
Article Figures & Data
Figures
- Figure 1.
Trial profile.
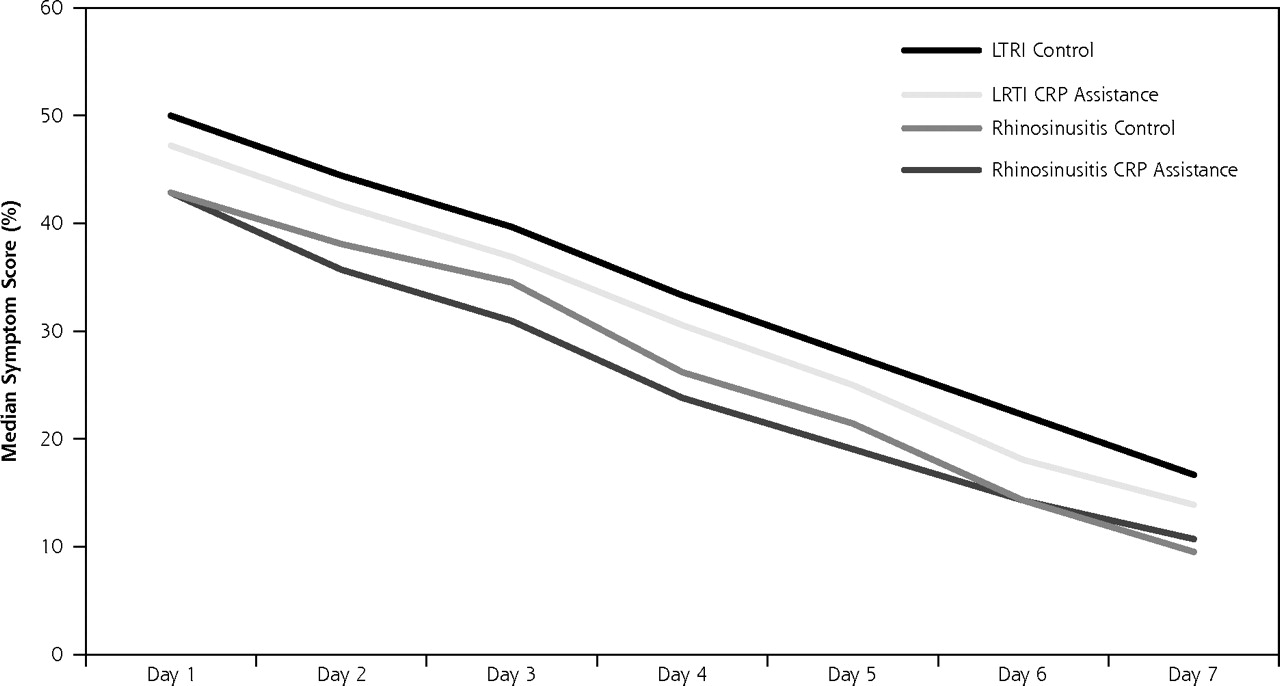
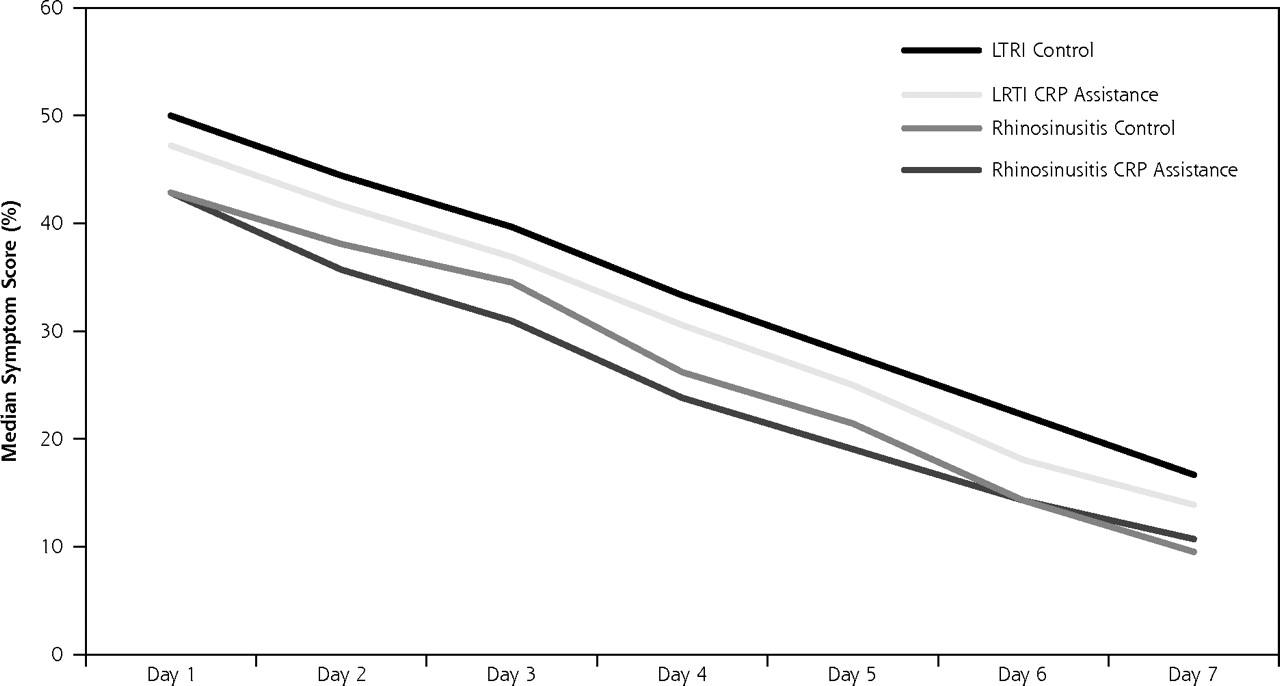
- Figure 2.
Median symptom scores per group during first week after index consultation.
CRP = C-reactive protein; LTRI = lower respiratory tract infection.
Symptom scores for LRTI were calculated by summing and deriving percentage total scores for 6 symptoms: cough, phlegm, sleeping problems, dyspnea, degree of illness, and limitations in daily activities. Symptom scores for rhinosinusitis were calculated by summing and deriving percentage total scores for 7 symptoms: rhinorrhea, blocked nose, dental pain, headache, pain at bending over, degree of illness, and limitations in daily activities.
Median symptom scores of intervention and control groups were not signifi cantly different at any day in week 1, nor when analyzed using area under the curve.

Tables
Characteristic CRP Assistance Control COPD=chronic obstructive pulmonary disease; FP=family physician; IQR=interquartile range; VAS=visual analog scale. a There were 106 responses from both groups for education level. b Scored on a range from 0–100 (with 100 being most severe). Demographics n=129 n=129 Female, % (n) 68.2 (88) 70.5 (91) Age, mean (SD), y 43.0 (13.4) 45.5 (14.0) Lower education, % (n)a 29.2 (31) 19.8 (21) Secondary education, % (n)a 43.4 (46) 42.5 (45) Higher education, % (n)a 27.4 (29) 37.7 (40) Current smoking, % (n) 30.8 (33) 25.5 (27) Comorbidity n=129 n=129 COPD, % (n) 3.9 (5) 2.3 (3) Asthma, % (n) 7.8 (10) 7.0 (9) Allergic rhinitis, % (n) 10.1 (13) 9.3 (12) Diabetes mellitus, % (n) 7.0 (9) 3.1 (4) Heart disease, % (n) 4.7 (6) 6.2 (8) Lower respiratory tract infection, n n=56 n=51 Shortness of breath, % (n) 66.1 (37) 58.8 (30) Wheezing, % (n) 39.3 (22) 29.4 (15) Chest pain, % (n) 51.8 (29) 56.9 (29) Auscultation abnormalities, % (n) 44.6 (25) 41.2 (21) Fever, % (n) 48.2 (27) 49.0 (25) Perspiring, % (n) 51.8 (29) 41.2 (21) Headache, % (n) 32.1 (18) 43.1 (22) Myalgia, % (n) 46.4 (26) 49.0 (25) Generally feeling unwell, % (n) 75.0 (42) 78.4 (40) Duration of symptoms, mean (SD), d 8.07 (5.12) 8.82 (6.16) Duration of symptoms, median (IQR), d 7 (5–14) 7 (4–14) VAS illness severity score by physician, mean (mm, SD)b 46.16 (22.92) 42.07 (23.07) Rhinosinusitis n=73 n=78 History of rhinorrhea, % (n) 71.2 (52) 76.9 (60) Purulent rhinorrhea, % (n) 52.1 (38) 56.4 (44) Blocked nose, % (n) 78.1 (57) 75.6 (59) Unilateral facial pain, % (n) 53.4 (39) 56.4 (44) Headache, % (n) 69.9 (51) 76.9 (60) Dental pain, % (n) 34.2 (25) 28.2 (22) Pain at chewing, % (n) 19.2 (14) 10.3 (8) Pain at bending over, % (n) 60.3 (44) 66.7 (52) Worsening symptoms after initial improvement, % (n) 19.2 (14) 25.6 (20) Duration of symptoms, mean (SD), d 9.28 (6.70) 10.04 (6.85) Duration of symptoms, median (IQR), d 7 (4–14) 8 (5–14) VAS illness severity score by physician, mean (mm, SD)b 40.61 (22.28) 40.51 (21.05) - Table 2.
Mean and Median C-Reactive Protein Values at Index Consultation and Number of Patients Within CRP Categories
CRP Measure All Patients n=258 CRP Assistance n=129 Control n=129 P Valuea CRP=C-reactive protein; IQR=interquartile range. a Difference between CRP vs control calculated using Mann-Whitney U for nonparametric testing. Mean (SD), mg/L 34.17 (37.33) 34.89 (38.41) 33.46 (36.36) Median (IQR), mg/L 18 (<8–46) 17 (<8–52) 19 (<8–42) .88 Minimum-maximum, mg/L <8->160 <8–>160 <8–>160 0–20 mg/L, % (n) 54.3 (140) 56.6 (73) 51.9 (67) 21–50 mg/L, % (n) 24.0 (62) 17.8 (23) 30.2 (39) 51–100 mg/L, % (n) 14.3 (37) 17.1 (22) 11.6 (15) >100 mg/L, % (n) 7.4 (19) 8.5 (11) 6.2 (8) - Table 3.
Effects of Intervention on Antibiotic Use After the Index Consultation (by CRP Category) and Within a 28-Day Follow-Up. Exploratory Data on Antibiotic Use Per Respiratory Tract Infection
Antibiotic Use CRP Assistance % (n) Control % (n) RRa 95% CI CI=confidence interval; CRP = C-reactive protein; LRTI = lower respiratory tract infection; RR = relative risk. Note: Statistical testing was not performed on the exploratory data on antibiotic use per respiratory tract infections, as this trial was designed to detect differences between the total group of patients per group. a Relative risks corrected for clustering. After index consultation 43.4 (56/129) 56.6 (73/129) 0.77 0.56–0.98 Rhinosinusitis 45.2 (33/73) 60.3 (47/78) LRTI 41.1 (23/56) 51.0 (26/51) Within 28-day follow-up 52.7 (68/129) 65.1 (84/129) 0.81 0.62–0.99 Rhinosinusitis 57.5 (42/73) 69.2 (54/78) LRTI 46.4 (26/56) 58.8 (30/51) By CRP category 0–20 mg/L (n = 140) 26.0 (19/73) 49.3 (33/67) 21–50 mg/L (n = 62) 56.5 (13/23) 59.0 (23/39) 51–100 mg/L (n = 37) 68.2 (15/22) 66.7 (10/15) >100 mg/L (n = 19) 81.8 (9/11) 87.5 (7/8) - Table 4.
Effects of Interventions on Patient-Reported Recovery and Secondary Outcomes (Assessed After the Index Consultation)
Outcomes CRP Assistance Control P Valuea IQR=interquartile range. a Calculated using χ2 and Mann-Whitney U where applicable. b Maximum score = 12. Lower respiratory tract infection Patients feeling recovered on day 7, % (n/n) 23.5 (12/51) 18.4 (9/49) .53 Patient reported time to full recovery Median (IQR) 15.5 (9.5–28) 20 (13.3– >28) .21 Mean (SD) 17.5 (9.2) 19.8 (9.5) Rhinosinusitis Patients feeling recovered on day 7, % (n/n) 22.4 (15/67) 28.9 (22/76) .37 Patient reported time to full recovery, h Median (IQR) 14 (10–28) 14 (7– >28) .77 Mean (SD) 17.3 (9.3) 16.6 (9.9) All patients (n = 258) Reconsult, % (n/n) 25.6 (33/129) 17.8 (23/129) .13 Satisfaction: patient at least very satisfied, % (n/n) 76.3 (90/118) 63.2 (79/125) .03 Future consultation intention: patient likely to reconsult, % (n/n) 74.8 (86/115) 61.0 (75/123) .02 Patient enablement scoreb .58 Median (IQR) 2 (4) 2 (4) Mean (SD) 2.5 (2.6) 2.3 (2.4)
The Article in Brief
Point-of-Care C-Reactive Protein Testing and Antibiotic Prescribing for Respiratory Tract Infections: A Randomized Controlled Trial
Jochen W.L Cals , and colleagues
Background Antibiotics are often overprescribed for patients with respiratory infections and rhinosinusitis. Measuring C-reactive protein, which increases quickly when an inflammation is present, can help determine which patients will benefit from antibiotic treatment. This study looks at whether C-reactive protein testing during patient visits for respiratory infections and rhinosinusitis helps clinicians make better prescribing decisions.
What This Study Found Testing for C-reactive protein during patient visits for respiratory infections and rhinosinusitis led to reduced antibiotic use and did not have a negative effect on patients' recovery. Patient satisfaction with care was higher when C-reactive protein testing was used.
Implications
- C-reactive protein testing during patient visits for respiratory infection and rhinosinusitis may be a useful strategy to decrease antibiotic use and increase patient satisfaction without compromising patient health.
Annals Journal Club:
Mar/Apr 2010
Point-of-Care C-Reactive Protein to Assist Antibiotic Prescribing for Respiratory Tract Infections
The Annals of Family Medicine encourages readers to develop a learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care and then acting on those discussions.1How it Works
In each issue, the Annals selects an article or articles and provides discussion tips and questions. We encourage you to take a RADICAL approach to these materials and to post a summary of your conversation in our online discussion. (Open the article online and click on "TRACK Comments: Submit a response.") You can find discussion questions and more information online at: http://www.AnnFamMed.org/AJC/.
CURRENT SELECTION
Article for Discussion
- Cals JWL, Schot MJC, de Jong SAM, Dinant GJ, Hopstaken RM. Point-of-care C-reactive protein testing and antibiotic prescribing for respiratory tract infections: a randomized controlled trial. Ann Fam Med. 2010; 8(2):124-133.
Discussion Tips
In the last issue Annals journal club assessed a systematic review of an uncommon treatment for a particular kind of respiratory infection. This issue�s journal club provides an opportunity to consider a new adjunctive aid to decisions about antibiotic prescribing for a wider range of respiratory tract infections.Discussion Questions
- What questions are addressed by this article? How do the questions fit with what already is known about diagnostic tests and delayed prescriptions for respiratory infections?
- How does the way the questions were framed affect the utility of the findings?
- How strong is the study design for answering the questions?
- To what degree can the findings be accounted for by:
- How study participants were selected or excluded?
- How the main variables were measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a 3rd factor)?
- Chance?
- How do the methods match up against the CONSORT Guidelines for clinical trials: http://www.consort-statement.org/consort-statement/?
- What are the main study findings across the different outcome measures?
- What can we learn from the subgroup analyses?
- Does the study funding affect your confidence in the findings? Does the registration of the trial increase your confidence?2 (See: http://www.trialregister.nl/trialreg/admin/rctview.asp?TC=1112.)
- How comparable are the study populations to your practice? What is your judgment about the transportability of the findings?
- How (if at all) could this study change your practice?
- What important researchable questions remain?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals journal club: It�s time to get RADICAL. Ann Fam Med. 2006;4(3):196-197. http://annfammed.org/cgi/content/full/4/3/196.
- De Angelis C, Drazen JM, Frizelle, JM, et al. Clinical trial registration: a statement from the International Committee of Medical Journal Editors. N Engl J Med. 2004; 351:1250-1251.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- How, why and when are delayed (back-up) antibiotic prescriptions used in primary care? A realist review integrating concepts of uncertainty in healthcare
- Determinants of inappropriate antibiotic prescription in primary care in developed countries with general practitioners as gatekeepers: a systematic review and construction of a framework
- C-reactive protein cut-offs used for acute respiratory infections in Danish general practice
- Implementation of C-reactive protein point of care testing to improve antibiotic targeting in respiratory illness in Vietnamese primary care (ICAT): a study protocol for a cluster randomised controlled trial
- Liver Function in Novel Coronavirus Disease (COVID-19): A Systematic Review and Meta-Analysis
- Challenges and opportunities for antibiotic stewardship among preterm infants
- Antibiotic Prescribing for Acute Respiratory Tract Infections 12 Months After Communication and CRP Training: A Randomized Trial
- Accuracy of Signs and Symptoms for the Diagnosis of Acute Rhinosinusitis and Acute Bacterial Rhinosinusitis
- Impact of point-of-care C reactive protein in ambulatory care: a systematic review and meta-analysis
- Use of C-reactive protein to tailor antibiotic use: a systematic review and meta-analysis
- Funding and policy incentives to encourage implementation of point-of-care C-reactive protein testing for lower respiratory tract infection in NHS primary care: a mixed-methods evaluation
- C-reactive protein: guiding antibiotic prescribing decisions at the point of care
- Patient Willingness to Have Tests to Guide Antibiotic Use for Respiratory Tract Infections: From the WWAMI Region Practice and Research Network (WPRN)
- Proposed Clinical Decision Rules to Diagnose Acute Rhinosinusitis Among Adults in Primary Care
- Qualitative study of primary care clinicians views on point-of-care testing for C-reactive protein for acute respiratory tract infections in family medicine
- Point-of-care CRP testing in the diagnosis of pneumonia in adults
- Diagnosis of acute rhinosinusitis in primary care: a systematic review of test accuracy
- Narrative review of primary care point-of-care testing (POCT) and antibacterial use in respiratory tract infection (RTI)
- Clinical presentation and microbiological diagnosis in paediatric respiratory tract infection: a systematic review
- Current and future use of point-of-care tests in primary care: an international survey in Australia, Belgium, The Netherlands, the UK and the USA
- Association between point-of-care CRP testing and antibiotic prescribing in respiratory tract infections: a systematic review and meta-analysis of primary care studies
- Antibiotic prescribing and C-reactive protein testing for pulmonary infections in patients with intellectual disabilities
- Enhanced Communication Skills and C-reactive Protein Point-of-Care Testing for Respiratory Tract Infection: 3.5-year Follow-up of a Cluster Randomized Trial
- Risks and Benefits Associated With Antibiotic Use for Acute Respiratory Infections: A Cohort Study
- Predictors of clinical outcome in a national hospitalised cohort across both waves of the influenza A/H1N1 pandemic 2009-2010 in the UK
- Interventions to reduce antibiotic prescription for lower respiratory tract infections: Happy Audit study
- Why do children hospitalised with pneumonia not receive antibiotics in primary care?
- GPs' views in five European countries of interventions to promote prudent antibiotic use
- Multidisciplinary Discourse
- Tip of the Iceberg
- Point-of-care C-reactive protein to assist antibiotic prescribing for respiratory tract infections.
- In This Issue: Relationships Count for Patients and Doctors Alike