
Abstract
PURPOSE There is currently too few endoscopists to enact a national colorectal cancer screening program with colonoscopy. Primary care physicians could play an important role in filling this shortage by offering screening colonoscopy in their practice. The purpose of this study was to examine the safety and effectiveness of colonoscopies performed by primary care physicians.
METHODS We identified relevant articles through searches of MEDLINE and EMBASE bibliographic databases to December 2007 and through manual searches of bibliographies of each citation. We found 590 articles, 12 of which met inclusion criteria. Two authors independently abstracted data on study and patient characteristics. Descriptive statistics were performed. For each outcome measure, a random effects model was used to determine estimated means and confidence intervals.
RESULTS We analyzed 12 studies of colonoscopies performed by primary care physicians, which included 18,292 patients (mean age 59 years, 50.5% women). The mean estimated adenoma and adenocarcinoma detection rates were 28.9% (95% confidence interval [CI], 20.4%–39.3%) and 1.7% (95% CI, 0.9%–3.0%), respectively. The mean estimated reach-the-cecum rate was 89.2% (95% CI, 80.1%–94.4%). The major complication rate was 0.04% (95% CI, 0.01%–0.07%); no deaths were reported.
CONCLUSIONS Colonoscopies performed by primary care physicians have quality, safety, and efficacy indicators that are comparable to those recommended by the American Society of Gastrointestinal Endoscopy, the American College of Gastroenterology, and the Society of American Gastrointestinal Endoscopic Surgeons. Based on these results, colonoscopy screening by primary care physicians appears to be safe and effective.
- Colonoscopy
- colorectal cancer
- physicians, family
- internist
- general practitioners
- primary care physicians
- primary health care
- mass screening
INTRODUCTION
Colorectal cancer1–4 is the third most common cancer and second leading cause of cancer mortality in the United States.5 Guidelines recommend colonoscopy as a suitable screening method,1,4,6,7 and evidence is increasing that colonoscopy may be the most cost-effective approach.3,8–14 As a result, the demand for screening colonoscopy is rapidly growing. The resources needed to screen every eligible person using colonoscopy do not currently exist in the US medical system, however,15 and fewer than one-third of those who are eligible for colonoscopy are screened.3,16
There has been a recent call for monitoring quality indicators in endoscopy to support continuous quality improvement among endoscopists. Proposed measures for quality include reach-the-cecum rates, adenoma detection rates, advanced adenoma detection rates, and withdrawal times.14,17,18 In the United States, a comprehensive task force of the American Society of Gastrointestinal Endoscopists and the American College of Gastroenterology has recommended acceptable standards for these quality measures based on a comprehensive review of the literature.19 In the United Kingdom, the Joint Advisory Group on GI Endoscopy (JAG) established standards for colonoscopies regardless of specialty. These standards state that a colonoscopist perform at least 150 colonoscopies during training, perform 150 colonoscopies annually, and have a reach-the-cecum rate of at least 90%.20
No systematic data are available that document the safety and efficacy of primary care physicians in performing screening colonoscopies. The purpose of this study was to perform a systematic review and meta-analysis of studies that evaluated the quality and safety of screening colonoscopies performed by primary care physicians.
METHODS
Data Sources and Searches
A literature search was conducted in MEDLINE from 1966 to December 2007 and EMBASE from 1974 to December 2007 to retrieve all articles addressing colonoscopy performed by primary care physicians. To ensure complete retrieval of information, the search topics were expanded to include the practice of primary care physicians, family physicians, internists, and colorectal cancer. The primary care concept would thus include all clinical care settings, such as private practice, hospital, and rural physicians. MeSH terms and the search strategy are listed in the Supplemental Appendix, available online at http://www.annfammed.org/cgi/content/full/7/1/56/DC1. Reference lists of included studies were systematically reviewed for additional studies. In addition, researchers and experts belonging to a listserv of primary care endoscopists were asked to provide lists of relevant studies and unpublished studies.
Study Selection
A study was included in the meta-analysis if it reported on colonoscopies performed by primary care physicians, defined as family physicians, internists, obstetricians and gynecologists, and general practitioners. The studies included retrospective cohort studies as well as 1 case-control study. Studies were excluded if they were nonclinical or did not provide outcome data on the colonoscopies or if the colonoscopies were not performed by primary care physicians. All potentially eligible trial reports were read by 2 authors of this study (T.W., B.L.), and disagreements concerning eligibility were resolved by discussion.
Data Extraction and Quality Assessment
Two of the authors (T.W., B.L.) independently reviewed each study and extracted the study and patient characteristics. These characteristics included patient demographics, adenoma and adenocarcinoma detection rates, reach-the-cecum rates, use of sedation, training of endoscopists, and major complications, including death, perforation, and bleeding.
Data Synthesis and Analysis
Although many studies in our series involved more than 1 colonoscopist, most did not report outcomes by the individual colonoscopist; instead, they reported only aggregate outcomes. Initial examination for the presence of heterogeneity in reach-the-cecum rate across studies was performed using the χ2 test of association. For each of 4 binomially distributed outcomes (reach-the-cecum rates for both sedated and unsedated patients, adenoma detection rates, and adenocarcinoma detection rates), we fit logistic regression models using the GLIMMIX procedure in SAS 9.1 (SAS Institute, Cary, North Carolina). Each model included an intercept and study factor, with the study factor (representing each of the 12 included studies) treated as a random effect. This random effects modeling enabled assessment of the between-study variability for each outcome and accounted for differences in the number of procedures per study to obtain an overall estimate for each outcome measure. Predicted values obtained from each model were transformed using this procedure to provide both overall and study-specific estimated success rates and 95% confidence intervals (CIs).
Quality scores, such as Jadad score, have been used in the meta-analysis of randomized clinical control trials.21 No quality score has been developed for the use of nonrandomized studies, however, and the use of quality scores in meta-analysis of observational studies is controversial and may lack proven validity.22 Accordingly, no quality scores were computed for the individual studies. We did, however, adhere to the guidelines for reporting meta-analysis of observational studies in epidemiology (MOOSE guidelines).23
RESULTS
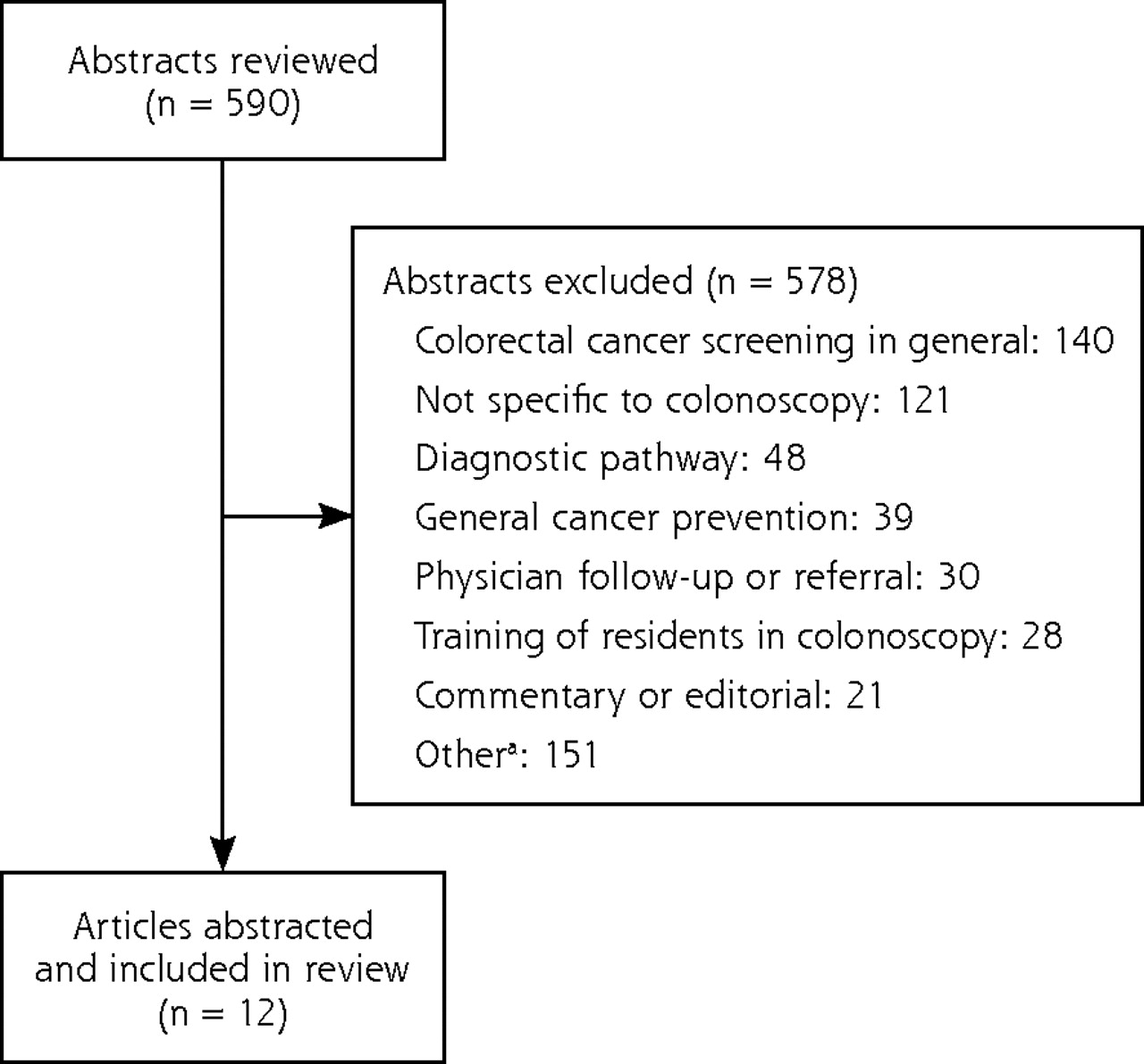
Our search found 590 potentially eligible trials. We subsequently excluded 578 trials for the following reasons: 140 were for colorectal cancer screening in general; 121 were not specific to colonoscopy; and the remaining 317 studies met other criteria for exclusion, such as resident education in colonoscopy, patient compliance with screening recommendations, and the capacity to perform colonoscopy. Figure 1⇓ displays the search results and study flow diagram. The analysis therefore included 12 trials. There were 11 retrospective cohort studies and 1 case-control study. Table 1⇓ summarizes the study characteristics. No randomized trials, systematic reviews, or meta-analysis were identified.
Summary of Studies

Search results and study flow diagram.
a Includes patient compliance with screening, capacity to perform colonoscopy, conscious sedation, patient characteristics, learning effect on the number of procedures, colon cancer treatment, genetics of colon cancer.
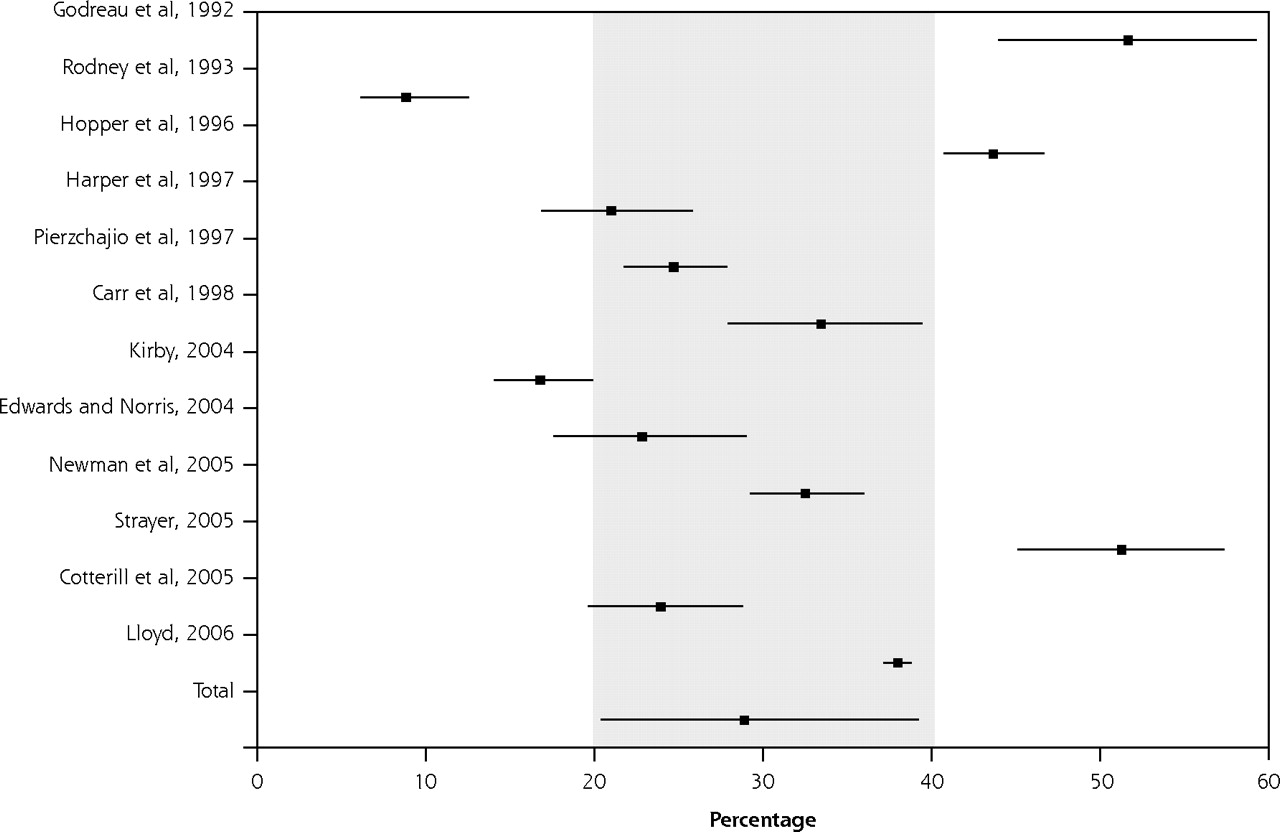
Table 2⇓ summarizes the results of the analysis. These 12 studies included a pooled sample size of 18,292 patients. The mean age was 59 years, and 50.5% were women. Using the random effects models, the estimated mean adenoma detection rate was 28.9% (95% CI, 20.4%–39.3%) and the estimated mean adenocarcinoma rate was 1.7% (95% CI, 0.9%–3.0%). The estimated mean reach-the-cecum rate was 89.2% (95% CI, 80.1%–94.4%). A χ2 test of association found that reach-the-cecum rates varied significantly between the studies (P <.001). Figures 2⇓ and 3⇓ display the forest plots of adenoma detection rates and reach-the-cecum rates. No deaths were reported in any of the studies. There were 4 patients with bleeding complications and 3 patients with colonic perforations, resulting in a major complication rate of 0.04% (95% CI, 0.01%–0.07%).
Estimated Rates of Colonoscopy Quality Outcomes Using Random Effects Modeling

Forest plot of adenoma detection rates.

Forest plot of reach-the-cecum rates.
Funnel plots (Supplemental Figures 1–3, available online at http://www.annfammed.org/cgi/content/full/7/1/56/DC1) were generated for adenoma and adenocarcinoma detection rates and reach-the-cecum rates. There was a mostly symmetric distribution in the funnel plots for adenoma detection rates and reach-the-cecum rates, indicating an absence of publication bias. That the funnel plot for adenocarcinoma detection rates is less symmetric may indicate the presence of publication bias for this outcome.
DISCUSSION
It has been suggested that 90% or more of all colonoscopies should reach-the-cecum and that it should increase to 95% or higher when the indication is for colorectal cancer screening.19,36 The reported experience in practice varies. In 1 series of 6 gastroenterology fellows who were in their last 7 months of training and who had already performed a mean of 328 colonoscopies, the reach-the-cecum rate was 86% (range, 73%–93%).36 The reach-the-cecum rate for the attending endoscopist performing the colonoscopies without a fellow was 97%. In 2003 another series reported on 17,868 colonoscopies by 69 “fully trained” endoscopists in 7 hospital centers in North America.37 In this study, the median cecal intubation rate was 88% (interquartile range, 83%–91%). Only 55% of endoscopists achieved a mean cecal intubation rate of more than 90%, and for 9% of endoscopists the rate was less than 80%. In a prospective analysis of 13,580 colonoscopies performed by surgical endoscopists, the reach-the-cecum rate was 92%.38
We found an overall reach-the-cecum rate of 89.2% (95% CI, 80.1%–94.4%) with colonoscopies performed by primary care physicians. In a sensitivity analysis, we recalculated the preceding values for several different subgroups. Most colonoscopies now involve the use of conscious sedation. If only sedated colonoscopies are included, the reach-the-cecum rate rises to 90.5% (95% CI, 83.1%–94.8%). One study was an outlier with a reach-the-cecum rate of only 48.7%. This study involved cases collected between 1985 and 1990, much earlier than the other studies, and the poor results may have been due to lesser technology or older techniques. If this study is excluded, the overall reach-the-cecum rate is 92.0% (95% CI, 86.7%–95.3%).
The adenoma detection rate is an important quality indicator for the effectiveness of colonoscopy because the goal of colonoscopy is to detect neoplastic lesions and remove polyps. The estimated adenoma detection rate in our meta-analysis is 28.9% (95% CI, 20.4%–39.3%). If one study (an outlier with adenoma detection rate of 8.8%) is excluded, the adenoma detection rate increases to 31.7% (95% CI, 24.0%–40.7%). This detection rate is within the recommended rates by the Task-force on Quality in Endoscopy.19 Practice variability is also found among specialists, however. There are disparities in detection rates among gastroenterologists in private practice (9.4% to 32.7%) and those in academic practice (25% to 40%).17,19 The adenoma detection rate has been reported as 34.2% by surgical endoscopists.38
The complication rates for colonoscopy in this series were well within suggested quality indicators.19 The overall bleeding risk for postpolypectomy bleeding should be less than 1%, and most instances can be managed nonoperatively.19 Available data suggest that perforation rates should be less than 0.2% overall or 0.1% in screening colonoscopies.19 There were 7 major complications in the 18,292 colonoscopies in this series (0.04%). Four complications (0.02%) involved bleeding from a polypectomy site. These patients were managed nonoperatively and were electively hospitalized overnight. Transfusion was not required in these cases. In this series 3 perforations occurred (0.02%). The first perforation was diagnosed at the time of the colonoscopy and was managed without surgery. The other 2 perforations were repaired surgically: 1 perforation was identified at the time of the colonoscopy, and the other perforation was identified 1 week after the procedure. There were no deaths.
There are several limitations to our review. Most colonoscopies were performed by family physicians; other primary care specialties may have been under-represented in our search strategy. There may have been publication bias that affected our primary outcomes; however, we contacted experts in the field for unpublished studies to supplement our search. Additionally, our funnel plots were symmetric for adenoma detection rates and reach-the-cecum rates, indicating an absence of publication bias for these outcomes. Our results apply to primary care physicians who had colonoscopy training and are not generalizable to all primary care physicians. Colonoscopy training varied considerably among studies and was inconsistently reported. Training included self-study, didactic courses, continuing medical education courses, model training, and proctored procedures by mostly general surgeons or occasionally by family physician endoscopists and rarely by gastroenterologists. Most studies did not report the numbers of colonoscopies completed during training. Because this study is a meta-analysis of case-control and cohort studies, the results are subject to the limitations of these types of studies, including lack of randomization and possibility for confounding variables. Our comprehensive search of the literature, however, found only observational study data, and no randomized clinical control trial was found.
Patient preference, cost, and other factors (eg, comorbidities, life expectancy) should be considered when contemplating a population-based colorectal cancer screening program. Although there appears to be a national move toward colonoscopy as the preferred method for colorectal cancer screening, other modalities remain acceptable screening methods. Yet, less than one-third of the US population is currently completing recommended colorectal cancer screening tests of any kind, and even fewer are screened by colonoscopy. Currently, there are insufficient numbers of endoscopists in the United States to implement a full-scale national screening program. With slightly more than 12,000 board-certified gastroenterologists in the United States, the capacity for a national endoscopic colorectal cancer screening program is limited. Any national screening program should consider all available and proven modalities for screening, eg, fecal occult blood tests.
Colonoscopies performed by primary care physicians are safe and effective. Quality indicators are well within the range of published literature for those performed by specialists and the parameters recommended by expert consensus. With the current need for greater access to colorectal cancer screening and the growing body of evidence for colonoscopy as the screening modality of choice, primary care physicians trained in colonoscopy can play a fundamental role in providing access to colonoscopy for colorectal cancer screening.
Footnotes
-
Conflicts of interest: The authors declare no potential, perceived, or real conflict of interest.
-
Funding support: For the academic year of 2006, part of Dr Taylor’s time was supported by a grant from Health Resources and Services Administration Academic Units (grant 2 D12 HP 00023-04) while at the Medical University of South Carolina, Charleston, South Carolina.
- Received for publication January 17, 2007.
- Revision received July 25, 2008.
- Accepted for publication August 4, 2008.
- © 2009 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Colorectal cancer screening within colonoscopy capacity constraints: can FIT-based programmes save more lives by trading-off more sensitive test cut-offs against longer screening intervals?
- Endoscopic Services in the United States: By Whom, for What, and Why?
- Alberta Family Physician Electronic Endoscopy study: Quality of 1769 colonoscopies performed by rural Canadian family physicians
- Expanding Access to Colorectal Cancer Screening: Benchmarking Quality Indicators in a Primary Care Colonoscopy Program
- Successful Endoscopic Repair of an Iatrogenic Colonic Perforation During Diagnostic Colonoscopy
- Test Performance of Immunologic Fecal Occult Blood Testing and Sigmoidoscopy Compared with Primary Colonoscopy Screening for Colorectal Advanced Adenomas
- Patient Satisfaction with Family Physician Colonoscopists
- A Way Forward for Health Care and Healers
- Implementation Insights
- The Complexity of and Opportunity for Screening in Primary Care
- The Aftermath of Efficacy