
Abstract
PURPOSE We wanted to systematically review whether primary care-based interventions improve initiation and duration of breastfeeding.
METHODS Studies were found by searching MEDLINE (1966–2001), HealthSTAR, the Cochrane Database of Systematic Reviews, the National Health Service Centre for Reviews and Dissemination Databases, and bibliographies of identified trials and review articles. Studies were included if they originated in the primary care setting and were conducted in a developed country, written in English, and contained a concurrent control group.
RESULTS Thirty randomized and nonrandomized controlled trials and 5 systematic reviews of breastfeeding counseling were included. Educational programs had the greatest effect of any single intervention on both initiation (difference 0.23; 95% confidence interval [CI], 0.12–0.34) and short-term duration (difference 0.39; 95% CI, 0.27–0.50). Support programs conducted by telephone, in person, or both increased short-term (difference 0.11; 95% CI, 0.03–0.19) and long-term duration (difference 0.08; 95% CI, 0.02–0.16). In contrast, written materials such as pamphlets did not significantly increase breastfeeding. Data were insufficient to determine whether the combination of education with support was more effective than education alone.
CONCLUSIONS Educational programs were the most effective single intervention. One woman would breast-feed for up to 3 months for every 3 to 5 women attending breastfeeding educational programs. Future research and policy should focus on translating these findings into more widespread practice in diverse primary care settings.
INTRODUCTION
Breast milk provides the optimal nutrition for infants and offers health benefits as well as immunity from infections.1 Maternal benefits of breastfeeding can include more rapid return of postpartum uterine tone and postpartum weight loss, delay of ovulation (temporary contraception), and decreased risk of breast, ovarian, and endometrial cancers.2,3 For these reasons, the Department of Health and Human Services’ Healthy People 2010 initiative has set a goal of having 75% of mothers breast-feed immediately postpartum, 50% at 6 months, and 25% at 1 year.4 Current breastfeeding rates fall short of these goals, and rates are lowest among vulnerable groups. “Vulnerable” refers to low-income, low educational level, and black populations. For example, US data from 2001 showed that 58% of low-income mothers and 53% of black mothers initiate breastfeeding. By 6 months, only 21% of low-income and 22% of black mothers continued breastfeeding. These rates compare with overall rates of 69.5% of new mothers who initiated breastfeeding, and 32.5% who were still breastfeeding at 6 months.5
Many public health and professional organizations emphasize the importance of breastfeeding.6–,12 Although initiatives exist for health care facilities to provide an environment that facilitates breastfeeding,13,14 guidelines for primary care-based interventions originating from a clinician’s office or hospital practice to improve breastfeeding do not currently exist. In 1999, the US Preventive Services Task Force (USPSTF) decided to develop new, evidence-based recommendations on primary care-based interventions to support breastfeeding. To assist the USPSTF, the Oregon Health & Science University Evidence-based Practice Center (OHSU-EPC) conducted a systematic review to evaluate the effectiveness of counseling, behavioral, and environmental interventions to improve breastfeeding. This review examined either the initiation or duration of breastfeeding in developed countries, or both the initiation and duration of breastfeeding if information was available.
METHODS
Study Selection
Randomized controlled trials (RCTs) and cohort studies conducted in developed countries were included in our review. We sought studies involving any counseling or behavioral intervention originating from a clinician’s practice (office or hospital) that was implemented to improve breastfeeding initiation, duration, or both. Interventions could be conducted by a variety of providers (including physicians, nurses, lactation consultants, or peer counselors) and in a variety of settings (clinic, hospital, home, or elsewhere) as long as they originated from the health care setting. Using this definition, community-based or peer-originated interventions were not included. For interventions that had not been studied in RCTs, we included nonrandomized controlled trials, but we did not include any other nonrandomized controlled trials in this review.
Search Strategy
We searched MEDLINE, the Cochrane Controlled Trials Registry, and HealthSTAR for articles from 1966 to December 2001, using the MeSH terms and keywords “breastfeeding,” “counseling,” “health education,” “teaching materials,” “medical advice,” and “advice” or “advise.” We also searched the Cochrane Database of Systematic Reviews (CDSR) and the National Health Service Centre for Reviews and Dissemination databases using the terms “lactation” and “breastfeeding.”
Two reviewers independently reviewed all abstracts and titles for inclusion. Studies were included if they originated in the primary care setting, were conducted in a developed country, were written in English, and contained a concurrent control group.
Data Extraction
Two reviewers independently abstracted the following descriptive data from all included studies: population and setting; type of control; type, frequency, timing, intensity, and duration of the intervention; person delivering the intervention (ie, nurse, lactation consultant, physician, peer counselor); and definitions for breastfeeding outcomes, including exclusivity, initiation, and duration of breastfeeding, adherence, and follow-up. We categorized interventions as group or one-on-one education, in-person or telephone support (including peer counseling), written materials, rooming-in, early contact, and commercial discharge packets. We defined education as individual instruction sessions or group classes that contained structured content, including anatomy, physiology, and nutritional issues. These sessions often included practical skills training, such as positioning, latch-on techniques, pump equipment use, and questions and answers to address common fears, problems, and myths. We categorized interventions as support when they provided telephone or in-person (clinic, hospital, or home) social support, advice, or encouragement. Supportive interventions were often personalized to individual patient needs. Early maternal contact is defined as a period of time, typically 10 to 45 minutes, of skin-to-skin contact between mother and infant soon after birth. breastfeeding outcomes were categorized as initiation, short-term duration, and long-term duration according to timeframes com monly reported in the literature. breastfeeding initiation referred to breastfeeding before hospital discharge, short-term duration referred to 2 to 4 months postpartum, and long-term referred to 4 to 6 months postpartum. Disagreements between the 2 reviewers were resolved by consensus. A third reviewer independently verified the accuracy of the data within the evidence tables.
Quality Assessment Instrument
We assessed the quality of published systematic reviews and controlled trials using criteria developed by the USPSTF.15 Two reviewers independently reviewed each study and applied the task force criteria and assigned each paper a quality rating of “good,” “fair,” or “poor” (Appendix B of the accompanying article, “Behavioral Interventions to Promote Breastfeeding: Recommendations and Rationale”). The criteria for systematic reviews include the use of explicit selection criteria and systematic appraisal of study quality, publication date, and relevance of the review. Individual studies were rated as poor if they used poor randomization techniques or if they failed to maintain comparable groups and failed to consider or adjust for potential confounders. There was 100% agreement between reviewers in quality scoring of systematic reviews and 93% agreement in quality scoring of individual studies. When the reviewers disagreed, a final score was reached though consensus.
Data Synthesis
We conducted separate meta-analyses of RCTs to examine the influence of specific components of counseling interventions on rates of 3 outcome measures: (1) initiation of breastfeeding (Y1); (2) breastfeeding for 1 to 3 months (short-term duration) (Y2); and (3) breastfeeding for 4 to 6 months (long-term duration) (Y3). We included trials that offered educational interventions, interventions using in-person or telephone support, or both. One RCT of support in very low-birth-weight infants was excluded from the meta-analysis.16 Mean differences and 95% confidence intervals were calculated for the individual and combined effects of education and support. Within these categories we examined the effect of using written materials as a cointervention.
Random effects meta-regression models were fit on the data from the eligible RCTs. For each dependent variable Yi, we fit the following regression equation:

where πi represents the ith probability of outcome (initiation, short-term duration, or long-term duration) and Ci is the control group rate for the ith study (an adjustment for baseline differences in breastfeeding rates among studies). To estimate the effect of the combination of education plus support on each outcome πi, we separately pooled studies that combined these interventions. Similarly, we estimated the effect of education combined with written materials by separately pooling studies that used both. To compare the effects of education or support alone to education with support or written materials, we compared these pooled estimates with the estimates of the effects of education alone and support alone derived from our model. The Bayesian data analytic framework was used to fit the models. Inference on the parameters was done using posterior probability distributions. The data were analyzed using WinBUGS software,17 which uses a method of Markov Chain Monte Carlo called Gibbs Sampling to simulate posterior proba bility distributions. Noninformative prior probability distributions were used. Sensitivity analyses were performed excluding poor-quality studies and to assess the effect of breastfeeding rates in the control group. There was no significant difference in the results when poor studies were excluded. We then fit a second model using all studies to allow for a linear association between the control group rate and the effect of the intervention.18 Data from the second model are presented.
RESULTS
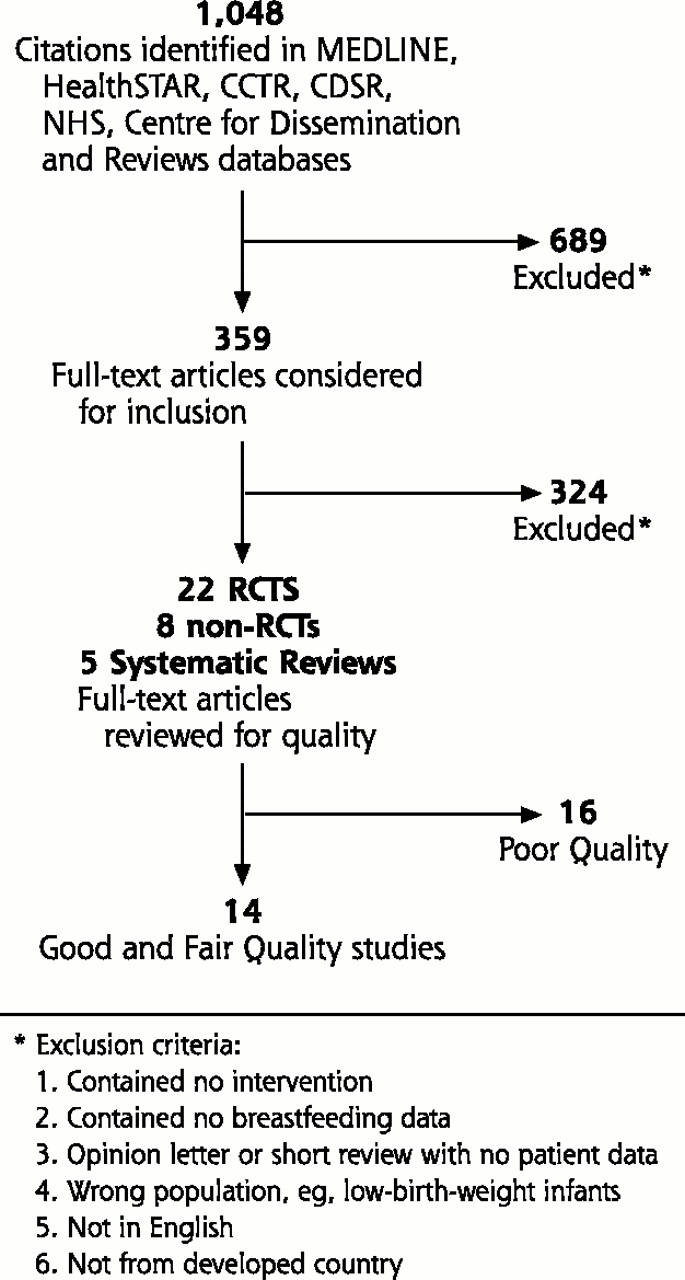
The searches selected 1,048 abstracts, of which 689 were rejected following abstract review. Full-text articles were reviewed to identify 22 RCTs,19–,40 8 non-RCTs,41–,48 and 5 systematic reviews49–,53 of breastfeeding counseling (Figure 1⇓).54
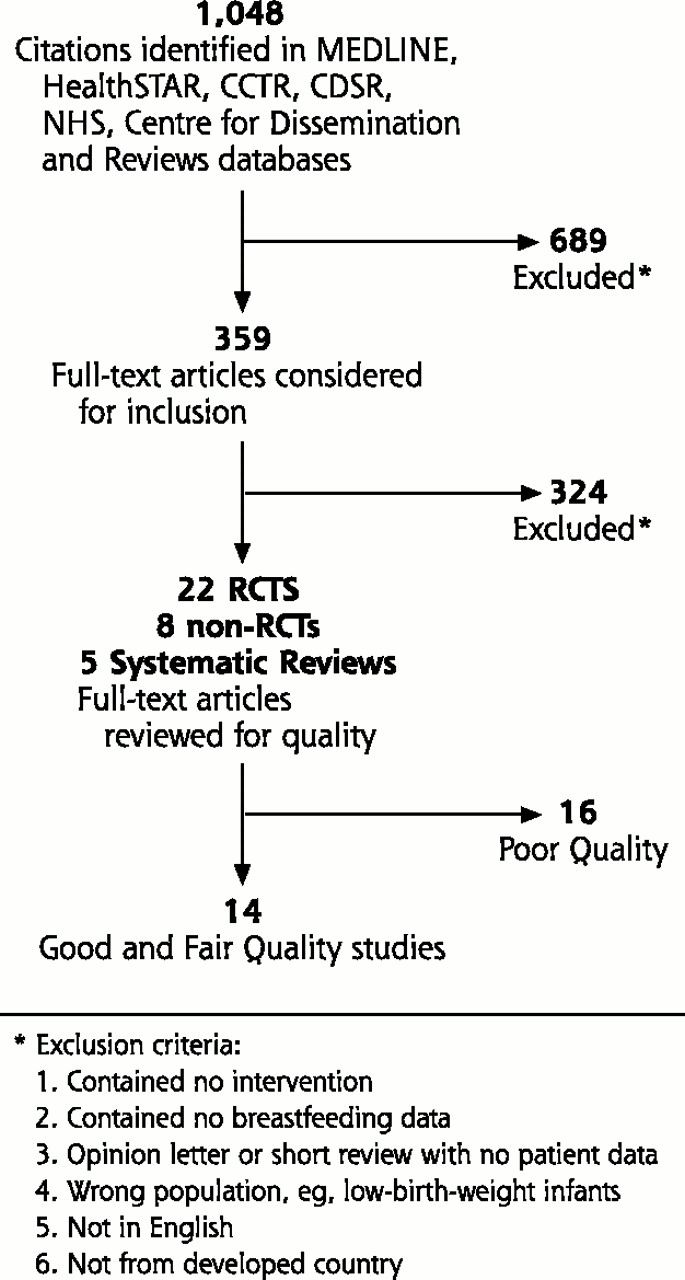
Study Eligibility Flow Chart
Trial Characteristics
A table of descriptive information (available as a data supplement in the online full-text version of this article at: www.annfammed.org/cgi/content/full/1/2/70/DC1) displays the types of interventions evaluated in the trials: group or one-on-one education, in-person or telephone support, written materials, rooming-in, early contact, and commercial discharge packets. Using the USPSTF criteria, 12 studies were judged to be of fair quality,19–25,27–29,40,41 2 were of good quality,30,38 and 16 studies were of poor quality.26,31–37,39,42–,48 Most of the poor-quality trials had substantial baseline differences between control and intervention groups, lack of adjustment for confounders, high attrition, or insufficient data to conduct intention-to-treat analyses.
Table 1⇓ summarizes the results of the RCTs of education, support, and written materials compared with usual care. In general, breastfeeding interventions improved rates of initiation and continuation of breastfeeding. Effects on long-term duration were small. Interventions appear to have larger effects in populations with low baseline rates of breastfeeding.
Breastfeeding Interventions
Breastfeeding Education.
Twelve RCTs studied the impact of individual or group education inter ventions on breastfeeding initiation or duration (Table 1⇑).19–23,26,29–31,35,45 The key features of the educational sessions are displayed in the descriptive information data supplement at: www.annfammed.org/content/full/1/2/DC1. These programs were usually conducted by lactation specialists or nurses as antepartum sessions. Structured content that was consistently delivered on core topics: breast milk as the ideal nutrition for infants, benefits of breastfeeding (health and other), physiology, and anatomy. Additional educational sessions frequently provided skills training, such as breastfeeding positioning and latch-on techniques, equipment (including clothing, pumps, and storage), and questions and answers addressing common fears, problems, and myths. Most educational sessions lasted 30 to 90 minutes, and there was not an apparent association between length of session and effectiveness. Similarly, whether the education sessions were individual or in groups did not appear to predict success. As shown in Table 1⇑, there appears to be greater effectiveness of educational sessions in populations where the preintervention breastfeeding rate is less than 50%.
Table 2⇓ displays the results of the meta-analysis. Overall, programs that had these educational components increased breastfeeding initiation (difference 0.23; 95% confidence interval [CI], 0.12–0.34) and short-term continuation up to 3 months (difference 0.39; 95% CI, 0.27–0.50). Education did not have a significant impact on long-term duration up to 6 months (difference 0.04; 95% CI, −0.06–0.16).
Results of Meta-analyses of Studies of Education and Support
Breastfeeding Support.
Eight RCTs21,23–27,37 studied the impact of in-person or telephone support on breastfeeding initiation and duration (Table 2⇑). Support programs involved telephone or in-person clinic, hospital, or home visits by lactation consultants, nurse or peer counselors,26 and combined prearranged appointments and unscheduled visits or telephone calls for problems. The content of the intervention was often personalized to the individual patient’s needs. Timing of support programs was divided, with 3 exclusively antepartum,24–,26 3 exclusively postpartum,21,27,37 and 2 both antepartum and postpartum.27,29
Overall, support alone significantly increased short- and long-term breastfeeding duration, with differences of 0.11 (95% CI, 0.03–0.19) and 0.08 (95% CI, 0.02–0.16), respectively, but did not have a significant effect on initiation (difference 0.06; 95% CI, −0.02–0.15) (Table 2⇑).
We were interested not only in the isolated effect of support but also in the added benefit of supportive measures when combined with educational programs. Four RCTs combined breastfeeding support with educational programs.21,23,26,29 All 4 of these studies used in-person contact through either clinics or home visits. Compared with support alone, studies that combined breastfeeding education and support produced larger increases in initiation (from difference of 0.06; 95% CI, −0.02–0.15 to difference 0.21; 95% CI, 0.07–0.35), short-term duration (from difference 0.11; 95% CI, 0.30–0.19 to difference 0.37; 95% CI, 0.17–0.58), and no difference in long-term duration. The combination of education and support, however, was not substantially different from that of education alone.
Support and Peer Counseling.
Peer counselors are thought to be particularly useful sources of support and motivation. One RCT26 and 4 non-RCTs evaluated peer counselors.44,46–,48All were judged to be of poor quality because of assembly of dissimilar groups, important loss-to-follow-up, or lack of adjustment for important confounders. Often studies assigned patients to the control group when there was no peer counselor available to see them or if they did not request a counselor at all. One of these studies44 compared 4 separate clinics each with a different intervention regime: (1) peer counselor only, (2) video education only, (3) peer plus video, and (4) control with no intervention. Although the clinics had similar demographics in general, there were statistically significant baseline differences in parity, education, and employment among patients enrolled in the different clinics. Each of these factors could have affected the breastfeeding rates. Another study46 compared 2 clinics that had peer counselors with 6 clinics that did not. Before the intervention, the breastfeeding rate of the intervention group was lower than that of the control group (22.5% vs 27.5%).
All 4 of the nonrandomized trials measured breastfeeding initiation. Although there was a trend toward benefit in all, only 1 study47 found a significant benefit for breastfeeding initiation and 2 studies46,47 found a significant benefit for short-term breastfeeding. The first study consisted of women who were planning or had experienced a delivery at Cook County Hospital in Chicago.47 The intervention group consisted of women who intended to breast-feed, requested a peer counselor while they were pregnant or postpartum, and had a peer counselor that was available for consultation. Priority was given to primiparous patients who requested peer counselor services. The control group similarly consisted of women who intended to breast-feed, requested a peer counselor either in pregnancy or after delivery, and did not have a peer counselor available. The groups were statistically similar in education, race, work plan (ie, plan to return to work or school), previous breastfeeding, and perceived support. Five patients were lost to follow-up in each group. In this study, 55 of 59 (93%) women in the intervention group initiated breastfeeding compared with 30 of 43 (70%) women in the control group, and the mean number of weeks of breastfeeding was similarly higher in the intervention group (15 weeks in the intervention group vs 8 weeks in the control group).
Written Materials.
Seven RCTs22,27,29–32,35 examined the effect of written materials, either alone or in combination with other interventions, on breastfeeding initiation and duration. Written materials varied in their length and detail, from a list of key points, to pamphlets reinforcing educational materials, to more detailed booklets. Three30–,32 of the RCTs studied the effect of written materials alone, and 4 RCTs22,27,29,35 combined written materials with education or support or both (Table 1⇑). Written materials alone did not increase breastfeeding rates. The pooled estimate for the effectiveness of written materials plus education was comparable to that of education alone estimated from the full model. The combination of education plus written materials, in 3 studies measuring short-term duration of breastfeeding, appeared less effective (0.10; 95% CI, −0.01–0.21) than education alone (risk difference from logit model 0.39; 95% CI, 0.27–0.50).
Rooming-In.
Only 1 study55 conducted in a developed country included rooming-in as an intervention. This study contained multiple other interventions, thus the effect of rooming-in alone could not be ascertained.
Early Maternal Contact.
Early maternal contact is defined as a period of time, typically 10 to 45 minutes, of skin-to-skin contact between mother and infant soon after birth. One good-quality Cochrane review examined the effect of early maternal contact.51 We conducted a meta-analysis of the 4 studies56–,59 of early maternal contact that were conducted in developed countries and found no significant benefit (odds ratio [OR], 1.23; 95% CI, 0.65–2.05).
Commercial Discharge Packets.
One good-quality Cochrane review of 9 randomized trials found that giving mothers commercial discharge packs often containing samples and coupons for formula reduced exclusive breastfeeding.53 Only 2 studies looked at the effect of commercial packs containing formula samples on any breastfeeding in 0 to 2 weeks. One study of 88 women rated 4 out of 5 by Cochrane for quality found no significant difference in breastfeeding at 1 week in women who were given commercial discharge packets with formula at discharge from the hospital (12 of 38 in the intervention group vs 10 of 50 in the control group).60 One more recent larger trial of poor quality39 found that 12 of 163 (7%) women in the commercial group ceased breastfeeding before discharge vs 2 of 148 (1%) in the control group (P = 0.03). Women with uncertain goals for breastfeeding were significantly less likely to breast-feed and to breast-feed exclusively if given commercial packs.
One trial found no increase in short-term breastfeeding for an intervention targeted at pacifier avoidance.40 One trial38 compared an intensive program for usual care consisting of group sessions, one-on-one clinic visits, and free access to breastfeeding consultation with a less intense intervention consisting of a home health visit by a registered nurse 48 hours after discharge from the hospital. They found no difference in rates of initiation or continuation of breastfeeding.
DISCUSSION
In summary, education and support interventions to promote breastfeeding appear to improve breastfeeding initiation and maintenance up to 6 months. Educational sessions that review the benefits of breastfeeding, principles of lactation, myths, common problems, solutions, and skills training appear to have the greatest single effect. One woman would successfully initiate and maintain breastfeeding for up to 3 months for every 3 to 5 women that attended educational sessions. breastfeeding classes are offered by many practices. One challenge for translating these findings into clinical practice will be to make breastfeeding classes more accessible to all patients.
Although peer counselor programs are used by many practices and hospitals, there are insufficient data to determine their effectiveness. Other common office or hospital practices include provision of written materials and discharge packets. Neither practice was found to be effective in prompting breastfeeding; in fact, discharge packets were found to have a detrimental effect.
In previous good-quality systematic reviews,51,52 education and peer counseling increased breastfeeding initiation and support measures increased duration. Written materials were not effective in increasing initiation or duration. The use of discharge packs containing promotional material with or without formula samples significantly reduced exclusive breastfeeding for up to 6 weeks. Unlike the previous reviews, which included trials from developing countries, our analysis is the first to assess all breastfeeding interventions singly and in combination in developed countries.
breastfeeding intervention studies often combined interventions. None of the individual studies, however, compared the combined intervention against each component separately. We used a meta-regression to estimate the effects of education and support alone and conducted a separate meta-analysis of studies that combined these interventions. Our analysis suggests that, for initiation and short-term duration of breastfeeding, the combination of education plus support might be more effective than support alone, but not more effective than education alone. The addition of written materials to education did not increase (and might have decreased) the effectiveness of education. These results offer a compelling rationale for future intervention studies that compare combined education and support with education and support alone.
This review provides encouraging evidence that educational programs and support services provided in research settings can improve breastfeeding initiation and duration rates in the United States and other developed countries. It is as yet unknown, however, how widely accessible such programs are in this country and how effective and cost-effective they are in real-life, diverse health care settings. If not all mothers are receiving breastfeeding education or support services, studies might be needed of what barriers exist at the levels of the patients and health care systems, and whether these barriers can be surmounted.
This review found that overall studies of breastfeeding interventions lacked scientific rigor, a finding that has been echoed by numerous systematic reviews. Intervention studies often lacked detail to assess similarity among similar interventions. For example, educational interventions were mixed on their detailed description of content of the session, method of communicating the content, training of the individual to deliver the content, and total time spent in the educational session. Across studies, it is difficult to assess the variability of routine care, which was the most common control group. In certain communities it might be standard to receive 1 home visitation and in others it might not.
This review found that studies rated as poor quality by the quality-rating system developed by the US Preventive Services Task Force had results similar to those rated as good or fair. Many of these studies were nonrandomized controlled trials that were rated as poor because there were baseline differences in the compared groups, or randomized trials with issues regarding randomization methods or lack of intention-to-treat analyses. Although such flaws have been shown to be correlated with effect sizes in studies of obstetric interventions,61 their impact in studies of clinic-based behavioral counseling is uncertain. Because of this uncertainty and the lack of statistical difference with and without poor-quality studies, all studies were pooled to display mean differences and confidence boundaries. The lack of scientific rigor in individual studies to date is also a limitation for the strength of these findings. These data, however, reflect the summary of the best evidence available to date. Additional research on the generalizability of the standard quality criteria to behavioral counseling interventions is needed. At the same time, future studies of breastfeeding interventions should make every attempt to follow high-quality standards of randomization, analysis, and reporting.
Recommendations and Rationale
The US Preventive Services Task Force Behavioral Interventions to Promote Breastfeeding: Recommendations and Rationale are available at the supplementary data link from the online full-text version of this article at http://www.annfammed.org/cgi/content/full/1/2/70/DC2.
SUPPORT
This study was conducted by the Oregon Health & Science University Evidence-based Practice Center under contract to the Agency for Healthcare Research and Quality, contract #290-97-0018, Task Order Number 2, Rockville, Md. Additional support came from the National Institutes of Health grant NIH-K12 HD01243-01 and the Agency for Healthcare Research and Quality grant 1 K08 HS11338-01. The authors of this article are responsible for its contents, including clinical or treatment recommendations. No statement in this article should be construed as an official position of the Agency for Healthcare Research and Quality or the US Department of Health and Human Services.
REPRINTS
Reprints are available from the AHRQ Web site (www.preventiveservices.ahrq.gov) and through the National Guideline Clearinghouse (www.guideline.gov). Print copies of this article, along with other articles and Recommendation and Rationale statements, are available by subscription to the Guide to Clinical Preventive Services, Third Edition: Periodic Updates. The cost of this subscription is $60 and is available from the AHRQ Clearinghouse (call 1-800-358-9295 or e-mail ahrqpubs{at}ahrq.gov).
Reprints of the USPSTF recommendations based on this evidence review can be found in Counseling to Promote Breastfeeding: Recommendations and Rationale, available on the AHRQ Web site and in the Guide to Clinical Preventive Services, Third Edition: Periodic Updates.
Acknowledgments
We are thankful to Susan Carson, MPH, and Marian McDonaugh, PharmD, for their assistance in reviewing articles, and Patty Davies, MS, for her assistance in conducting the literature searches.
Footnotes
-
Conflicts of interest: none reported
- Received for publication February 20, 2003.
- Accepted for publication June 11, 2003.
- © 2003 Annals of Family Medicine, Inc.
REFERENCES
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Factors influencing the early initiation of breast feeding in public primary healthcare facilities in Northeast Nigeria: a mixed-method study
- Use of Telehealth to Increase Breastfeeding Exclusivity and Duration
- Invested in Success: A Qualitative Study of the Experience of CenteringPregnancy Group Prenatal Care for Perinatal Educators
- Infant Formula Feeding at Birth Is Common and Inversely Associated with Subsequent Breastfeeding Behavior in Vietnam
- Effectiveness of the Baby Friendly Community Initiative in Italy: a non-randomised controlled study
- Severe and Moderate Acute Malnutrition Can Be Successfully Managed with an Integrated Protocol in Sierra Leone
- Antenatal peer support workers and initiation of breast feeding: cluster randomised controlled trial
- The effect of a programme of organised and supervised peer support on the initiation and duration of breastfeeding: a randomised trial
- Interventions to promote breast-feeding: applying the evidence in clinical practice
- Promoting Breastfeeding: What Works and What Doesn't
- Continuity of Care: "It Is About Connecting"
- 'The Expert ... Is the Patient in Front of Us'
- In This Issue: Health Care Inequalities