
Article Figures & Data
Figures
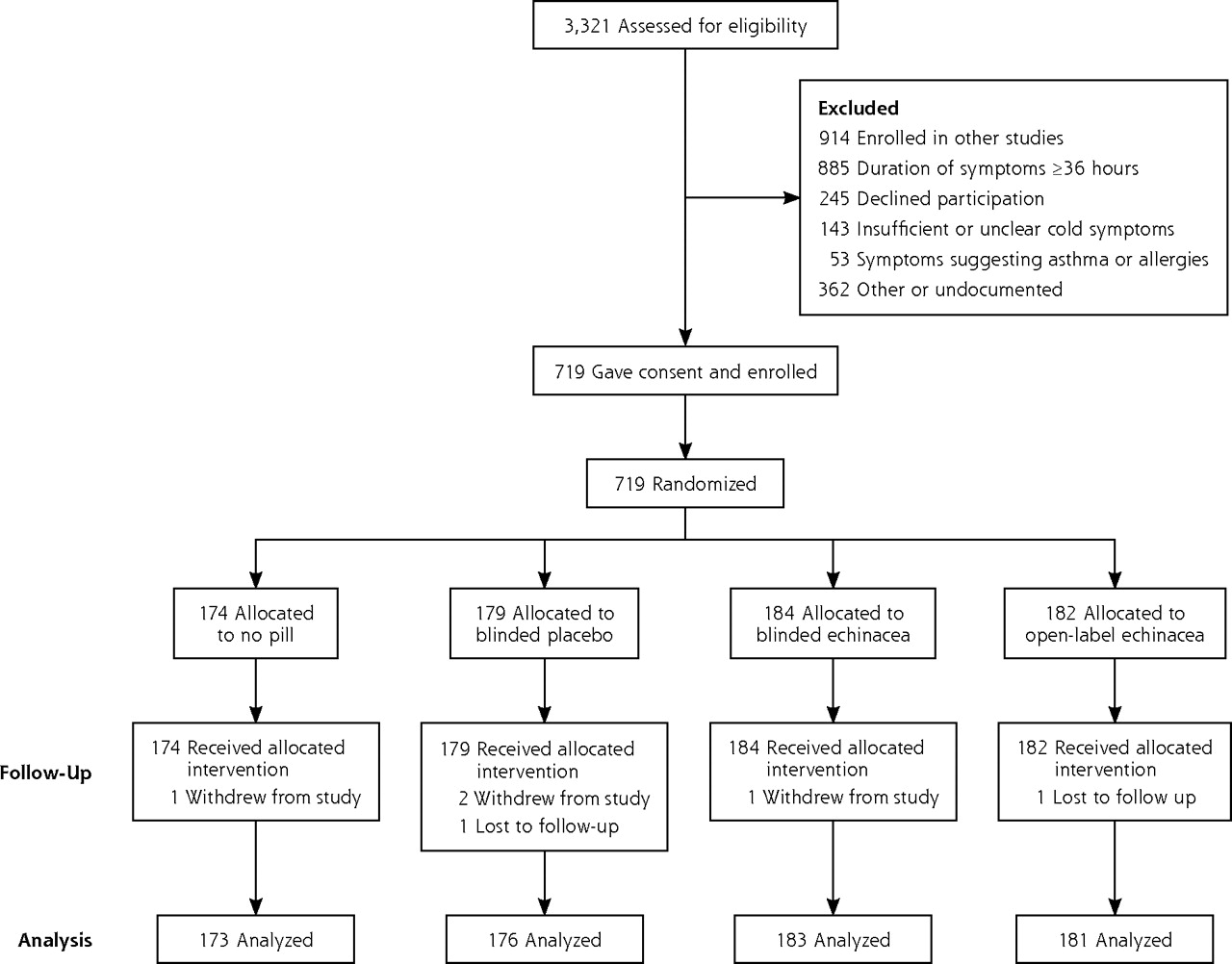
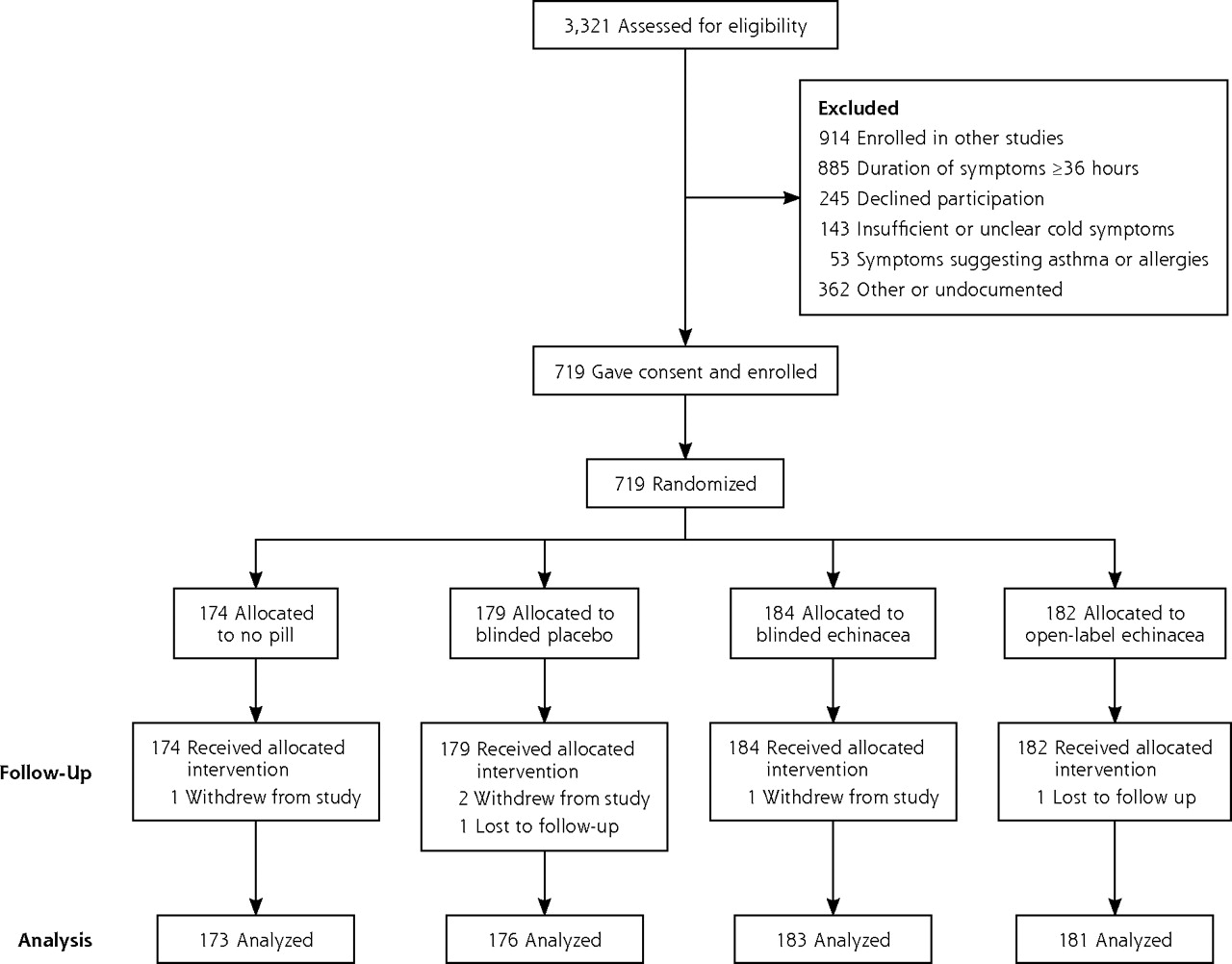
- Figure 1.
Participant flowchart: entry, randomization, and follow-up of participants
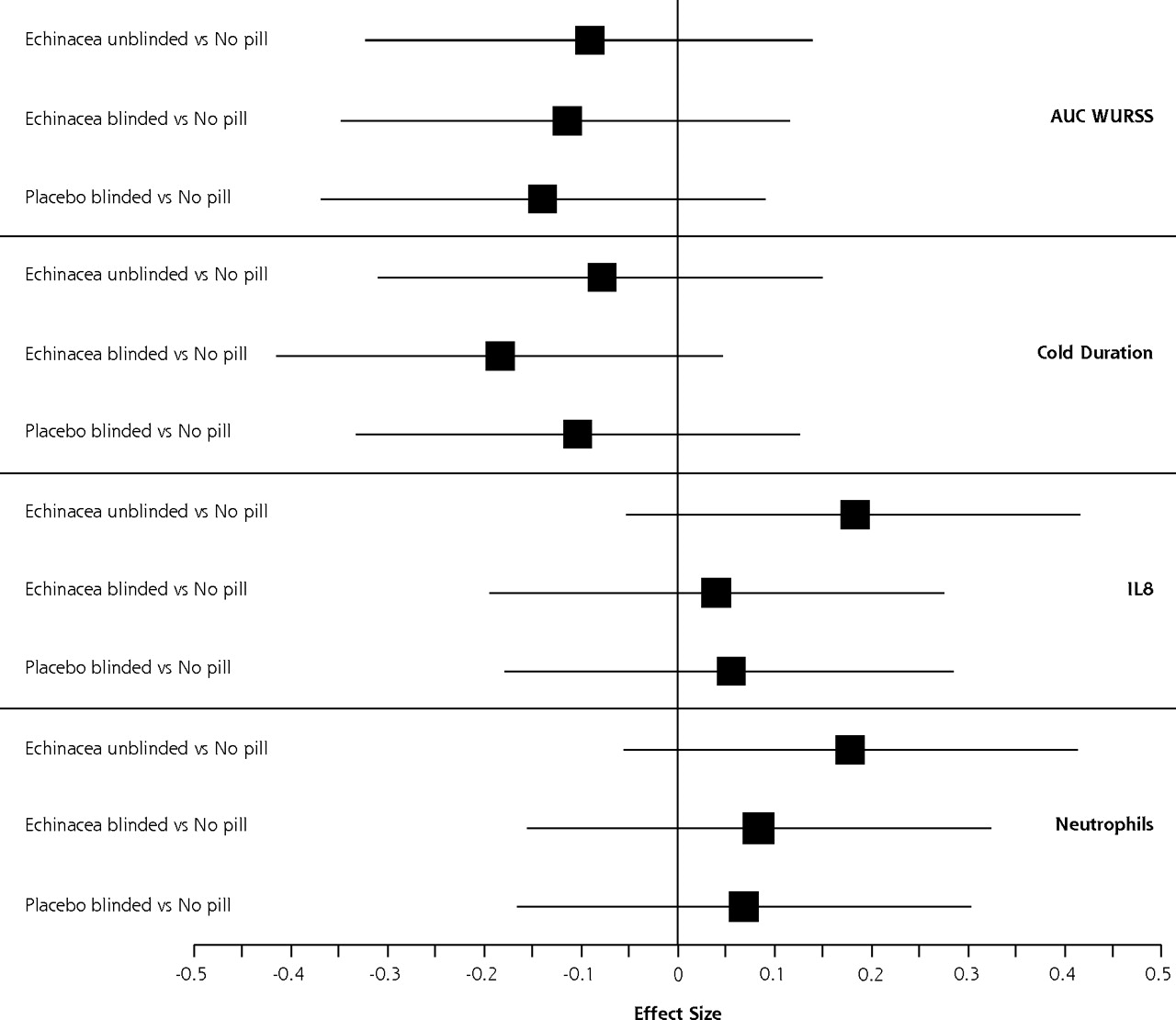
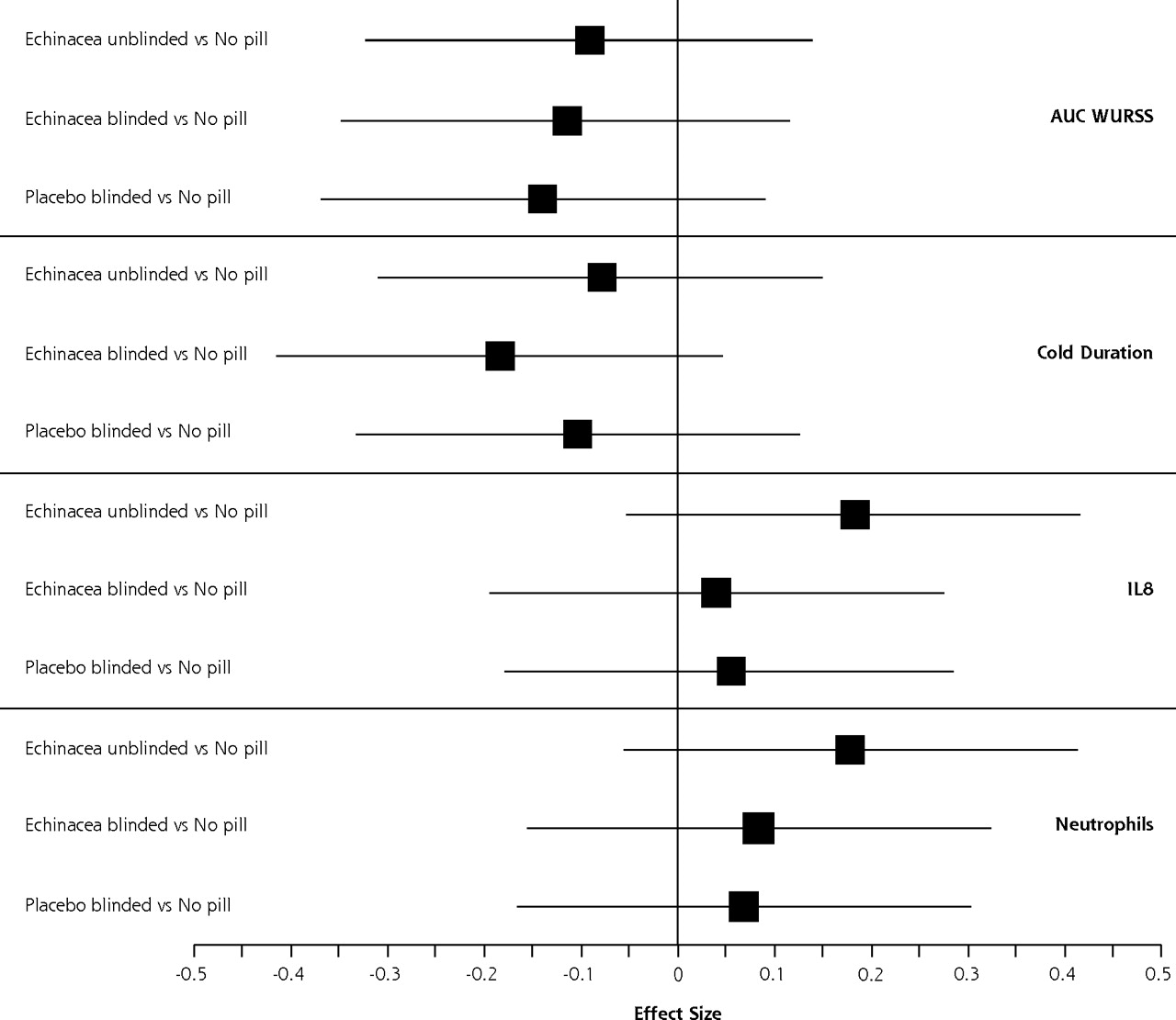
- Figure 2.
Standardized effect size of pill groups compared with no-pill group.
AUC = area-under-the-curve global severity; IL-8 = interleukin 8; WURSS = Wisconsin Upper Respiratory Symptom Survey.
Note: Central black boxes represent Cohen’s d standardized effect size; Error bars are 95% confidence intervals. These results come from a mixed general linear model adjusting for potential confounders: duration before entry, cold severity at entry, age, sex, ethnicity, education, income, smoking status, physical and mental health at entry, and assignment to the 3 clinician-related groups. Raw unadjusted results were similar.
Tables
Characteristic All n=719 No Pill n=174 Blinded to Placebo n=179 Blinded to Echinacea n=184 Open-Label Echinacea n=182 a Belief in echinacea (expectancy) was assessed at baseline using a visual analogue scale ranging from 0 (totally ineffective) to 100 (extremely effective); only those with some experience with echinacea answered this question. Age, mean (SD), y 33.7 (14.4) 32.3 (14.2) 33.2 (13.5) 35.4 (15.3) 33.9 (14.5) Age, interquartile range, y 21.5–41.8 20.8–43.4 21.3–43.5 21.5–46.5 21.7–46.5 Female, % 64.1 60.9 63.7 65.8 65.9 Nonwhite, % 12.1 13.8 12.3 14.1 8.2 Current smoker, % 12.8 14.4 11.2 14.1 11.6 Household income ≤$25,000, % 35.9 40.4 35.7 35.1 32.6 At least some college, % 84.0 84.0 85.6 80.0 86.4 Belief in echinacea score [No. of participants], mean (SD)a [219] 50.3 (20.6) [53] 50.7 (21.4) [48] 48.2 (21.5) [57] 50.7 (20.5) [61] 51.4 (19.4) Outcome No Pill Blinded to Placebo Between-Group Differences SF-8 = SF-8 Health Survey; WURSS-21 = 21-item Wisconsin Upper Respiratory Symptom Survey. a Global severity represents area-under-the-curve, with WURSS-21 scores the y-axis and illness duration the x-axis. b Because global severity was skewed, we first transformed using Box Cox methods, then adjusted for potential confounders with a mixed general linear model, controlling for symptom duration before entry, cold severity at entry, age, sex, ethnicity, education, income, smoking status, physical and mental health (SF-8), and randomized assignment to the 3 clinician-related groups. c Belief in echinacea (expectancy) was assessed by asking, “How effective do you think that echinacea is?” Participants responded by marking a visual analogue scale, which ranged from 0 (totally ineffective) to 100 (extremely effective). Sample size (protocol completers), n 173 76 – Illness duration, mean (95% CI), d 7.03 (6.51 to 7.56) 6.87 (6.33 to 7.41) −0.16 (−0.90 to 0.58) Illness duration, median (95% CI), d 6.42 (6.13 to 7.21) 6.47 (5.82 to 7.12) 0.05 (−0.78 to 0.88) Global severity score, mean (95% CI)a 286 (249 to 323) 264 (233 to 296) −22.0 (−70.3 to 26.3) Global severity score, median (95% CI)a 220 (189 to 238) 206 (177 to 256) −14.0 (−59.4 to 31.3) Transformed and adjusted global severity score (95% CI)b 10.3 (9.9 to 10.7) 10.0 (9.7 to 10.4) −0.30 (−0.76 to 0.46) Participants who rated echinacea’s effectiveness >50c Subsample size, n 32 25 – Illness duration, mean (95% CI), d 8.41 (7.09 to 9.72) 5.83 (4.44 to 7.23) −2.58 (−4.47 to −0.68) Illness duration, median (95% CI), d 7.95 (6.26 to 10.27) 4.45 (4.01 to 6.70) −3.50 (−5.80 to −1.20) Global severity score, mean (95% CI)a 374 (263 to 484) 277 (171 to 383) −97.0 (−249.8 to 55.8) Global severity score, median (95% CI)a 306 (178 to 430) 237 (115 to 330) −69.0 (−217.5 to 79.1) Transformed and adjusted global severity score (95% CI)b 11.3 (10.0 to 12.5) 10.2 (9.0 to 11.5) −1.10 (−2.81 to 0.61) Outcome Blinded to Echinacea Open-Label Echinacea Between-Group Differences SF-8 = SF-8 Health Survey; WURSS-21 = 21-item Wisconsin Upper Respiratory Symptom Survey. a Global severity represents area-under-the-curve, with WURSS-21 scores the y-axis and illness duration the x-axis. b Because global severity was skewed, we first transformed using Box Cox methods, then adjusted for potential confounders with a mixed general linear model, controlling for symptom duration before entry, cold severity at entry, age, sex, ethnicity, education, income, smoking status, physical and mental health (SF-8), and randomized assignment to the 3 clinician-related groups. c Belief in echinacea (expectancy) was assessed by asking, “How effective do you think that echinacea is?” Participants responded by marking a visual analogue scale, which ranged from 0 (totally ineffective) to 100 (extremely effective). Sample size (protocol completers), n 183 181 – Illness duration, mean (95% CI), d 6.34 (5.86 to 6.83) 6.76 (6.24 to 7.27) 0.42 (−0.28 to 1.12) Illness duration, median (95% CI), d 6.04 (5.30 to 6.53) 6.16 (5.31 to 6.60) 0.12 (−0.82 to 1.05) Global severity score, mean (95% CI)a 236 (210 to 263) 258 (226 to 289) 22.0 (−18.9 to 62.9) Global severity score, median (95% CI)a 193 (163 to 218) 195 (169 to 213) 2.00 (−34.0 to 37.5) Transformed and adjusted global severity score (95% CI)b 10.1 (9.7 to 10.4) 10.1 (9.7 to 10.5) 0.08 (−0.37 to 0.73) Participants who rated echinacea’s effectiveness >50c Subsample size, n 33 30 – Illness duration, mean (95% CI), d 7.10 (5.80 to 8.40) 7.07 (5.85 to 8.29) −0.03 (−1.78 to 1.72) Illness duration, median (95% CI), d 6.45 (4.32 to 8.40) 6.51 (5.50 to 8.92) 0.06 (−2.46 to 2.58) Global severity score, mean (95% CI)a 275 (179 to 370) 264 (198 to 330) −11.0 (−126.6 to 104.6) Global severity score, median (95% CI)a 202 (125 to 264) 243 (172 to 303) 41.0 (−50.2 to 130.6) Transformed and adjusted global severity score (95% CI)b 10.1 (9.1 to 11.2) 10.4 (9.5 to 11.3) 0.30 (−1.10 to 1.70) Outcome No Pill Blinded to Placebo Blinded to Echinacea Open-Label Echinacea IL-8 = interleukin 8; PSS-4 = Cohen’s Perceived Stress Scale-4; SF-8 = SF-8 Health Survey. a Data for IL-8 concentration and neutrophil count reflect median change in from baseline (day 1) to day 3. b Mean rank difference and geometric mean are shown for IL-8 concentration and neutrophil count because these measures were highly skewed and did not satisfy statistical assumptions of normality. c Mean values from day 3. d Side effects were assessed at exit by asking whether the participant had these at any time during the cold. e Comparing those reporting headache in the no-pill group with those in the other 3 groups combined yields χ2 of 22.3, which with 1 df is statistically significant at P <.001. Using χ2 to test dichotomous outcomes and the F test to test continuous outcomes, headache was the only between-group difference that reached P ≤.01. f Belief in echinacea (expectancy) was assessed by asking, “How effective do you think that echinacea is?” Participants responded by marking a visual analogue scale, which ranged from 0 (totally ineffective) to 100 (extremely effective). IL-8 concentration change, median, pg/mL (95% CI)a 30 (2–89) 39 (12–106) 58 (18–105) 70 (18–134) IL-8 concentration rank difference, mean, pg/mLb 322 333 330 358 IL-8 concentration geometric change, mean, pg/mL (95% CI)b 211 (140–316) 208 (141–308) 222 (159–311) 267 (181–393) Neutrophil count change, median, na 1.0 1.0 2.0 1.0 Neutrophil count difference, mean rank, nb 312 322 327 345 Neutrophil count, geometric change, mean (95% CI), nb 20.1 (15–29) 27.1 (19–40) 21.5 (15–31) 26.9 (18–40) SF-8 physical health score, n (95% CI)c 48.0 (47.1–49.0) 46.9 (45.9–48.0) 47.3 (46.2–48.4) 47.7 (46.8–48.6) SF-8 mental health score, mean (95% CI)c 43.8 (42.3–45.3) 42.5 (41.0–43.9) 44.4 (43.1–45.7) 43.7 (42.2–45.2) EuroQol Feeling Thermometer score, mean (95% CI)c 59.0 (56.0–61.9) 60.8 (57.5–64.0) 63.1 (60.3–65.9) 62.0 (59.2–64.8) PSS-4 stress score, mean (95% CI)c 11.7 (11.2–12.1) 11.4 (11.0–11.9) 11.5 (11.1–12.0) 11.5 (11.1–11.9) Side effects, % (95% CI)d Bad taste NA 9.1 (7.2–16.8) 12.4 (7.6–17.3) 8.9 (4.7–13.1) Diarrhea 5.4 (2.0–8.9) 12.0 (7.2–16.8) 9.6 (5.3–13.9) 9.4 (5.2–13.7) Headachee 62.1 (54.7–69.4) 49.1 (41.7–56.5) 46.3 (39.0–53.7) 47.8 (40.5–55.1) Nausea 10.2 (5.6–14.9) 12.6 (7.7–17.5) 15.8 (10.4–21.2) 6.7 (3.0–10.3) Rash 1.8 (0.0–3.8) 1.1 (0.0–2.7) 1.1 (0.0–2.7) 1.7 (0.0–3.5) Stomach upset 16.3 (10.7–21.9) 12.0 (7.2–16.8) 14.7 (9.5–19.9) 13.3 (8.4–18.3) Participants who rated echinacea’s effectiveness >50f Subsample size, n 32 25 33 30 IL-8 concentration change, median, pg/mL (95% CI)a 43 (17–57) 66 (47–81) 64 (27–72) 66 (36–93) IL-8 concentration geometric change, mean, pg/mL (95% CI)b 28 (18–43) 55 (41–75) 42 (29–62) 56 (45–70) Neutrophil count change, median, na 40 (20–59) 47 (26–76) 63 (33–73) 67 (39–87) Neutrophil count, geometric change, mean (95% CI), nb 28 (17–45) 38 (26–57) 48 (36–64) 56 (44–70)
The Article in Brief
Placebo Effects and the Common Cold: A Randomized Controlled Trial
Bruce Barrett , and colleagues
Background This study investigates how simulated real-life conditions (not taking a pill vs taking a named known pill) compares with the conditions of a conventional randomized controlled research trial. In particular, the study assesses 2 kinds of pill-related placebo effects in treating common cold (no pill vs blinded placebo and blinded vs open-label treatment), as well as potential effects of doctor-patient interaction.
What This Study Found There are modest and nuanced effects related to receiving pills regardless of their content, especially among those who believe in a particular therapy. The 4-armed trial (no pill, placebo, echinacea blinded and echinacea unblinded), which included 719 randomized participants aged 12 to 80 years, revealed that patients randomized to the no-pill group had longer and more severe illnesses than those who received pills, regardless of the pills� content. Among those who believed in the efficacy of echinacea and received pills, illnesses were shorter and less severe, regardless of whether the pills contained echinacea.
Implications
- Based on these findings, which suggest small but meaningful effects related to expectation and pill allocation, the authors conclude that patients� beliefs and feelings about treatments should be taken into consideration when making medical decisions.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Early intervention with a glycerol throat spray containing cold-adapted cod trypsin after self-diagnosis of the common cold: a randomised prospective, parallel group and single-blind methods trial (Glycerol-cod trypsin spray in common cold)
- Socioeconomic, racial and ethnic differences in patient experience of clinician empathy: Results of a systematic review and meta-analysis
- The Challenge of Reproducibility and Accuracy in Nutrition Research: Resources and Pitfalls
- In This Issue: Technology and Primary Care