Table of Contents
PLAIN-LANGUAGE SUMMARIES
Editorial
The Human Face of War: Family Doctors Enduring Conflict’s Daily Toll
Background: This issue of Annals of Family Medicine includes four articles discussing the impact of the Israeli/Palestinian conflict on family doctors and patients in the region. These articles offer perspectives from academic family doctors who have firsthand experience living and working in the region.
Editorial Stance: The decision to publish these articles was based on the idea that it is important to remember, support, and give voice to health care professionals and their patients who are living and working under horrifying conditions. Annals of Family Medicine hopes that these articles move beyond politics and taking sides to reveal the complexity and impact of this conflict.
Why It Matters: Family doctors in conflict zones face extraordinary challenges, providing care in an environment shaped by violence and uncertainty. These articles offer a glimpse into how war affects both patients and health care workers, showing that beyond political issues, real people—including clinicians trying to care for their communities and patients trying to manage their symptoms—are enduring the consequences.
The Human Face of War
Caroline R. Richardson, MD, Editor
Annals of Family Medicine
The Warren Alpert Medical School, Brown University, Providence, RI
_____________________________________________________________________________________
Research Brief
Study Reveals Impact of Trauma on Health Care Professionals Following the 2023 Terror Attack in Southern Israel
Background and Goal: The October 7, 2023, terrorist attack in southern Israel forced the evacuation of countless individuals, placing intense demands on health care personnel. Primary care clinicians, who are at the forefront of treating severely traumatized evacuees, are often exposed to secondary trauma, which can affect their mental health and job performance. This study investigated the levels of burnout, well-being, and resilience among health care staff working in primary care clinics in Israel during the aftermath of the attack. The goal was to better understand how trauma exposure impacts health care staff and to identify factors that might mitigate burnout.
Study Approach:This cross-sectional study was conducted from October 15th to November 20th, 2023. Electronic questionnaires were distributed to 600 medical professionals, including family physicians, nurses, medical secretaries, and social workers from urban and rural clinics serving both Jewish and Arab sectors. The questionnaire included demographic questions and two validated questionnaires measuring burnout and positive mental health.
Results:A total of 129 health care professionals completed the survey, 78% of whom were female. The average age was 49 years, most were family physicians (68%), Israeli-born (82%), secular (78%), and Jewish (90%).
-
The study results indicate that while health care professionals experienced a sense of significance and self-efficacy in treating evacuees, which positively contributed to their well-being, the prolonged daily exposure, spanning over a month, to traumatized patients led to increased levels of depersonalization among the professionals.
-
Health care professionals with more professional experience had better well-being scores and lower levels of mental exhaustion compared to those with less professional experience.
-
There was a negative correlation between age and depersonalization, meaning that older health care workers experienced lower levels of emotional detachment from their work.
-
Males reported higher levels of well-being than females.
Why It Matters:The well-being of health care personnel is critical to maintaining the quality of care provided to trauma survivors. These findings underscore the need for tailored interventions to mitigate psychological impact and address the risk of secondary traumatization among health care professionals.
The 2023 Terror Attack on Southern Israel: Well-Being and Burnout Among Health Care Personnel Treating Traumatized Evacuees
Dikla Agur Cohen, MD, MSc
Merav Sudarsky, MD
Department of Family Medicine, Ruth and Baruch Rappaport Faculty of Medicine, Technion - Israel Institute of Technology, Haifa, Israel
The Family Medicine Department, Clalit Health Services, Haifa and Western Galilee District, Israel
______________________________________________________________________
Essay
Caring for Families Under Occupation: The Struggles of Physicians Amidst War in the Palestinian Territories
Background: The ongoing military occupation of the West Bank and Gaza since 1967 has created a fragmented health care system in the Occupied Territories of Palestine, exacerbated by the current war in Gaza. Family physicians and other clinicians face numerous challenges, including the lack of coordination between health institutions, scarce resources, and limited access to specialized care. The October 7, 2023, war has worsened conditions, leading to more severe disruptions in health care and threats of violence posing new challenges for physicians working in these areas. In this essay, a family physician and her team in the southern West Bank describe their own challenges and give voice to the physicians in the Occupied Territories of Palestine they interviewed to better understand the professional and personal challenges of living and working during the uncertainty of war.
Key Argument: With the Gaza War, physicians in the West Bank are grappling with severe disruptions in access to health centers due to checkpoints and road closures, the constant risk of violence, and hospital raids that interrupt patient care. Witnessing the ongoing trauma to their patients and their own families carries a profound emotional toll. Despite these difficulties, physicians continue to find ways to support their patients and communities. They remain dedicated, even while facing burnout and emotional exhaustion, and many still seek ways to maintain communication and solidarity with their colleagues in Gaza.
Why It Matters: The personal accounts of physicians in the Occupied Territories of Palestine reveal the profound impact of occupation war and occupation on both clinicians and patients. Their stories illustrate the human cost of conflict and the immense difficulties in delivering even basic health care under such conditions. By sharing these experiences, the essay raises awareness of the need for international attention to the plight of medical professionals in the region, and the ongoing violations of medical ethics and human rights. It serves as a call to support these physicians as they continue to care for their communities despite overwhelming odds.
“We Haven’t Even Started Crying Yet:” Caring for the Family Under Occupation and War in the Occupied Palestinian Territories
Therese Zink, MD, MPH, et al
Family Medicine, Alpert School of Medicine, Brown University, Providence, Rhode Island
______________________________________________________________________
Essay
Healing In Conflict: The Perspective of an Israeli Family Physician During Wartime
Background:On October 7, 2023, Israel experienced a devastating attack when over 1,200 Israelis, including Jews, Christians, and Muslims, were killed or taken hostage by Hamas terrorists. Family doctors were suddenly responsible for treating patients amid ongoing rocket attacks and a heightened sense of insecurity, while entire communities faced displacement and psychological trauma. The author reflects on her experience volunteering at a temporary primary care clinic near the Dead Sea a week after the attack, providing care to displaced patients from diverse backgrounds.
Key Argument: This essay highlights the significant burden placed on family doctors during wartime. These physicians treated injured patients, provided trauma-informed care, and offered emotional support in a time of extreme fear and uncertainty. The sorrow the author encountered in her volunteering experience served as a reminder of the parallel suffering endured by civilians in Gaza.
Why It Matters: This essay sheds light on the complex realities physicians face when caring for patients in wartime, demonstrating how they continue to deliver compassionate care despite immense challenges. The experience of Israeli family doctors after the October 7th attack underscores the importance of trauma-informed care, empathetic communication, and mental health support. These physicians rapidly acquired new skills in trauma care and collaborated with mental health professionals to provide essential care, highlighting their resilience and commitment to supporting their communities during a crisis.
Healing Amidst Conflict: The Perspective of an Israeli Family Physician During Wartime
Dikla Agur Cohen, MD, MSc
Department of Family Medicine, Ruth and Baruch Rappaport Faculty of Medicine, Technion - Israel Institute of Technology, Haifa, Israel
The Family Medicine Department, Clalit Health Services, Haifa and Western Galilee District, Israel
_____________________________________________________________________________________
Special Report
Family Medicine in Times of War
Background and Goal:Wars and conflicts appear to be a fact of life for populations across the globe, often in places where family medicine functions as the backbone of the health care system. In these situations, family physicians are frequently called on to serve in expanded roles and are witnesses to the enormous mental and physical suffering of individuals, families, communities, and populations. This special report examines the role of family physicians in the Israel–Hamas conflict and other current wars, exploring how lessons learned from these situations can inform future practices in family medicine.
Key Insights:The report offers several important lessons for family physicians in wartime. Physicians must maintain open lines of communication with colleagues on all sides of the conflict and share timely, accurate information. Additionally, physicians are encouraged to hear and acknowledge the narratives of patients and other health care workers to foster understanding and reconciliation. The report also stresses the importance of providing both material and workforce support, such as donating medical supplies and volunteering to care for war casualties. Family physicians are urged to prepare for wartime service through expanded training in trauma care and mental health interventions. Lastly, the report advocates for family physicians to engage in research and social action, helping shape policies that improve health outcomes during and after conflicts.
Why It Matters: This report highlights the need for family physicians to be prepared to handle both the immediate and long-term effects of war, including physical injuries, psychological trauma, and the disruption of health care systems. By learning from current and past conflicts, the field of family medicine can better support patients and communities in future crises.
Family Medicine in Times of War
Jeffrey M. Borkan, MD, PhD
Department of Family Medicine, The Warren Alpert Medical School of Brown University, Providence, Rhode Island
_____________________________________________________________________________________
Original Research
Within-Group Physician Visits Reduce Emergency Department Use Compared to Out-of-Group Walk-In Clinic Visits
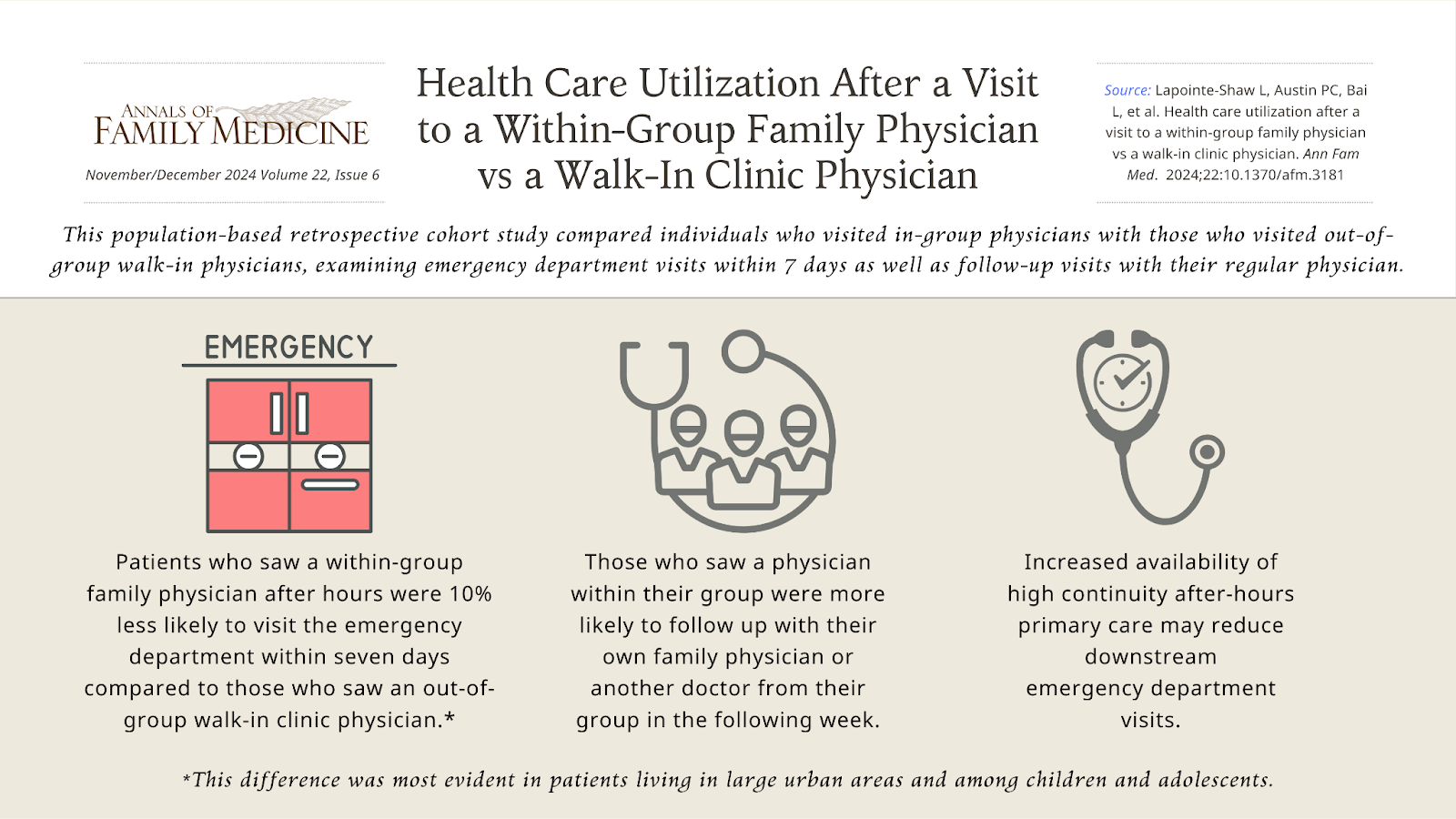
Background and Goal: Timely access to primary care is essential, but many patients face difficulties booking same-day or next-day appointments with their regular family physician. Walk-in clinics offer a solution by providing care without an appointment, but they often disrupt continuity of care. This study aimed to compare the outcomes of patients who visited a physician from their own family physician group during after-hours versus those who visited an out-of-group walk-in clinic physician.
Study Approach: This retrospective study used claims data from Ontario, Canada to compare patients who visited a physician within their family physician group for after-hours care with those who visited out-of-group walk-in clinics. Researchers examined emergency department visits within seven days of these appointments and other outcomes like follow-up visits with their regular physician. Patients in each group were matched to ensure comparable characteristics for analysis.
Main Results:The study identified 607,166 individuals who had their visit with a within-group physician during after-hours or on weekends, and 1,094,215 individuals who had their visit with an out-of-group walk-in clinic physician they were not enrolled to. After matching, there were 506,033 individuals in each group.
-
Patients who saw a within-group family physician after hours were 10% less likely to visit the emergency department within seven days compared to those who saw an out-of-group walk-in clinic physician.
-
This difference was most evident in patients living in large urban areas and among children and adolescents.
-
Those who saw a physician within their group were more likely to follow-up with their own family physician or another doctor from their group in the following week.
Why It Matters: The findings suggest that maintaining continuity of care, even for after-hours visits, can reduce unnecessary emergency department visits. Ensuring patients can access timely care with a physician within their own family physician group may help improve patient outcomes and reduce health care costs by decreasing emergency department usage.
Health Care Utilization After a Visit to a Within-Group Family Physician vs a Walk- In Clinic Physician
Lauren Lapointe-Shaw, MD, PhD, et al
Institute for Clinical Evaluative Sciences, Toronto, Ontario, Canada
Institute of Health Policy, Management and Evaluation, Department of Medicine, University of Toronto, Toronto, Ontario, Canada
Women's College Institute for Health System Solutions and Virtual Care, Women's College Hospital, Toronto, Ontario, Canada
Division of General Internal Medicine and Geriatrics, University Health Network and Sinai Health System, Toronto, Ontario, Canada
Visual Abstract:
____________________________________________________________________________________
Original Research
Antibiotic Initiation for Suspected Community-Acquired Pneumonia High Even When Chest X-Ray Results are Negative
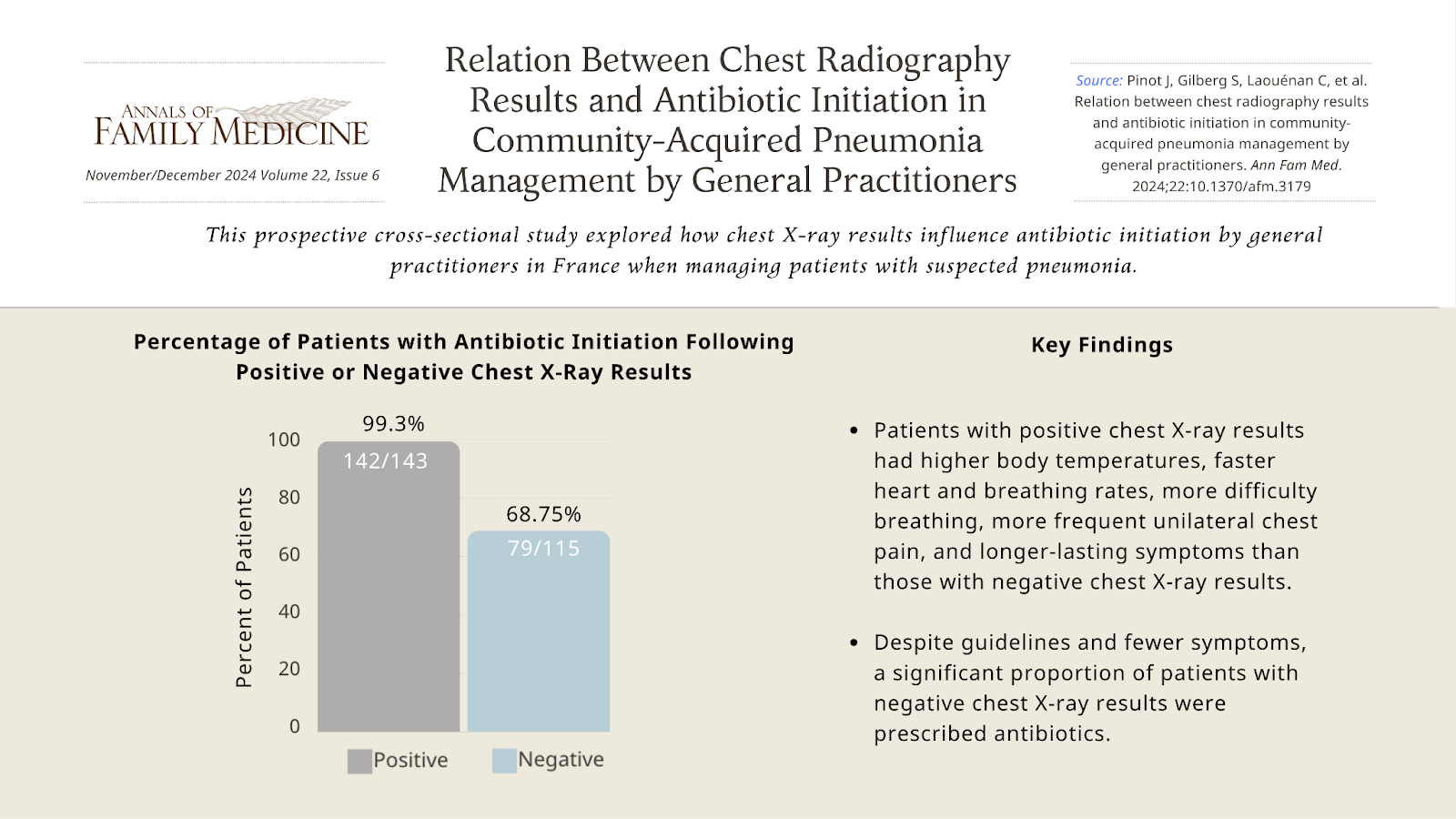
Background and Goal: Although clinical guidelines recommend using chest X-rays to confirm community-acquired pneumonia and limit unnecessary antibiotic use, there is ongoing debate about the role of chest X-rays in managing suspected pneumonia cases. This study explored how chest X-rays results influence antibiotic initiation by general practitioners in France when managing patients with suspected pneumonia.
Study Approach:A prospective cross-sectional study was conducted with adult patients with suspected pneumonia who received chest X-rays as part of their evaluation. To analyze factors associated with antibiotic initiation, patients’ characteristics were compared at inclusion and at 28 days between patients with positive chest X-rays (indicating pneumonia) and patients with negative chest X-rays.
Main Results:The sample included 259 adult patients. The median age was 58 years, 120 (46.3%) were male, 249 (96.1%) had not received antibiotics prior to inclusion, 69 (26.7%) had at least one risk factor for pneumococcal disease.
-
Most of the general practitioners who included patients were women (55.2 %; n = 153), with a median age of 39 years and 76.1% (n = 210) were general practitioner trainers.
-
55.6% of patients (144 out of 259) had positive chest X-rays results.
-
Patients with positive chest X-ray results had higher body temperature, faster heart rate, faster breathing rate, more difficulty breathing, and more frequent unilateral chest pain than patients with negative chest X-rays results and their symptoms lasted for a longer time.
-
99.3% of patients with positive chest X-ray results received antibiotics (142 out of 143 patients).
-
Despite fewer symptoms and negative chest X-ray results, a significant portion (68.75%) of patients with negative chest X-ray results were prescribed antibiotics (79/115 patients).
Why It Matters: The findings of this study show that many general practitioners prescribe antibiotics for suspected community-acquired pneumonia even when chest X-ray results are negative, highlighting a gap between guidelines and actual practice. This may contribute to the overuse of antibiotics, a major factor in antimicrobial resistance. The findings suggest that clearer guidelines and alternative diagnostic tools may be needed to help general practitioners confidently manage patients with suspected pneumonia without over-relying on antibiotics.
Relationship Between Chest Radiography Results and Antibiotic Initiation in Community-Acquired Pneumonia Management by General Practitioners
Juliette Pinot, MD, et al
Université Paris Cité and Université Sorbonne Paris Nord, INSERM, IAME, Paris, France
Université Paris Cité, Department of General Practice, Paris, France
Visual Abstract:
_____________________________________________________________________________________
Original Research
Restrictive Abortion Laws Drive Changes in Counseling, Increase Legal Concerns, and Weaken Training Confidence Among Family Medicine Professionals
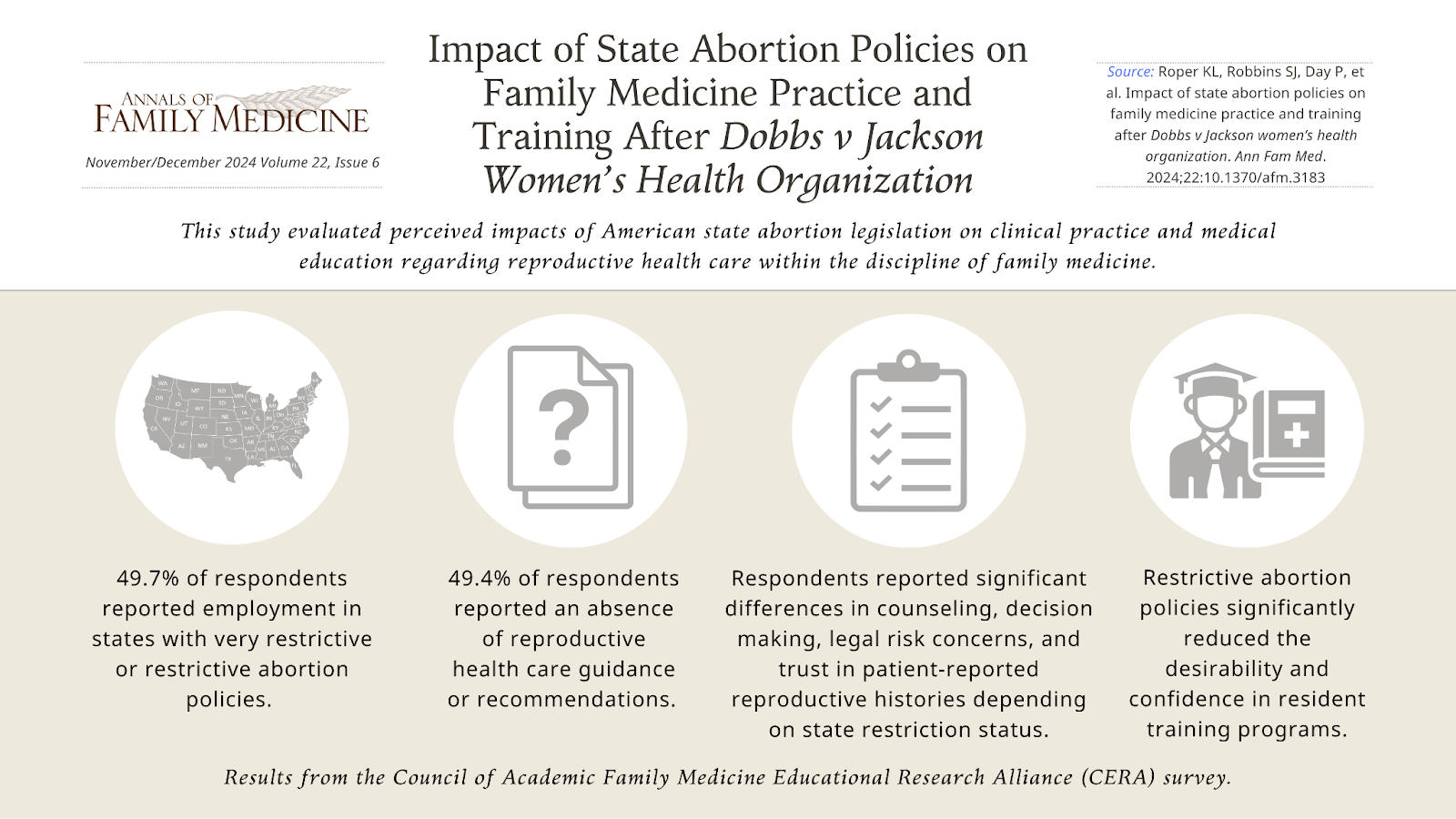
Background and Goal: The 2022 Supreme Court decision in Dobbs v. Jackson Women’s Health Organization removed federal protections for abortion, allowing individual states to establish their own laws. This shift has created significant legal uncertainty, especially in states with highly restrictive abortion laws. Family medicine clinicians, who often provide comprehensive reproductive care, are now navigating new challenges related to clinical practice and training. This study evaluated perceived impacts of state abortion legislation on clinical practice and medical education regarding reproductive health care within the discipline of family medicine.
Study Approach: The study utilized data from a national survey conducted by the Council of Academic Family Medicine, a joint initiative of four major academic family medicine organizations to support the leadership, research and education of the discipline. The survey gathered responses from family medicine clinicians, educators, and other professionals across states with varying abortion restrictions. States were classified based on their abortion policies according to the Guttmacher Institute, ranging from very restrictive to very protective. The survey measured changes in clinical practice, legal concerns, patient-clinician trust, and medical training since the Dobbs decision.
Main Results: Data from 1,196 respondents was analyzed.
-
Of the 1,196 respondents, 49.7% reported working in states with very restrictive or restrictive abortion policies.
-
Among the 991 respondents with clinical responsibilities, significant differences were observed in counseling practices, clinical decision-making, worry about legal risks, and trust in patients’ self-reported reproductive medical history compared to peers in unrestricted states.
-
Perceived trust from patients toward clinicians remained unchanged.
-
Respondents in states with restrictive abortion policies also reported significantly reduced confidence in resident training programs and a decrease in program desirability.
Why It Matters:The findings highlight that restrictive state abortion laws are already influencing how family medicine clinicians practice and how they train future health care professionals. Without clear guidelines, clinicians face legal uncertainties, which may affect their ability to provide comprehensive reproductive care. These challenges, particularly in states with restrictive abortion policies, could limit access to essential health care services and disrupt medical education.
Impact of State Abortion Policies on Family Medicine Practice and Training After Dobbs v Jackson Women’s Health Organization
Karen L.Roper, PhD, et al
Department of Family and Community Medicine, University of Kentucky, Lexington, Kentucky
Visual Abstract:
_____________________________________________________________________________________
Original Research
Collaborative, Trauma-Informed Care Improves Depression Outcomes in Primary Care
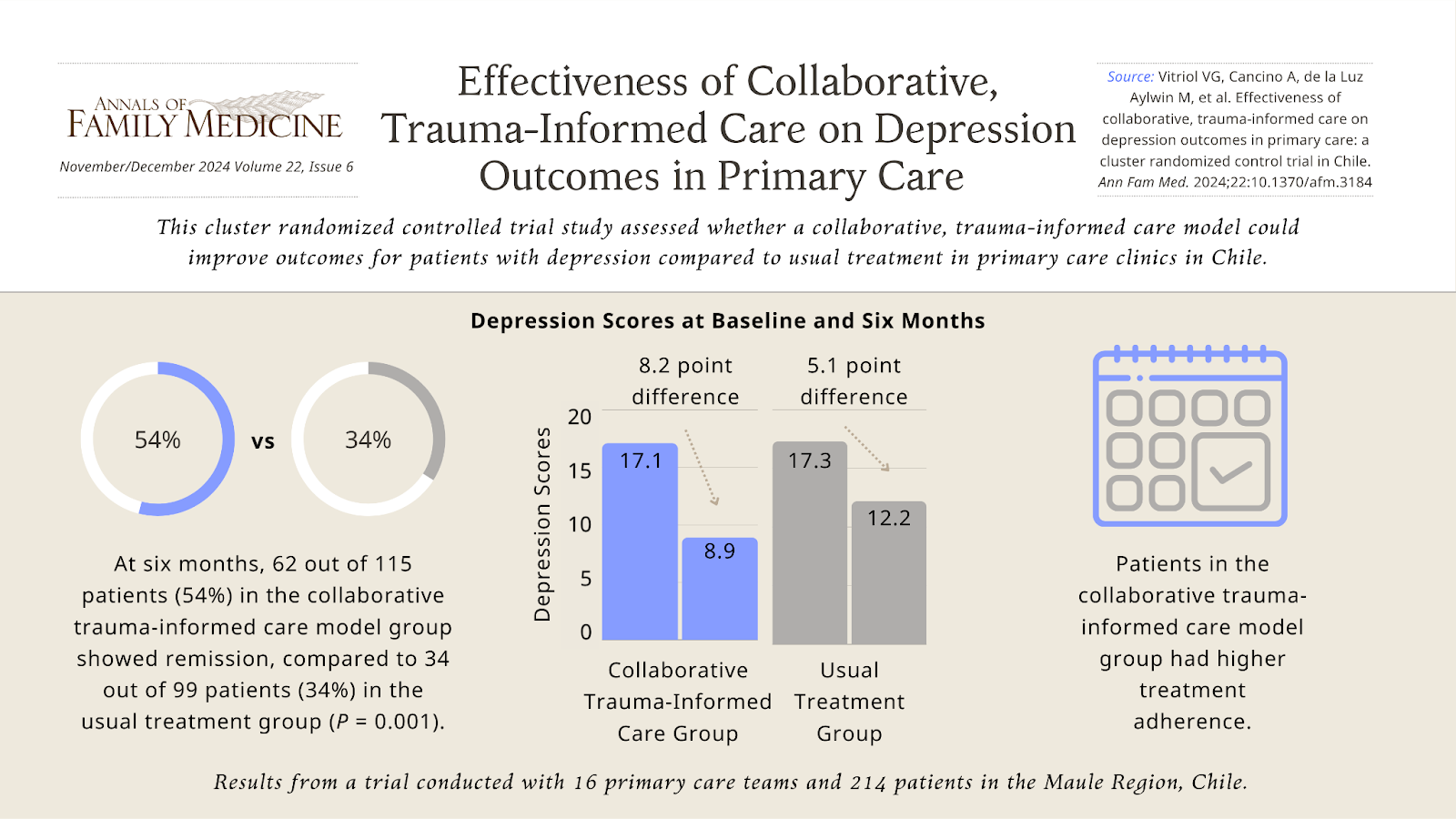
Background and Goal: Depression is a major public health issue in Chile, affecting women at twice the rate of men. During the COVID-19 pandemic, depressive symptoms rose sharply, stressing the need for more effective care in primary care settings. Many patients experience complex forms of depression that are linked to trauma and other challenges, which standard treatments often fail to address. This study aimed to assess whether a collaborative, trauma-informed care model could improve outcomes for patients with depression compared to usual treatment in primary care clinics in Chile.
Study Approach: The study was a cluster randomized controlled trial conducted with 16 primary care teams in the Maule Region, Chile, from August 2021 to June 2023. Clinics were randomly assigned to either the collaborative, trauma-informed care model or usual treatment model. Collaborative, trauma-informed care model teams consisted of a physician, a psychologist, and a social worker, all trained in trauma-informed care and in managing difficult-to-treat depression. Usual treatment teams, consisting of primary care professionals, followed current national guidelines for depression treatment.
A total of 214 adult patients between 18 and 70 years old with diagnosed depression were recruited and monitored over a six-month period, with evaluations at three and six months.
Main Results: 214 patients were recruited, 85% women, with 61.2% having 4 or more adverse childhood experiences.
-
Depression scores dropped significantly in both groups, but the collaborative trauma-informed care model group saw a greater reduction—from 17.1 to 8.9—compared to the usual treatment group, which improved from 17.3 to 12.2. (P < 0.001).
-
At six months, 62 out of 115 patients (54%) in the collaborative trauma-informed care model group showed remission, compared to 34 out of 99 patients (34%) in the usual treatment group. (p = 0.001)
-
Patients in the collaborative trauma-informed care model group had higher treatment adherence.
-
Both the collaborative trauma-informed care model and usual treatment groups showed improvements in anxiety, social functioning, and emotional regulation, but no significant differences were found between groups in these areas.
Why It Matters: This study demonstrates the effectiveness of integrating trauma-informed care into a collaborative care model for treating depression in primary care. By addressing complex forms of depression, particularly those complicated by past trauma, this approach showed significant improvements in patient outcomes. The findings suggest that this model can offer a more comprehensive and effective solution for treating difficult-to-manage depression.
Effectiveness of Collaborative, Trauma-Informed Care on Depression Outcomes in Primary Care: A Cluster Randomized Control Trial in Chile
Verónica G. Vitriol, MD, Mg, et al
University of Talca Medical School, Talca, Chile
Visual Abstract:
Original Research
Stay-at-Home Order Led to Increased Reporting of Health-Related Social Needs in Oregon
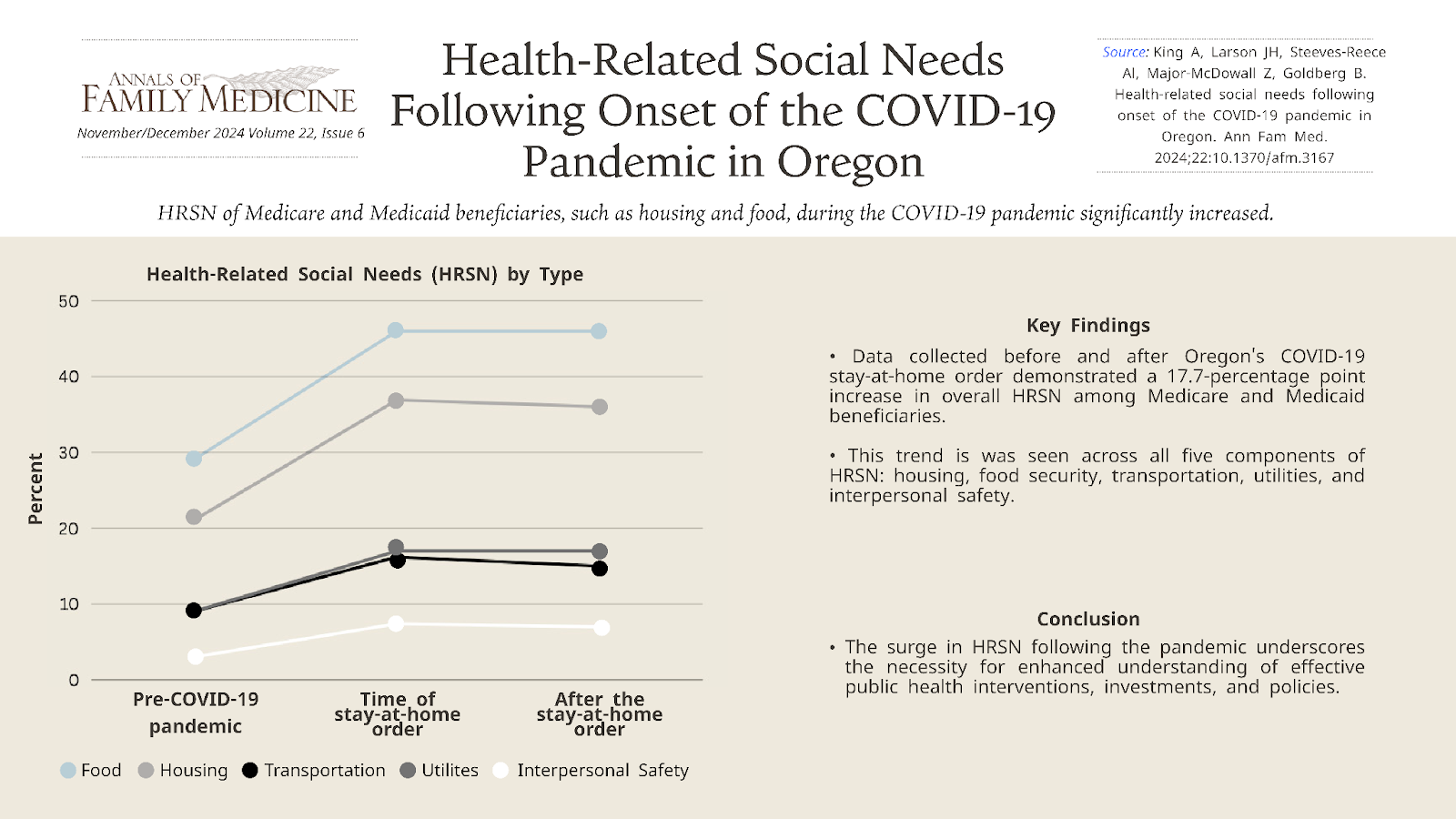
Background and Goal: Efforts to address the health-related social needs (HRSN) of Medicare and Medicaid beneficiaries, such as housing and food, during the COVID-19 pandemic were insufficient. This research examined HRSN data from the Accountable Health Communities (AHC) study collected in Oregon to understand changes in HRSN for Medicare and Medicaid beneficiaries at the onset and first two years of the pandemic.
Study Approach: The study sample included 21,522 Medicare and Medicaid beneficiaries screened for overall health-related social needs between May 13, 2019 and December 24, 2021. An interrupted time series analysis was used to analyze both the immediate effects and the long-term trend changes in Medicare and Medicaid beneficiary reported HRSN following Oregon’s stay-at-home order.
Main Results: A total of 21,522 unique Medicare and Medicaid beneficiaries participated in AHC in Oregon between May 13, 2019 and December 24, 2021: 8,234 before the March 23, 2020 stay-at-home order and 13,288 following it. The number of screens for any given week ranged from 34 to 385.
-
There was an abrupt 17.7 percentage point increase in overall health-related social needs around March 23, 2020 (onset of stay-at-home order) which did not significantly decline during the study period.
-
The percentage of beneficiaries reporting food, housing, and interpersonal safety needs increased by 16.5, 15.9, and 4.4 percentage points, respectively, with no significant decline during the study period.
-
The percentage of beneficiaries reporting transportation and utility needs increased by 7.5 and 7.2 percentage points, respectively, but decreased significantly after the start of the pandemic (decreasing by 0.2 and 0.1 percentage points each week, respectively).
Why It Matters: The jump in the number of people reporting health-related social needs following the start of the pandemic and the persistence of needs, particularly in housing, point to a need for increased understanding of which public health and health care interventions, investments, and policies effectively address health-related social needs. Public investments in social service delivery systems, and population-specific actions by payers and clinical systems may be effective strategies to address the health-related social needs of Medicare and Medicaid beneficiaries.
Health-Related Social Needs Following Onset of the COVID-19 Pandemic in Oregon
Anne King, MBA, et al
Oregon Rural Practice-based Research Network, Oregon Health & Science University, Portland, Oregon
Visual Abstract:
_____________________________________________________________________________________
Original Research
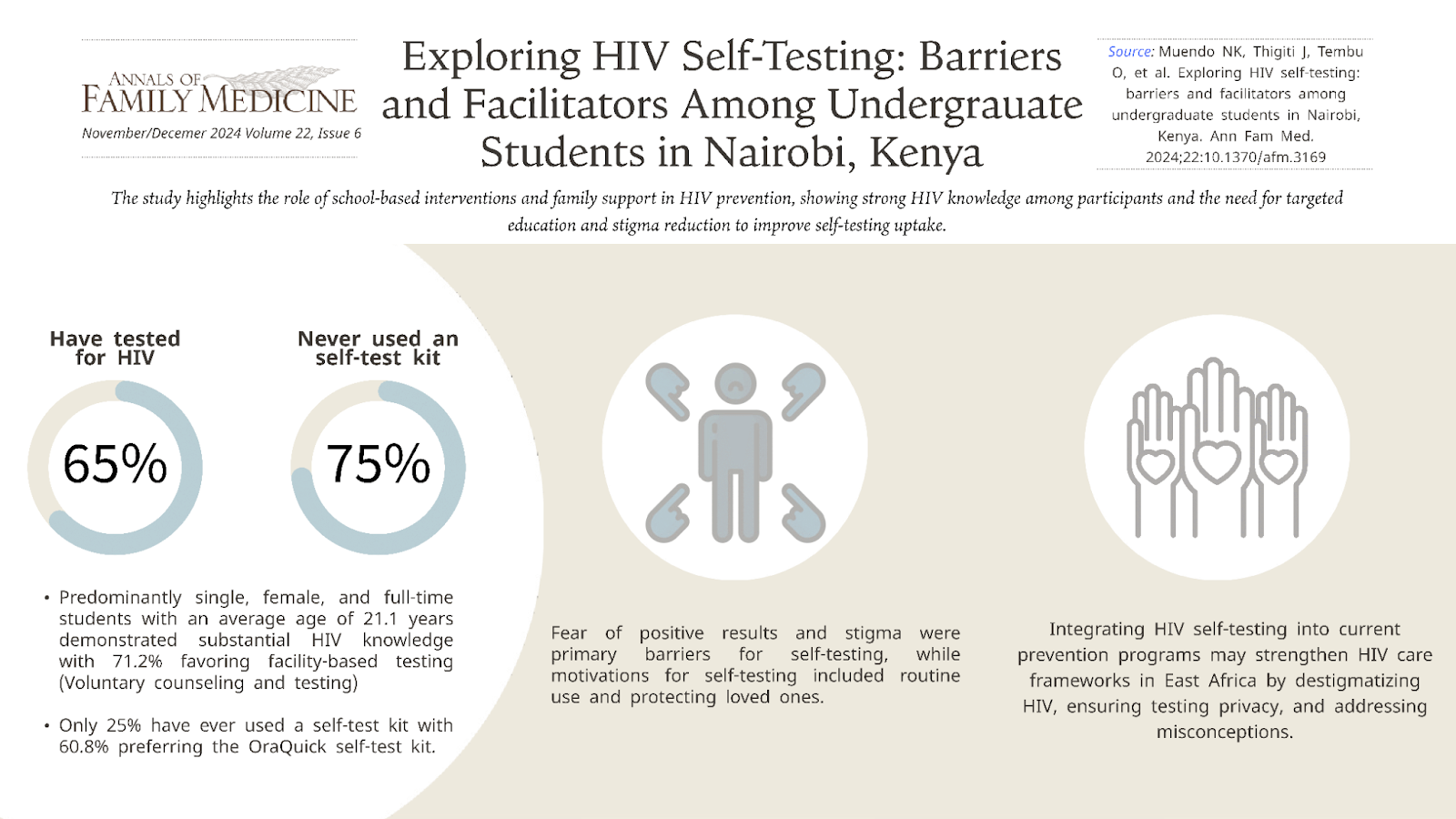
Fear of Positive Results and Stigma Hinder HIV Self-Testing, While Routine Use and Protecting Loved Ones Motivates University Students
Background and Goal: HIV remains a global health challenge, with over 36.9 million individuals living with HIV in 2017. Despite efforts to increase HIV testing and treatment, traditional services have not effectively reached marginalized communities. HIV self-testing (HIVST) offers a discreet and accessible alternative, potentially improving testing rates among at-risk populations, including university students in Kenya. This study assessed the awareness and acceptance of HIVST among undergraduate students.
Study Approach:This cross-sectional analytical study employed a multi-stage cluster sampling technique among undergraduate students aged 18-21 years at Kenyatta University. Clusters from various academic departments were randomly selected, and individual students were chosen for participation until the desired sample size of 398 participants was reached. Data were collected through questionnaires administered by trained enumerators.
Main Results:Participants’ age averaged 21.1 years, with a majority being single, female, and full-time students.
-
Substantial HIV knowledge was observed, and nearly half were aware of pre-exposure prophylaxis (47.7%).
-
The majority of students have tested for HIV (65.3%), with a majority not using a self-test kit (75.6%).
-
Only 24.4% of students used a self test kit.
-
45.4% of students said they would prefer to use a self-test kit rather than go to a facility.
-
Fear of positive results and stigma were primary barriers for self testing, while motivations for self-testing included routine use and protecting loved ones.
-
Media exposure, especially the "Chukua Selfie" campaign, correlated with higher HIVST usage.
Why It Matters: Participants' substantial knowledge of HIV contrasts with findings from other regions, underscoring the need for targeted education and safe sex promotion. Addressing fear and stigma through comprehensive interventions is essential for improving HIVST uptake. Integrating HIV self-testing into existing prevention programs can enhance HIV care frameworks in East Africa. Strategies to destigmatize HIV, ensure privacy in testing, and address misconceptions are vital for improving health outcomes among young individuals. Continuous efforts to strengthen self-testing programs are crucial to achieving global HIV targets.
Exploring HIV Self-Testing: Barriers and Facilitators Among Undergraduate Students in Nairobi, Kenya
Nicholas Kyalo Muendo, MBChB, MSc, MMed, et al
Department of Family Medicine, Kenyatta University, Nairobi, Kenya
Visual Abstract:
_____________________________________________________________________________________
Research Brief
Direct Primary Care Practices Less Likely Found in High-Need Shortage Areas but More Common in Rural Regions
Background and Goal:Direct primary care (DPC) is a model where patients pay a membership fee to a physician who provides your primary care, bypassing insurance. While this model has grown in popularity, there are concerns it might worsen the shortage of primary care doctors by focusing on areas that are already well-served. This study explored how often health professional shortage areas overlap with DPC practices across the U.S. DPC practices were also compared with a random group of primary care physicians in the U.S. to determine if there were significant differences between the two groups.
Study Approach: The researchers collected data on DPC practices from public sources and compared their locations to health professional shortage areas in the U.S. They also compared DPC practices to insurance based primary care physicians to see if there were differences in where they were located. Analyses were stratified by degree of rurality and health professional shortage area priority need scores.
Main Results: As of the date of download, there were 3,935 population-based health professional shortage areas in the US. 2,125 DPC practices were identified.
-
44% of Direct Primary Care (DPC) practices were located in health professional shortage areas, slightly lower than the 47% of insurance based primary care physicians in health professional shortage areas.
-
DPC practices were more often found in low- and medium-priority need areas within health professional shortage areas (45% in low-need, 47% in medium-need). In contrast, 20% of insurance based primary care physicians were in high priority need areas, compared to 14% of DPCs, showing that insurance based primary care physicians were slightly more concentrated in higher-need areas.
-
25% of DPCs in Health Professional Shortage Areas were located in rural areas, and 22% were in partially rural areas, while insurance based primary care physicians were more concentrated in non-rural areas (63% of insurance based primary care physicians versus 53% of DPCs).
Why It Matters: DPC practices are generally less likely to be located in health professional shortage areas compared to insurance-based primary care practices. However, they are more likely to be found in rural or partially rural health professional shortage areas. These findings suggest that, while DPCs do not currently serve the most underserved populations overall, their success in rural areas—traditionally a challenging environment for primary care—indicates that this model could be scalable in other underserved regions.
Are Direct Primary Care Practices Located in Health Professional Shortage Areas?
Neal D. Goldstein, PhD, MBI, et al
Department of Epidemiology & Biostatistics, Drexel University Dornsife School of Public Health, Philadelphia, Pennsylvania
_________________________________________________________________________________
Methodology
Adapted Nominal Group Technique Effectively Builds Timely Consensus on Health Care Priorities for Older Adults
Background and Goal:The participatory research approach is an important tool of family medicine and primary health care research, but standard consensus methods like the Delphi and nominal group techniques can be time-consuming and may not represent a broad range of opinions. To address these issues, researchers developed an adapted nominal group technique (aNGT) to efficiently build consensus among stakeholders with diverse perspectives.
Approach: This study focused on shaping care trajectories for adults aged 65 and older, aiming to prioritize key domains and identify new care indicators. Researchers used four main strategies: (1) recruiting four diverse stakeholder groups (older adults, clinicians, managers, and decision makers) through purposeful and snowball sampling; (2) using remote tools to maximize participation; (3) adding a pre-elicitation activity so participants could individually review study materials and rank domains before group discussions; and (4) tailoring discussions to each group’s needs by, for example, scheduling meetings around lunch for clinicians and avoiding jargon.
Main Results:Of 28 participants who completed the questionnaire, 20 joined a group discussion. Through the pre-elicitation activity and one round of discussions, participants reached a consensus on prioritizing “symptoms, functioning, and quality of care.” Tailored discussions and remote tools were the most effective strategies in the process.
Why It Matters: By addressing traditional consensus-building challenges, the aNGT fosters inclusivity, efficiency, and relevance, making it a valuable approach for research that informs care standards. This study provides a practical model for inclusive research design, showing how to streamline consensus-building while ensuring that stakeholder voices drive meaningful health care outcomes.
Building Timely Consensus Among Diverse Stakeholders: An Adapted Nominal Group Technique
Deniz Cetin-Sahin, MD, PhD, et al
Lady Davis Institute for Medical Research at the Jewish General Hospital, Montreal, Quebec, Canada
Department of Family Medicine, McGill University, Montreal, Quebec, Canada
_____________________________________________________________________________________
Special Report
Reforming Primary Care to Combat the Diabetes Epidemic
Background and Goal:Diabetes is a growing public health issue in the U.S., affecting 38.4 million people and placing a significant burden on primary care services. As the number of diabetes cases continues to rise, primary care professionals play a key role in managing this complex, chronic condition. This report explores strategies to improve diabetes care.
Key Insights: The report highlights several important areas for improvement. First, there is a shortage of primary care professionals. Expanding the roles of nurse practitioners, pharmacists, and other health care professionals can help address this gap. Team-based care models, such as the Chronic Care Model and Patient-Centered Medical Home, have been effective in improving diabetes care by promoting better coordination among health care professionals. However, current payment structures do not sufficiently reimburse non-physician health care professionals, limiting the success of these models. Reforming payment systems to support all care team members and emphasizing preventive care is necessary. Lastly, diabetes disproportionately affects underserved populations, particularly racial and ethnic minorities. Improving access to primary care in these communities is essential for addressing health disparities.
Why It Matters: Diabetes affects millions of Americans, and as the number of cases grows, it is important that primary care physicians are equipped to manage this complex condition effectively. This report highlights the need for national policy changes to support primary care teams, including workforce expansion, team-based care approaches, and payment reform.
Diabetes Management: A Case Study to Drive National Policy Change in Primary Care Settings
Lisa Murdock, et al
American Diabetes Association, Arlington, Virginia
____________________________________________________________________________________
Special Report
Improving Early Detection of Cognitive Impairment in Primary Care
Background and Goal:The number of people living with Alzheimer’s disease in the U.S. is expected to double to nearly 14 million in 2060. Early detection of cognitive impairment is essential for improving patient outcomes, but primary care settings face significant challenges in screening. Presented at an interdisciplinary Geriatrics Summit hosted by the National Academy of Neuropsychology, this special report summarizes key points and gaps in knowledge about methods for detecting cognitive impairment in primary care clinics.
Key Insights: The report highlights the importance of addressing the rising incidence of cognitive impairment as the population ages, particularly with new treatments for early Alzheimer’s disease now available. It advocates for creative solutions to manage the increased workload, such as partnering with community health workers and leveraging telehealth. Automated tools for risk stratification, cognitive screening, and follow-up are in development, with successful models already integrated into electronic health records. Clinical trials are needed to assess multi-step protocols that combine risk assessment with cognitive screening in primary care and community settings. The report emphasizes the importance of developing cognitive care plans, especially for vulnerable populations, and outlines the need for clear roles between primary care physicians and specialists in managing cognitive disorders.
Why It Matters:Addressing cognitive decline early on can lead to better patient outcomes and improved quality of life. By removing barriers to screening and promoting collaboration between primary care and specialists, more patients can be identified earlier and receive the care they need.
Improving Early Detection of Cognitive Impairment in Older Adults in Primary Care Clinics: Recommendations From an Interdisciplinary Geriatrics Summit
Robin C. Hilsabeck, PhD, et al
National Academy of Neuropsychology, Denver, Colorado
The University of Texas at Austin Dell Medical School, Austin, Texas
_____________________________________________________________________________________
Theory
Unhurried Conversations: An Urgent Must-Have For Patient-Centered Care
Background and Theory Overview: The theory behind “unhurried conversations” in health care emphasizes the importance of slowing down medical interactions to enable patient care. The approach identifies behaviors that patients and clinicians could enact within the context of the health care system in which they meet to “deepen” the interaction so that participants can work together to advance the patient’s situation. The idea challenges the increasingly fast-paced nature of modern health care, which often prioritizes efficiency at the expense of care.
What is New: This article identifies and elaborates on ten observable and key micro-level patient-clinician communication practices that support unhurried conversations. It outlines specific strategies for clinicians and patients to adopt. The article also provides guidance on how health systems can enable unhurried conversations by adjusting workflows and rethinking productivity metrics to prioritize patient-centered care.
Why It Matters: In a health care system that often rushes through patient interactions, this theory offers a pathway to more thoughtful, compassionate care. By adopting unhurried conversations, clinicians can improve the quality of the care they give and of their relationships with patients in achieving care that fits. This shift should improve the ability of clinicians and patients to address each patient situation, foster patients’ feelings of being heard and understood, and allow them to work together with clinicians in forming care plans that make sense. Additionally, it supports clinicians in being better able to care well for and with their patients.
Unhurried Conversations in Health Care Are More Important Than Ever: Identifying Key Communication Practices for Careful and Kind Care
Victor M. Montori, MD, et al
Knowledge & Evaluation Research Unit, Mayo Clinic, Rochester, Minnesota
_____________________________________________________________________________________
Innovations in Primary Care
New Process Decreases Wait Time for Diagnosis and Treatment for ADHD and Other Psychiatric Conditions
In a suburban family medicine residency clinic, an innovative approach was implemented to reduce wait times for adult ADHD diagnosis and treatment, which previously ranged from 20 to 56 weeks in behavioral health clinics. The new process involved two clinical visits. In the first visit, patients completed self-administered screening tools for ADHD and potential co-occurring conditions like depression, anxiety, and substance abuse. If ADHD was suspected, patients reviewed a diagnostic interview tool (DIVA-5) at home and returned for a second visit. During the second visit, clinicians reviewed the DIVA-5 results, confirmed the ADHD diagnosis if applicable, and offered treatment, including medication initiation. During the pilot phase, 80% of the 48 patients were diagnosed with ADHD, with 72% opting for medication. The new process decreased wait times for diagnosis and treatment by 46-96% compared to behavioral health referrals, significantly improving care access and patient satisfaction. This approach also increased the clinic’s ability to manage complex psychiatric conditions, offering a low-cost and adaptable solution for family medicine practices.
Adult ADHD Diagnosis in Family Medicine Clinic
Deborah M. Mullen, PhD, et al
The University of Tennessee at Chattanooga, Chattanooga, Tennessee
_____________________________________________________________________________________
Essay
Learning from Ervin’s Care: Ethics, Health Care Finance, and Human Connection
Background: The essay focuses on the care of a 70-year-old patient, Ervin, with complex medical conditions and intellectual disabilities. He was cared for in a Program of All-Inclusive Care for the Elderly (PACE) setting. The essay discusses the challenges of providing ethical medical and supportive care to individuals like Ervin, who often face complicated health and social issues.
Key Argument: Ervin’s story reveals significant challenges in the U.S. health care system, including gaps in social safety nets and ethical questions around caring for patients with reduced decision-making capacity. Many patients fall through the cracks due to the limitations of fee-for-service models and inadequate social services. Programs like PACE address some of these gaps through more personalized, team-based care. Ultimately, caring for this patient taught the author about the rewards of the human connections that primary care physicians establish with their patients.
Why It Matters: This essay highlights the need for health care systems to better support patients with complex medical and social needs. It underscores the importance of integrating medical care with social support to improve outcomes and build stronger connections between patients and their care teams.
Learning From Ervin’s Care: Ethics, Health Care Finance, and Human Connection
Amy C. Denham, MD, MPH
University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, North Carolina
_____________________________________________________________________________________
Innovations in Primary Care
Single-Visit First-Trimester Care with Point-of-Care Ultrasound Cuts Emergency Visits by 81% for Non-Miscarrying Patients
The Bethesda Family Medicine Clinic in St. Paul, Minnesota, established a bi-monthly Early Pregnancy Dating & Risk Assessment Clinic in September 2022. The clinic introduced an integrated approach, combining point-of-care ultrasound with immediate, multidisciplinary first-trimester care—a shift from the previous practice where each element, including ultrasound, risk assessment, and patient education, was conducted separately. During a single visit, patients under 14 weeks receive ultrasound-based dating, immediate assessment of pregnancy viability, and risk evaluation, with on-site counseling based on real-time ultrasound results. This integration allowed the clinic to quickly identify high-risk cases and offer timely intervention for issues such as miscarriage or abnormal pregnancies, reducing emergency visits, urgent clinic appointments, and first-trimester phone inquiries by 81% for non-miscarrying patients. For miscarriage cases, the time from initial concern to diagnosis decreased from an average of 5.8 days to 1.7 days. Clinic implementation led to more timely diagnosis of abnormal pregnancies and improved education and support for all patients, including those who experience miscarriage.
Enhancing First Trimester Obstetrical Care: The Addition of Point-of-Care Ultrasound
Allison Newman, MD, et al
Woodwinds Hospital Family Medicine Residency Program, Department of Family Medicine and Community Health, University of Minnesota Medical School, St. Paul, Minnesota