
Abstract
PURPOSE Previous studies have reported inconsistent findings regarding the association between the use of acid-suppressive drugs such as proton pump inhibitors (PPIs) and histamine 2 receptor antagonists (H2RAs) and fracture risk. We investigated this association using meta-analysis.
METHODS We searched MEDLINE (PubMed), EMBASE, and the Cochrane Library from inception through December 2010 using common key words. We included case-control, nested case-control, and cohort studies. Two evaluators independently reviewed and selected articles. We determined pooled effect estimates by using random-effects meta-analysis, because of heterogeneity.
RESULTS Of 1,809 articles meeting our initial inclusion criteria, 5 case-control studies, 3 nested case-control studies, and 3 cohort studies were included in the final analyses. The pooled odds ratio (OR) for fracture was 1.29 (95% confidence interval [CI], 1.18–1.41) with use of PPIs and 1.10 (95% CI, 0.99–1.23) with use of H2RAs when compared with nonuse of the respective medications. Long-term use of PPIs increased the risk of any fracture (adjusted OR = 1.30; 95% CI, 1.15–1.48) and hip fracture risk (adjusted OR = 1.34; 95% CI, 1.09–1.66), whereas long-term H2RA use was not significantly associated with fracture risk.
CONCLUSIONS We found possible evidence linking PPI use to an increased risk of fracture, but no association between H2RA use and fracture risk. Widespread use of PPIs with the potential risk of fracture is of great importance to public health. Clinicians should carefully consider their decision to prescribe PPIs for patients already having an elevated risk of fracture because of age or other factors.
INTRODUCTION
Recently, the medical literature has paid considerable attention to unrecognized adverse effects of commonly used medications and their potential public health impact.1 Osteoporosis is one such potential adverse effect. It is a common and important source of morbidity in the population in general, particularly among older adults. More than 40% of women and 14% of men older than 50 years of age experience fractures related to osteoporosis.2 Osteoporotic fractures of the spine frequently occur in both men and women.3
Acid-suppressive drugs (ASDs) represent the second leading medication worldwide in terms of sales, with the value totaling $26.9 billion in 2005.4 Proton pump inhibitors (PPIs) and histamine 2 receptor antagonists (H2RAs) are the most popular ASDs available, and millions of individuals currently take these medications on a continuous or long-term basis.5 These potent drugs are used to treat various disorders, and indications for long-term maintenance therapy with this drug class continue to expand.6
The relationship between ASD use and bone health remains unclear. Some findings raise the possibility that PPIs may prevent osteoporosis and fractures. Several in vitro and animal studies have suggested that PPIs may decrease bone resorption by inhibiting osteoclastic vacuolar H+/K+ ATPase activity.7–11 Osteoclasts possess proton pumps, which are used during the excretion of H+ ions for bone resorption. Osteoclast-selective PPIs may therefore be used as antiresorptive agents12 with the potential of preventing fractures.13–16 Administration of a selective inhibitor of the osteoclastic vacuolar H+/K+ ATPase prevents bone loss in ovariectomized rats, an animal model representative of postmenopausal osteoporosis.15 As bone resorption is necessary for the development of normal bone microstructure, however, one may speculate that PPI-induced blockade of the osteoclast-associated vacuolar proton pump may actually increase fracture risk.17
It has been reported that ASDs may interfere with bone metabolism and thus increase fracture risk. Some potential mechanisms by which PPI therapy may lead to fractures have been identified. First, the small intestine’s ability to absorb ingested calcium salts depends on pH.18,19 Calcium solubility is believed to be important for its absorption,20 and an acidic environment in the gastrointestinal tract facilitates the release of ionized calcium from insoluble calcium salts.21 Second, impaired calcium absorption might lead to compensatory secondary hyperparathyroidism, which may increase the rate of osteoclastic bone resorption. Third, PPIs may interfere with the resorptive activity of osteoclasts. Without osteoclast activity, old bone cannot be replaced, predisposing patients to fractures.17,22 Further research is required to determine the precise effect of long-term use of PPIs on bone mineral metabolism, however.23 Fourth, gastric parietal cells appear to have a potent endocrine role in secreting estrogens.24–27 Atrophy of the gastric mucosa, observed in patients infected with CagA-positive Helicobacter pylori,28 reduces the number of gastric parietal cells and may decrease local production of estrogens. Estrogens produced in the stomach directly induce expression and production of ghrelin,29,30 which appears to increase bone formation by osteoblasts.31
PPIs target the H+/K+ ATPase of gastric parietal cells and inhibit the final step in gastric proton release.32 Standard doses of these drugs can reduce gastric acid secretion by up to 98% by irreversibly deactivating the proton pump of gastric parietal cells.33 Marked hypochlorhydria, particularly among the elderly population, who might have a decreased clearance of PPIs and be more likely to have hypochlorhydria at baseline because of a higher prevalence of H pylori infection,34,35 could theoretically result in calcium malabsorption.36,37 H2RAs could potentially have similar effects, although they are less potent acid suppressants, blocking 70% of gastric acid production.38
Observational studies have yielded inconclusive results regarding the association between use of ASDs and fracture risk, with reported adjusted odds ratios (ORs) or relative risks (RRs) ranging widely, from 0.88 to 3.10. Some epidemiologic studies have found that PPI therapy is associated with an increased risk of hip fractures,22,23,39–41 whereas a nested case-control study did not find any significant association.42 To our knowledge, no meta-analysis of such studies has been conducted. We therefore investigated the association between the use of PPIs or H2RAs and fracture risk by performing a meta-analysis of observational studies.
METHODS
We followed the MOOSE (Meta-analysis of Observational Studies in Epidemiology) guidelines43 during all stages of design, implementation, and reporting of this meta-analysis.
Literature Search
We searched MEDLINE (PubMed) (inception to December 2010), EMBASE (inception to December 2010), and the Cochrane Library (inception to December 2010) by using common key words related to ASDs and fracture risk. The key words for ASDs were as follows: “H2 blocker or histamine-2 receptor antagonists or cimetidine or ranitidine or famotidine or nizatidine or proton pump inhibitors or proton pumps or omeprazole or Nexium or lansoprazole or rabeprazole or pantoprazole or esomeprazole.” The key words for fracture risk were as follows: “osteoporosis or osteopenia or fracture risk or fractures or fracture rates or bone health or bone metabolism or bone mineral density.” We did not limit the search through use of any restrictions.
Study Selection
We planned to (1) include randomized controlled trials (RCTs) and cohort, nested case-control, and case-control studies that investigated the association between the use of ASDs such as PPIs or H2RAs and fracture risk and (2) develop a list of the types of fracture outcomes reported in the studies with the adjusted ORs or RRs and 95% confidence interval (CIs). Two of the authors (C-S.E. and J-S.A.) independently evaluated the eligibility of all studies retrieved from the databases on the basis of selection criteria.
Data Extraction and Quality Assessment
We extracted data from the selected articles on the following items: the first author’s last name, publication year, country where the study was performed, study design, study period, type of outcome (fracture of the hip, vertebrae, wrist, or any site), type of agent (PPI or H2RA), adjusted OR and RR with CIs, number of variables adjusted for in the analysis, the case individuals and control individuals with or without exposure, and duration of exposure.
Long-term use was defined as use for more than 1 year before the index date. We chose this duration because alterations in fracture risk due to the use of other medications, such as bisphosphonates, thiazide diuretics, and corticosteroids, become apparent after 1 year of exposure.44,45 In studies wherein users did not use the PPI or H2RA for more than 1 year, we chose the longest available period of use.
Two investigators (C-S.E. and S.M.P.) independently extracted data by using a standardized data collection form. We resolved disagreements by mutual discussion and, if required, by consulting a third investigator.
We assessed the methodologic quality of included studies by using the Newcastle-Ottawa Scale (NOS) for determining the quality of case-control and cohort studies in meta-analyses.46 We considered studies having a total score of greater than 7 to be high-quality studies, as standard criteria have not been established and the mean total score for all 11 studies assessed was 7.18.
Main and Subgroup Analyses
We investigated the association between the use of PPIs, H2RAs, or both and the risk of fracture by using adjusted data for the main analyses. We also performed subgroup analyses by type of study (case-control, nested case-control, or cohort study), methodologic quality of the study (high vs low), number of variables used for statistical adjustment (≥5 vs <5), type of agent (PPI vs H2RA), fracture outcome, medication dose, and sex.
Statistical Analysis
We assumed that ORs approximated RRs and therefore combined the study estimates regardless of which measure of association was reported because the incidence of the outcomes of interest was sufficiently rare (<5% per year). Pooled effect estimates were obtained by using random-effects meta-analysis, because of heterogeneity.
We examined the heterogeneity of results across studies by using the Higgins I2, which measures the percentage of total variation across studies.47 The Der-Simonian and Laird method48 for calculating summary measures was used in the random-effects models. We evaluated the publication bias of the studies included in the final analysis by using the Begg funnel plot and the Egger test. We used the Stata SE version 10.1 software package (StataCorp, College Station, Texas) for statistical analysis.
RESULTS
Characteristics of the Included Studies
We originally planned to include RCTs in this meta-analysis; however, as of the end of our search period, no RCTs on this topic had been reported.
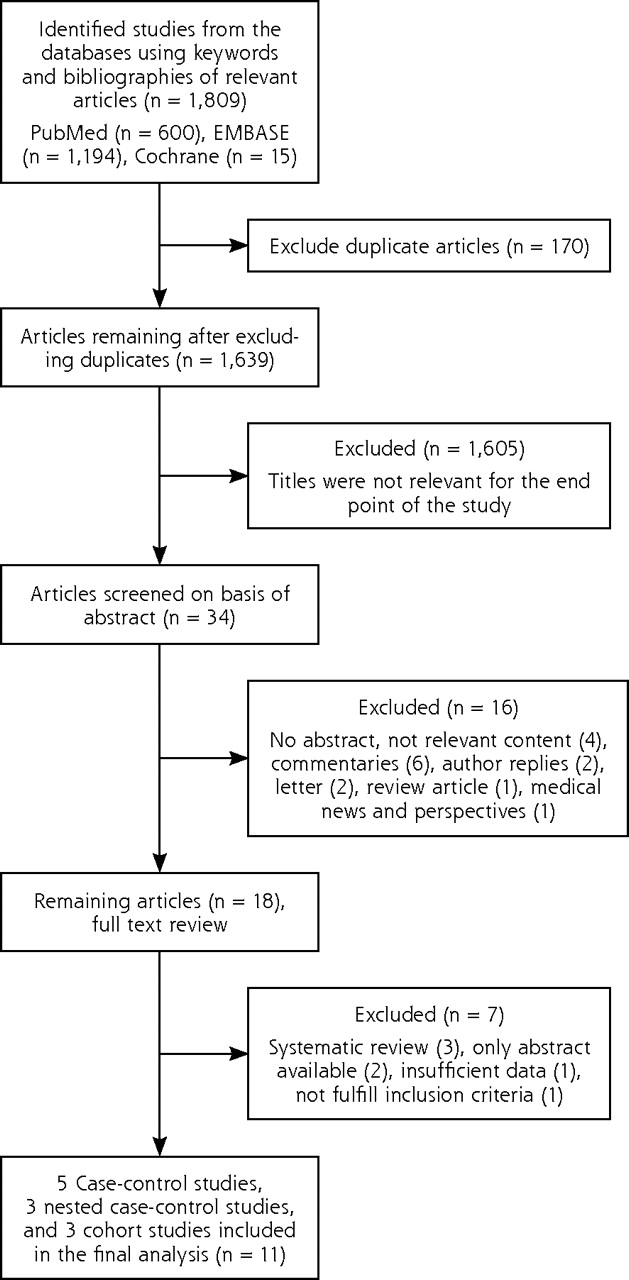
Figure 1⇓ shows how we selected relevant studies for inclusion in the meta-analysis. A total of 1,809 articles were identified by searching the 3 databases. We excluded 170 duplicate articles and an additional 1,621 articles that did not meet the selection criteria. We reviewed the full texts of the remaining 18 articles. Of these, 7 articles were excluded. The remaining 11 studies were included in the final analysis.22,23,39–42,49,50–53

Study flow diagram.
Table 1⇓ summarizes the general characteristics of the 11 studies included in the meta-analysis. We identified 5 case-control studies,23,39,49,52,53 3 nested case-control studies,22,42,50 and 3 cohort studies.40,41,51 The selected studies were published between 1997 and 2011, spanning 14 years. Six studies22,39,40,50–52 evaluated PPIs and H2RAs; 4 studies23,41,42,53 evaluated PPIs only; and 1 study49 evaluated H2RAs only.
Characteristics of Studies Included in the Final Analysis (N = 11)
Main Analysis
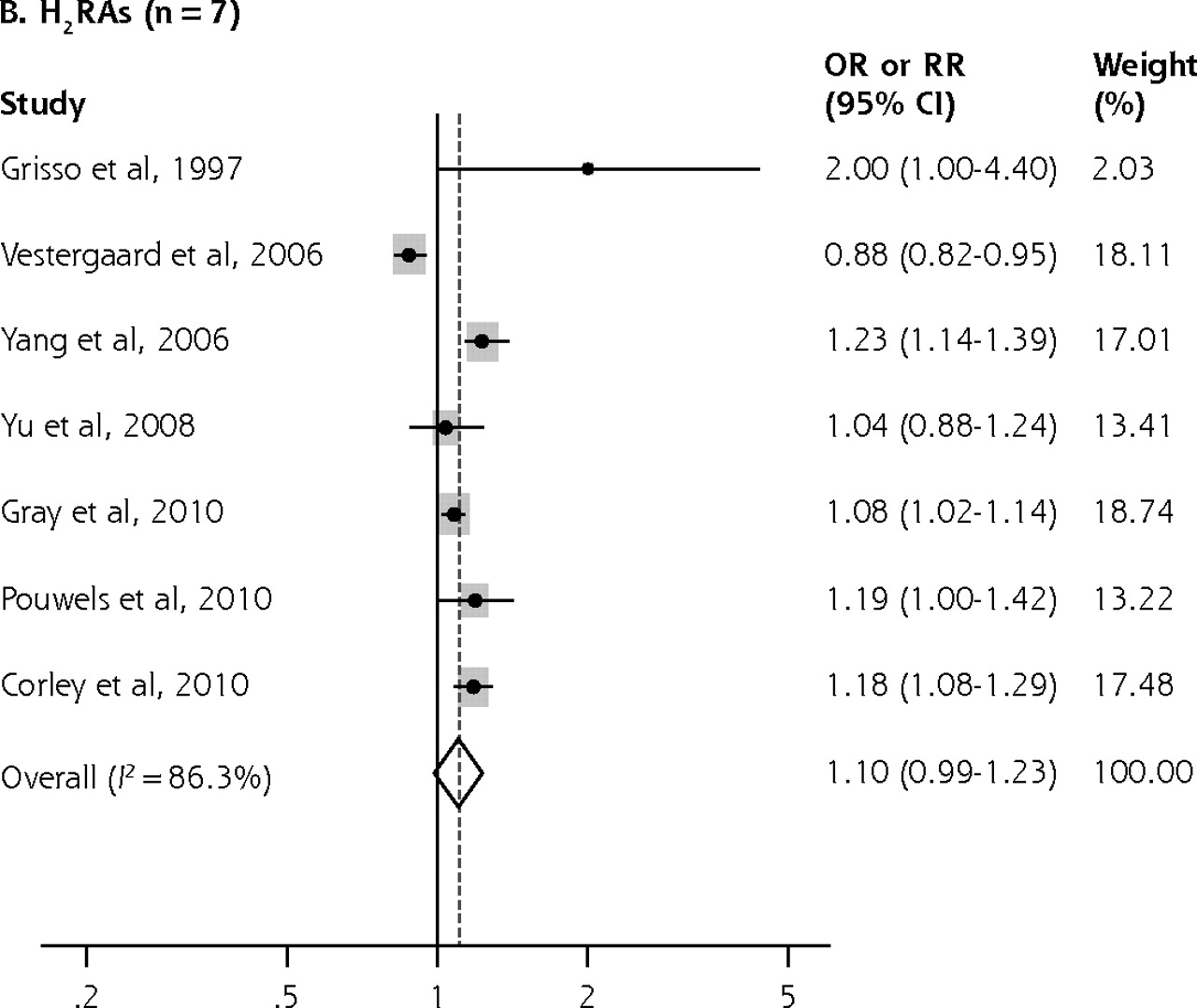
As shown in Figure 2⇓, the overall use of PPIs was associated with a significantly increased risk of any fracture in a random-effects model meta-analysis of 4 case-control studies, 3 nested case-control studies, and 3 cohort studies (adjusted OR = 1.29; 95% CI, 1.18–1.41; I2 = 69.8%; n = 10). Use of H2RAs was not associated with an increased fracture risk, however (adjusted OR = 1.10; 95% CI, 0.99–1.23; I2 = 86.3%; n = 7).


PPIs or H2 RAs use and the combined risk of any fracture in a random-effects model meta-analysis of case-controls studies and cohort studies.
CI=confidence interval; H2RA = histamine 2 receptor antagonist; OR = odds ratio; PPI = proton pump inhibitor; RR = relative risk.
Subgroup Meta-Analyses
Table 2⇓ shows the association between PPIs or H2RAs and the risk of fracture in subgroup meta-analyses.
PPI or H2RA Use and the Risk of Fracture in Subgroup Meta-analyses Using a Random-Effects Model
When studies were grouped by type, we observed a positive association between the use of PPIs and fracture risk in all types, but a positive association between the use of H2RAs and fracture risk only when nested case-control studies were combined (adjusted OR = 1.20; 95% CI, 1.13–1.28; I2 = 0.0%; n = 2) or when cohort studies were combined (adjusted OR = 1.08; 95% CI, 1.02–1.13; I2 = 0.0%; n = 2). In contrast, no significant association was observed in case-control studies (adjusted OR = 1.11; 95% CI, 0.81–1.51; I2 = 85.6%; n = 3).
Grouping of studies by methodologic quality (scores are given in Table 3⇓) showed a significantly increased fracture risk with PPI use in both high-quality studies (adjusted OR = 1.32; 95% CI, 1.18–1.47; I2 = 63.7%; n = 5) and low-quality studies (adjusted OR = 1.25; 95% CI, 1.06–1.48; I2 = 78.7%; n = 5). There was also a significant positive association between H2RA use and fracture risk in high-quality studies (adjusted OR = 1.13; 95% CI, 1.05–1.21; I2 = 40.3%; n = 3) but not in low-quality ones (adjusted OR = 1.09; 95% CI, 0.87–1.38; I2 = 90.6%; n = 4).
Methodologic Quality of Studies, Based on the Newcastle-Ottawa Scale (N = 11)
Grouping studies by the number of adjustment variables revealed a significantly increased fracture risk in those adjusting for at least 5 variables for both PPI use (adjusted OR = 1.36; 95% CI, 1.24–1.49; I2 = 63.0%; n = 6) and H2RA use (adjusted OR = 1.14; 95% CI, 1.06–1.22; I2 = 57.7%; n = 4). In studies adjusting for fewer than 5 variables, there was marginally no association between PPI use and fracture risk (adjusted OR = 1.16; 95% CI, 0.98–1.38; I2 = 66.5%; n = 4), but no significant association between H2RA use and fracture risk (adjusted OR = 1.11; 95% CI, 0.81–1.51; I2 = 85.6%; n = 3).
When we grouped studies by fracture outcome, we found a significant positive association between PPI use and hip fracture risk (adjusted OR = 1.31; 95% CI, 1.11–1.54; I2 = 88.4%; n = 9) and vertebral fracture risk (adjusted OR = 1.56; 95% CI, 1.31–1.85; I2 = 6.3%; n = 3), whereas there was no significant association between PPI use and the risk of other fractures, or between H2RA use and hip and any fracture risk.
In subgroup meta-analyses by duration of use, long-term use of PPIs increased the risk of any fracture (adjusted OR = 1.30; 95% CI, 1.15–1.48; n = 10) and the risk of hip fracture (adjusted OR = 1.34; 95% CI, 1.09–1.66; n = 9). There was no association between long-term use of H2RAs and either of these outcomes.
When we grouped studies by dose, we observed a significantly increased risk of hip fracture for both high-dose use of PPIs (adjusted OR = 1.53; 95% CI, 1.18–1.97; n = 4) and usual-dose use of PPIs (adjusted OR = 1.42; 95% CI, 1.31–1.53; n = 4). In contrast, we found no association with hip fracture for either high-dose or usual-dose use of H2RAs.
Subgroup analyses by sex showed no significant association between PPI or H2RA use and hip fracture risk in men, or hip fracture or vertebral fracture risk in women.
Publication Bias
We found no statistically significant asymmetry in funnel plots, and the result of the Egger test was non-significant. Specifically, the Begg funnel plot was not asymmetrical, and the P value for bias in the Egger test was .45 for PPIs and .43 for H2RAs (data not shown), indicating no significant influence of publication bias among the included studies.
DISCUSSION
In this meta-analysis of observational studies, we found that the use of PPIs was associated with a moderate increase in the risk of fracture compared with nonuse of PPIs, whereas we did not observe any significant association between H2RA use and this risk. Similarly, long-term PPI use and any dose of PPIs increased the risk of fracture in a meta-analysis of all the studies reporting duration of use and dose, whereas neither long-term use and nor use of any dose of H2RAs was significantly associated with fracture risk.
We did not find any significant association between use of H2RAs, which are less potent acid inhibitors than PPIs, and fracture risk. On average, H2RAs block only 70% of gastric acid production, whereas PPIs suppress acid production by up to 98%.33,38,54 More prolonged exposure to H2RAs may be necessary to observe similar effects on fracture risk, but we did not find long-term use of these agents to increase risk. These results suggest that H2RAs and PPIs may have differing effects on bone metabolism. Some studies suggest that H2RAs may have antiresorptive properties55,56 and even increase bone mineral density, which could decrease fracture risk.39 Cimetidine also has been shown to prevent osteoclast differentiation induced by histamine.57,58 Because of the mixed effects of H2RAs on bone health, there have been inconsistent results regarding long-term use of these drugs and fracture risk22,39,42,49 or bone mineral density.59 In contrast, PPIs have been shown to inhibit gastric proton pumps at physiologic concentrations, whereas the inhibition of osteoclast and other tissue H+/K+ ATPase activity, such as osteoclast proton pumps, is much less pronounced.60 We did find, however, that the use of H2RAs was associated with a mild increase in fracture risk in studies having high-quality methodology (NOS score >7) and in studies adjusting for at least 5 variables, but not in studies having low-quality methodology and adjusting for fewer than 5 variables. Further research in this area is needed.
Interestingly, the subgroup meta-analyses by the number of adjustment variables showed a significantly increased risk of fracture for both PPI and H2RA use when the data were adjusted for at least 5 variables. The results for H2RAs conflict with those of Vestergaard et al,39 who reported a statistically significant protective effect with use of these drugs for any fracture and hip fracture. The positive association we found between H2RA use and fracture risk in studies with a high level of statistical adjustment may also be consistent with the marginal association we observed in high-quality studies (NOS score >7).
Yu et al50 showed a possible interaction of PPI use and calcium supplement use on the risk of nonspine fractures in men. In stratified analyses, PPI use was associated with an increase in fracture risk among men who were not taking calcium supplements, but not among men who were taking them. In contrast, no significant interactions were found for fracture outcomes in women. The clinical implication of this finding is that PPIs prescribed along with calcium supplement might be able to prevent osteoporosis in older men.
Kaye and Jick42 restricted the phase 2 part of their study to patients with no major medical risk factors for fracture and found no association of PPI use and fracture. This finding can be interpreted as evidence that PPI use is not associated with a substantially increased risk of fracture. If a causal association between use and fracture risk indeed existed to a clinically relevant degree, one would expect to find this association also in this group of patients with a low a priori fracture risk. It cannot be concluded that PPI use is not associated with an altered fracture risk in patients at high risk of fractures, however, as this patient subset was not included in the phase 2 study. In addition, exclusion of patients with direct risk factors for factures, such as previous fracture and osteoporosis, can be problematic if these diseases are on the causal pathway and not necessarily confounders.61
Our meta-analysis has several strengths. First, it is the most comprehensive meta-analysis on the use of ASDs and fracture risk to date. Second, it examines the associations in greater detail by stratifying by the type of agent (PPI or H2RA) and the type of outcome (hip or vertebral fracture), as well as by dose and duration of use. On the other hand, our meta-analysis also has several limitations. First, observational studies are considered to have greater potential for bias. To compensate for this limitation, we conducted subgroup analysis according to various factors. Second, the Egger test is known to lack power, reducing our ability to detect potential publication bias. Third, we did not have access to individual data on nutrients that might affect the risk of fracture. The dietary habits of ASD users may differ from those of nonusers because of intolerance secondary to gastritis. Furthermore, the dietary acid load can affect bone metabolism. Finally, we could not evaluate the effect of underlying gastric diseases in each patient because these data were not given in each study. Bone alteration may be related to the underlying gastric disease. The prevalence of H pylori infection has been found to be high in men with osteoporosis,62 and this infection may be present in patients taking ASDs. H pylori infection can induce a permanent inflammatory response, that is, a gastric and systemic increase in indexes of inflammation. This mechanism has been implicated in some extragastric manifestations in H pylori–infected patients.62
A major limitation of our meta-analysis of observational studies is the possibility of uncontrolled confounding. Our findings should therefore be confirmed by further prospective studies including RCTs that are designed specifically with large sample sizes and long follow-up durations to test the effect of ASDs on the risk of fracture.
In conclusion, we found that in a meta-analysis of case-control, nested case-control, and cohort studies, PPI use modestly increased fracture risk, whereas H2RA use did not. An OR or RR of less than 2, as seen in this study, is generally considered to be a weak or low-magnitude association. Nevertheless, even small increases in these values for common diseases may have important public health implications. Clinicians should therefore carefully consider their decision to prescribe PPIs for patients at elevated risk for fracture, especially women older than 65 years of age.63–65 It is not necessary to treat patients to the point of an achlorhydric state to resolve acid reflux symptoms, so we recommend that drug doses be chosen thoughtfully with consideration of what is necessary to achieve desired therapeutic goals.
Footnotes
-
↵* Drs Park and Myung contributed equally to this paper as corresponding authors.
-
Conflicts of interest: authors report none.
-
Funding support: This work was supported by a National Research Foundation of Korea (NRF) Grant funded by the Korean government (grant 2010-0004429).
- Received for publication October 11, 2010.
- Revision received December 16, 2010.
- Accepted for publication January 6, 2011.
- © 2011 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}
{kind=link}