
Abstract
PURPOSE We wanted to explore the associations between intimate partner violence (IPV) and comorbid health conditions, which have received little attention in male patients.
METHODS Using a computer-based self-assessment health questionnaire, we screened sequential emergency department patients who were urban, male, and aged 18 to 55 years. We then examined associations between types of IPV disclosures, co-occurring mental health symptoms, and adverse health behaviors.
RESULTS Of 1,669 men seeking nonurgent health care, 1,122 (67.2%) consented to be screened, and 1,026 (91%) completed the screening; 712 (63%) were in a relationship in the past year. Of these men, 261 (37%) disclosed IPV: 20% (n = 144) disclosed victimization only, 6% (n = 40) disclosed perpetration only, and 11% (n= 77) disclosed bidirectional IPV (defined as both victimization and perpetration in their relationships). Men disclosing both victimization and perpetration had the highest frequencies and levels of adverse mental health symptoms. Rates of smoking, alcohol abuse, and drug use were likewise higher in IPV-involved men.
CONCLUSIONS A cumulative risk of poor mental health and adverse health behaviors was associated with IPV disclosures. Self-disclosure by men seeking acute health care provides the potential for developing tools to assess level of risk and to guide tailored interventions and referrals based on the sex of the patient.
- Male intimate partner violence
- violence and mental health
- behavioral health risks
- preventive health screening
- aggression
- interpersonal relations
- violence
- health risk appraisal
- health surveys
INTRODUCTION
Intimate partner violence (IPV), defined as a pattern of assaultive and coercive behaviors in intimate relationships, remains a major public health concern in the United States.1,2 The health care system advocates screening women for victimization and referring them to legal and community-based advocacy services. Both men and women, however, perpetrate a wide range of emotional and physical violence against their intimate partners, and3–5 bidirectional IPV may be more common than generally recognized in medical settings.6,7 Substance abuse and mental health problems have been found to be major cofactors in IPV,8–10 and there is reason to believe that interventions aimed at reducing violent behavior will be only marginally effective if co-occurring mental health and substance abuse problems are ignored.11–15 Recent research targeting substance use along with IPV behavior is promising.16–18
The US Preventative Service Task Forces ranked the evidence in favor of routine screening for family violence as inconclusive and raised concerns for possible harm from retaliatory IPV after disclosure. Although it is reasonable to consider whether IPV-involved men could benefit from treatment under a medical model, the topic requires more study. Numerous studies quantify the co-occurrence of IPV and adverse mental health symptoms and substance use in women patients,19–21 but fewer address these issues in IPV-involved men.22 In fact, there are few venues for IPV-involved men to receive help outside the criminal justice setting.23 The acute health care setting may be one such potential venue.24
A recent editorial citing the presence of IPV perpetrators in the emergency department setting called for research on their identification and potential for treatment,25 as the emergency department may be the only contact with a health care clinician for low-income and medically underinsured patients.26 Previous work suggests both male and female patients will disclose IPV perpetration and victimization on a computer-based health risk assessment in an emergency department setting, knowing the clinician will see the results.27 Likewise, MacMillan et al28 found patients preferred self-administered screening.
The larger investigation ascertained the safety and effectiveness of screening urban patients for IPV victimization and perpetration using a computer kiosk29 and assessed mental health symptoms in IPV-involved women.30 In this article, we focus on the mental health correlates of IPV in male patients. Our second objective was to identify the strength of the associations between types of abuse disclosed (emotional, physical, and sexual, as well as both unidirectional and bidirectional IPV) and the number of co-occurring mental and behavioral health problems in men. We predicted more IPV disclosure in men would be positively associated with an increase in adverse mental health symptoms and substance use.
METHODS
Study Design
Our cross-sectional study (with a small prospective follow-up) was made up of primarily African American men seeking care in emergency departments who self-reported being in a relationship in the past year and answered questions about IPV involvement (victimization, perpetration, or both) at a computer kiosk. Four groups of male patients were compared (those disclosing IPV victimization, perpetration, both victimization and perpetration, and those with no IPV disclosures) with respect to mental health symptoms, alcohol use, and use of tobacco and street drugs. All patients who reported IPV received brief counseling and referrals. To assess the safety of the screening process, we collected 1-week and 3-month follow-up information on all victims. At a follow-up interview, which took place in the emergency department, we asked about any adverse events related to screening and whether victims had acted on suggested referrals. Because emergency departments are notorious for poor follow-up rates, we also tracked 911 calls from the addresses of all screened patients living in the surrounding police district for 6 months before and 6 months after the screening visit as a measure of retaliatory violence.29
Selection of Participants and Setting
The study site was in a large southeastern city at a public hospital and trauma center that treats 105,000 patients a year. Sequential eligible patients between the ages of 18 and 55 years were approached in the emergency department waiting room during predetermined study times. Participants were excluded if they could not read English at a 5th-grade level or were intoxicated, acutely psychotic, or too ill to stand and complete a 20-minute health-assessment questionnaire. All participants were taken to a semiprivate booth in the waiting room, where they were invited and, if interested, consented to participate in a study using a computer-based health risk assessment. They received health information and tailored community referrals based on their disclosed health risks. The university institutional review board approved the study.
Data Collection
We collected standard demographic information and, when possible, used validated questions to measure IPV, depression, traumatic stress, suicidality, and substance use, as well as general health. Participants were free to stop the computer-screening process at any point for any reason, and they were encouraged to stop if they were called to see the physician or became too sick. Any patient who disclosed current suicidality was immediately referred to the attending physician for evaluation.
Methods of Measurement
IPV victimization and perpetration questions were only asked of patients who said they had been in a relationship in the past year. Victimization was assessed using The George Washington University Universal Violence Prevention Screening Protocol,24 which consists of 6 questions previously validated in our population.31 To assess perpetration, we used a modified version of a scale developed by the first author32,33 that consisted of 8 questions assessing controlling behavior, verbal aggression, attitudes toward physical and sexual aggression, and both physical and sexual abuse of a current partner. The questions and validation information for both IPV scales are available in the Supplemental Appendix, available online at http://www.annfammed.org/cgi/content/full/7/1/47/DC1.
We used the Beck Depression Inventory-II (BDI-II)34 to ascertain the presence and severity of depressive symptoms. Total BDI-II scores of 20 or higher, indicative of moderate or severe levels of depressive symptoms, were coded as presence of depressive symptoms.35 We used part 3 of the Posttraumatic Stress Diagnostic Scale36 to determine the presence and severity of symptoms of posttraumatic stress disorder (PTSD); consistent with recommendations, patients who had scores of 21 or higher, reflective of moderate or severe levels of PTSD symptoms, were coded as having PTSD symptoms. We used the Scale for Suicide Ideation37 to measure suicidal intent. Patients scoring 11or higher were considered positive for suicidal ideation38 and were referred for psychiatric evaluation.
Adverse health behaviors related to alcohol abuse were assessed using the CAGE screening test.39 One positive response is considered indicative of risky drinking and 2 or more are considered at risk for alcoholism.40,41 Because we were also interested in binge drinking, which has a strong association with IPV,8,16 2 questions were added about quantity and frequency (drinking 3 or more days a week and drinking 4 or more drinks on any single occasion), both of which had to be answered in the affirmative to prompt a concern for possible problem drinking. By contrast, health behaviors related to use of tobacco and street drugs were each assessed by single questions: “Do you smoke cigarettes?” and “Have you used any street drugs in the past 4 weeks?” Because use of tobacco and street drugs was not the focus of the study, these behaviors were not incorporated in the current analysis.
Data Analysis
We used SAS statistical software (version 8, SAS Institute, Cary, North Carolina) for data analyses. Proportions and a series of χ2 analyses (or exact distribution alternative) were computed to assess bivariate associations between IPV status (any/none) and demographic and health-related characteristics. We used the t test to compare age distributions by IPV status. We calculated prevalence and prevalence ratios of IPV victimization and perpetration status with 95% confidence intervals to assess bivariate associations between IPV status, mental health symptoms, and health behaviors.
The sample size was calculated from the number of IPV-positive individuals (both men and women) needed for follow-up to assess safety of the IPV screening, about 2 times the number of men needed to assess the association between IPV and mental health reports.
RESULTS
A total of 1,669 male patients were eligible for participation in the survey, and 1,122 (67.2%) consented to participate. No significant differences existed for race, age, or chief complaint between participants and non-participants. Of the men who consented to participate in the study, 1,026 (91%) participants completed all key elements of the questionnaire. Of the screened men, 712 (63%) participants had been in a relationship in the past year and answered questions about past year victimization or perpetration. This group made up our study population.
Table 1⇓ displays the demographic information of the male participants by their IPV status. Most participants were single, African American, and uninsured. In general, IPV-involved men were less educated and less likely to be employed. They were more likely to be separated or divorced and more likely to report moderate to severe symptoms of depression, PTSD, and suicidality. IPV-involved men also were more likely to engage in other adverse health behaviors, including smoking, at-risk drinking, street drug use, nonuse of seatbelts, and risky sexual behavior.
Demographic Characteristics of Male Emergency Departments Patients in Relationships (N = 712)*
Table 2⇓ shows the number and percentages of men in relationships and who were positive for IPV victimization and perpetration by each question on the measures. Of the 712 men, 451 (63%) did not report any IPV, and 261 (37%) disclosed at least 1 type of IPV (emotional, physical, or sexual): 20% (n = 144) disclosed IPV victimization only, 5% (n = 40) disclosed IPV perpetration only, and 11% (n = 77) disclosed bidirectional IPV (both victimization and perpetration). Victimization was reported more often than perpetration, with emotional and physical victimization endorsed more frequently than sexual victimization.
Distribution of “Yes” Answers to Violence-Related Questions by All Men in Relationships Who Completed the IPV Questions on the Computer Survey (N = 712)
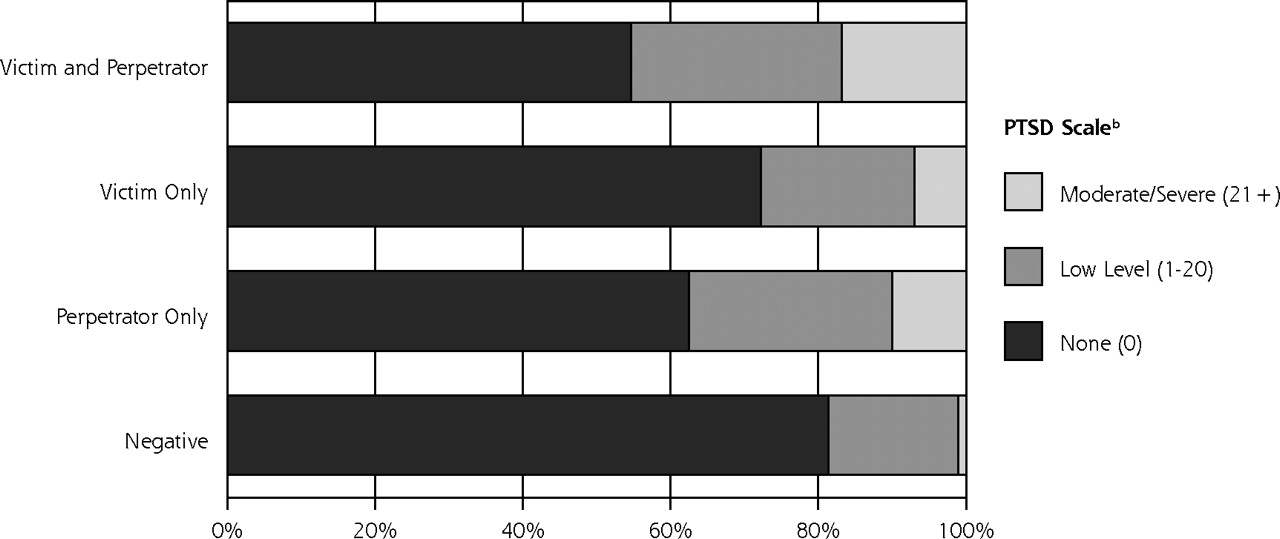
Figure 1⇓ categorizes the mental health symptom scores by the extent of IPV-involvement. Mental health scores in the clinical range (moderate/severe) were more common for those who experienced any IPV and were highest among those reporting both victimization and perpetration; patient reports of any symptoms followed a similar pattern. Table 3⇓ shows the prevalence ratios for both adverse mental health symptoms and unhealthy behaviors by IPV status. Those reporting perpetration only were more likely to report adverse mental health symptoms than those reporting victimization only, but those reporting both victimization and perpetration had the highest levels of adverse mental health symptoms. A similar gradient was identified for adverse health behaviors. The prevalence ratios of drug, tobacco and alcohol use increased as abuse and violence in the relationship increased, with bidirectional IPV having the greatest risks of poor mental health and unhealthy behaviors.
Prevalence Ratios of Mental Health Symptoms and Adverse Health Behaviors by IPV Status for All Men in Relationships Who Completed the IPV Questions on the Computer Survey (n = 712)


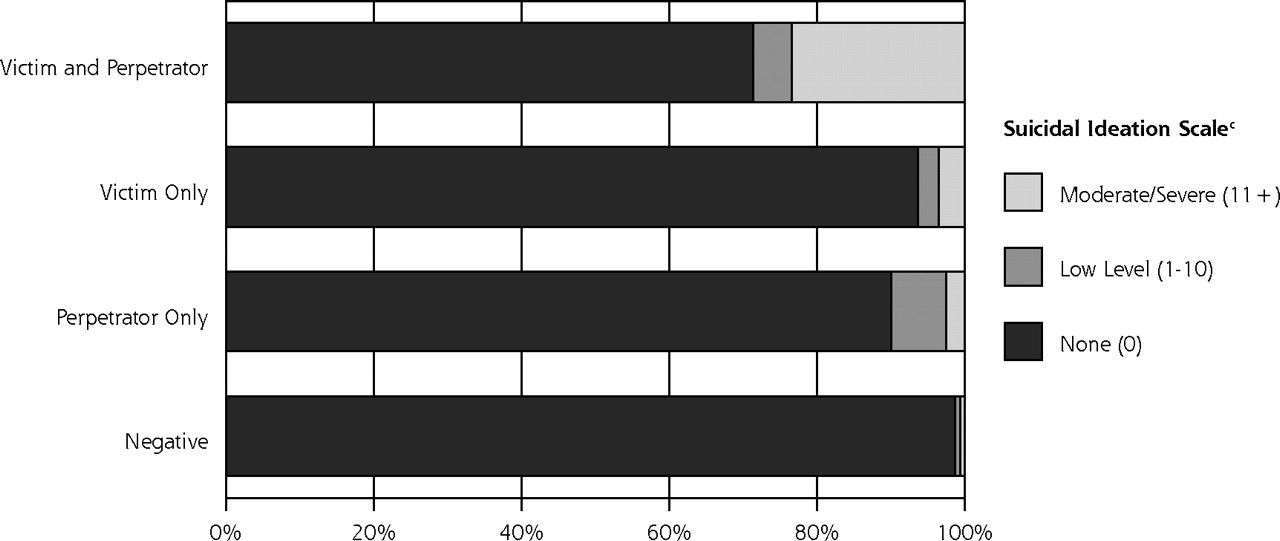
Mental health symptom scores, by intimate partner violence status.
PTSD=posttraumatic stress disorder.
a Depression measured by the Beck Depression Inventory: ≥20 are indicative of moderate or severe levels of depressive symptoms.34,35
b Posttraumatic Stress Diagnostic Scale: scores of >20 reflect moderate or severe levels of PTSD symptoms.36
c Scale for Suicide Ideation: patients with scores of >11 were considered suicidal and referred for psychiatric evaluation37,38
There were no detectable adverse events related to screening, either observed by the research assistants in the emergency department or reported by the 80 (56%) of male victims who returned for 1-week follow-up. Nor did we identify any increase in 911 calls to the addresses of screened men, regardless of IPV status (Table 4⇓).
Rates of 911 Telephone Calls to Addresses of Male Study Participants 6 Months Before and After Screening
For the men disclosing victimization who returned to the emergency department for follow-up visits, Table 5⇓ shows 1-week and 3-month use of referral resources. At 1 week, 55% said they had read the educational and referral information provided, and 13% had contacted IPV resources. Although only 47 male victims returned at 3 months, 15 (32%) reported they had contacted the referral resources; of those, 8 (17%) had sought mental health counseling, and 5 (11%) had sought alcohol counseling.
Most Frequently Reported Use of Resources and Safety Measures Taken by Male Patients Who Screened Positive for IPV Victimization
DISCUSSION
We found that men coming to an urban emergency department for nonurgent complaints self-disclosed a substantial amount of IPV; 37% of men in an intimate relationship in the past year disclosed IPV victimization, perpetration, or both. Results regarding confounding factors, such as social disadvantage, support a general pattern of cumulative exposure leading to increased risk.42–44 The amount of IPV involvement was associated with increasing proportions of patients reporting moderate/severe mental health symptoms. Depression, PTSD, and suicidality scores all were higher, and those experiencing and/or perpetrating more types of abuse had the highest number of adverse mental health symptoms. Proportions of smoking, drinking and street drug use were also higher in IPV-involved men, providing further support that at least some of the adverse health effects associated with violence may be due to unhealthy behaviors.45 This finding is similar to that of other studies which found multiple comorbid health conditions in patients with high trauma exposure.45–49
There are studies on the psychological comorbidities of men in court-mandated batterer’s treatment.10,15 Our work lends support to studies that describe the co-occurrence of IPV with depression and substance abuse in IPV-involved individuals.50
El-Bassel et al described rates of IPV and substance abuse in women of ethnic minorities,51 and others have assessed the mental health impact of IPV in women,18,20,21 but less attention has focused on the mental health symptoms and substance abuse problems of IPV-involved men coming to health care settings.
Looking specifically at emergency department patients, Lipsky et al found 15% of male patients in a Los Angeles emergency department self-reported current IPV perpetration, including 17.1% of African American and 9.1% of Latino male patients.52 In our study, the cumulative amount of abuse disclosures (emotional, physical, sexual) and amount of unidirectional and bidirectional violence (victimization, perpetration, or both) were related in a dose-response manner to levels of depression, PTSD, and suicidal ideation.
Given the high degree of overlap, one could argue that identifying male partner violence should be a part of any mental health and substance abuse assessment. The literature on screening men in health care settings as part of comprehensive health risk assessments is scant, however. Several studies report that men screened in the emergency department for partner violence had rates of partner violence similar to that of women; between 13% and 30% of men in various emergency department samples report current physical IPV victimization.52–54 Others have concluded that many of these men were abusers.55–57 Among men in a batterer’s treatment program, 46% said they had seen a physician in the last 6 months; the emergency department was the most common site.58 Because the emergency department is likely to see a heterogeneous group of men with varying levels of IPV risk, it will be important to identify men’s IPV victimization as well as their perpetration, along with comorbid conditions that might lend themselves to intervention.
Most assessments and interventions with IPV-involved men have been through the criminal justice system, which uses a one-size-fits-all model of group didactics and cognitive restructuring.59 Only a small fraction of IPV-involved men engage in treatment, however, and less than one-half subsequently complete these programs.60,61 Not surprisingly, many interventions for IPV-involved men have been unable to show any effectiveness.62,63 In part, this lack of effectiveness may be because current interventions for IPV have often failed to address adequately the comorbid mental health and substance abuse problems that may exist for both victims and perpetrators. One central problem in the field of IPV batterer’s treatment is how to best match types of interventions to subpopulations of perpetrators.64 New methods for identification and risk stratification of IPV need to account for the severity and periodicity of occurrences, as well as comorbid conditions. If it can be determined that routine IPV screening with men in health care settings is safe, we can add additional tools to improve recognition of high-risk situations and make distinctions between broad categories of male partner violence. Improving our understanding of the interactions between mental health and violence as they relate to the complexities of human relationships will be important if we are to develop new tailored interventions that can be delivered outside of the criminal justice system.65
Limitations
This study has a number of important limitations. The patient population was a fairly homogeneous convenience sample of urban, primarily indigent, African American men seeking health care at 1 large county hospital emergency department, which limits generalizability. Only nonurgent patients were recruited; thus, we may have missed the more severe forms of IPV seen with major trauma. Although there was no indication of any safety concerns related to screening men for IPV based on observation during the emergency department visit self-report at 1 week or an increase in 911 telephone calls to their addresses, we were only able to follow up on 55% of male victims at 1 week. Also the study method of using 911 calls to their address can result in misclassification, because we did not track the 911 calls by individual, just by address. So there may have been undetected adverse events. IPV was self-reported and therefore subject to recall bias or unwillingness to disclose. There was no external validation of the actual levels and types of IPV, so the potential for classification error warrants caution when interpreting our results. Although we tried to use validated screening tools, IPV is best validated by partner report, and more work is needed to improve the sensitivity and specificity of screening tools for IPV in male patients in health care settings.
In conclusion, we found a cumulative risk of depressive and PTSD symptoms, suicidal ideation, and substance abuse to be associated with violence in the relationships of male urban emergency department patients. The identification of IPV risk in men as part of a health risk assessment provides opportunities for new targeted IPV interventions delivered outside the criminal justice setting. Such interventions must be guided by an understanding of the heterogeneity of male partner violence and co-occurring behavioral and mental health issues.
Acknowledgments
The authors wish to acknowledge Joanna Bisgaier, MSW, for help with manuscript preparation, James Wiley, PhD, for inspiration and conceptual clarity, and the many other people who have contributed to this project, particularly our research assistants, Robin Schultz Kemball, MPH, and Hadley Mintz, MPH, and the staff and patients of Grady Hospital Emergency Department.
Footnotes
-
Conflicts of interest: none reported
-
Funding support: The data used in this study was collected with support from Centers for Disease Control and Prevention, R49 423113. Karin Rhodes, MD, MS, was supported by a grant from the National Institute of Mental Health, K23 MH64572; Debra Houry, MD, MPH, was supported by a grant from the National Institute of Mental Health, K23069375.
- Received for publication November 2, 2007.
- Revision received July 2, 2008.
- Accepted for publication July 14, 2008.
- © 2009 Annals of Family Medicine, Inc.
REFERENCES




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- "What matters in help-seeking and disclosure intent of intimate partner violence during the COVID-19 pandemic: Similarities and differences across demographic groups"
- Risk Factors and Moderators of Intimate Partner Violence Victimization Versus Perpetration Among Women in Spain
- "I've Never Felt Such Absolute Devastating Loss": A Photo Elicitation Exploration of Men's Postseparation Experiences of Coping After Intimate Partner Violence
- Deployment Experiences and Suicidal Behaviors Related to Interpersonal Violence Perpetration Among Army National Guard Soldiers
- Prevalence of Intimate Partner Violence and Beliefs About Partner Violence Screening Among Young Men
- Intimate Partner Violence Perpetration and Victimization Among Chinese Young Adults: Profiles and Associated Health Problems
- Human Services Utilization Among Male IPV Perpetrators: Relationship to Timing and Completion of Batterer Intervention Programs
- The Role of the Physician When a Patient Discloses Intimate Partner Violence Perpetration: A Literature Review
- Who Is at Risk for Intimate Partner Violence Victimization: Using Latent Class Analysis to Explore Interpersonal Polyvictimization and Polyperpetration Among Pregnant Young Couples
- Determinants of Intimate Partner Violence in Sub-Saharan Africa: A Review of Prevention and Intervention Programs
- Occurrence and impact of negative behaviour, including domestic violence and abuse, in men attending UK primary care health clinics: a cross-sectional survey
- Characteristics of Men Who Perpetrate Intimate Partner Violence
- Managing Dissonance: Implications for Therapeutic Practice With Partner Violence
- Intimate Partner Violence Among California Couples: Multilevel Analysis of Environmental and Partner Risk Factors
- Rates of Bidirectional Versus Unidirectional Intimate Partner Violence Across Samples, Sexual Orientations, and Race/Ethnicities: A Comprehensive Review
- Implementation Insights
- The Complexity of and Opportunity for Screening in Primary Care