins and when life begins; nearly one-half (47%) believed that pregnancy begins with fertilization, but less than one-third (30%) believed that life begins at that point. There was no majority belief on when a respondent would use EC in the process of fetal development. Thirty-eight percent of respondents stated that they would use EC only if they believed it worked before fertilization or implantation, and a large proportion (42%) of respondents were unsure of how their potential use of EC would change based on a physician’s comments about when it worked during fetal development.
Respondents’ Answers to Questions on Pregnancy and Emergency Contraception (N = 178)
Table 3⇓ shows the results from the logistic regression analysis. Women with incomes of less than $40,000 were more likely to believe that life begins at the joining of sperm and egg than women with higher incomes. Additionally, women aged 25 years or younger were more likely to think that EC works before the egg and sperm join than older women. There were no significant differences in the perception of abortion or the use of EC based on age, race, income, education, or strength of religious beliefs (data not shown).
Logistic Regression Analysis of Beliefs Regarding Beginning of Life and Emergency Contraception
DISCUSSION
Many of the participants in this study indicated that use of EC would be acceptable to them. Responses suggested, however, that the majority of women surveyed did not know that one possible mechanism of action of EC is to prevent implantation of a fertilized ovum. Although 30% of respondents believed that life begins at fertilization of the egg by sperm, respondents had different beliefs regarding their potential use of EC. These results suggest that women may not fully understand the possible mechanisms of action of EC. This lack of understanding may especially be true for younger women, who may be more likely to use EC.20
Debate over the availability of EC has been quite intensive. Its use by prescription led to a call by pharmacists for the concept of “ethical refusal,” which would allow them to not fill prescriptions if doing so violated their moral beliefs. Some pharmacists went so far as to hold the prescription so that it could not be taken to another pharmacy to be filled.21 In addition, when the Food and Drug Administration (FDA) considered making this an over-the-counter product, a high-level FDA staffer resigned citing the prolonged length of time the product was taking to reach pharmacy shelves because of moral objections of some political entities.22 Our results are congruent with this controversy and reflect the moral debate currently occurring in the United States regarding various methods of abortion.
There are limitations to this study. First, we interviewed only women between the ages of 18 and 50 years who sought medical care in a family medicine office. Women in the general public or women who have used EC in the past may have different perspectives. Teenagers may also have different views but were excluded from this study because of concerns about informed consent by the institutional review board. We do not know the total number of questionnaires distributed and therefore cannot assess the response rate or potential responder bias. Second, the questionnaire was not used previously and was not tested for intrarater reliability. This shortcoming is evidenced by the different percentages of women stating they would never use EC when asked in separate questions. Although our instrument was pilot tested for readability, the development of a more reliable instrument may have yielded different results.
In conclusion, these results raise questions regarding patients’ understanding of issues surrounding EC. Physicians and pharmacists should be careful when discussing contraception, as patients’ beliefs differ greatly when discussing this issue. There is also the potential for misunderstanding the possible mechanisms of action of EC; therefore, more appropriate consent processes and patient education materials should be developed so that women can feel confident that their use of EC is consistent with their moral beliefs.
Footnotes
-
Conflicts of interest: none reported
- Received for publication March 5, 2007.
- Revision received July 20, 2007.
- Accepted for publication August 2, 2007.
- © 2008 Annals of Family Medicine, Inc.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.