
Abstract
PURPOSE Family and friends who provide regular care for a sick or dependent individual (“caregivers”) are at increased risk of health-related socioeconomic vulnerabilities (HRSVs). This study examined pre-pandemic prevalence of and early pandemic changes in HRSVs among women caregivers compared with non-caregivers.
METHODS A cross-sectional survey was conducted in April 2020 (early pandemic) with 3,200 English-speaking US women aged 18 years or older, 30% of whom identified as caregivers. We modeled adjusted odds of self-reported HRSVs (financial strain, food/housing insecurity, interpersonal violence, transportation/utilities difficulties) before and changes during the early pandemic by caregiving status. Models were adjusted for age, race/ethnicity, marital status, education, income, number of people in household, number of children in household, physical and mental health, and number of comorbidities.
RESULTS Pre-pandemic, 63% of caregivers and 47% of non-caregivers reported 1 or more vulnerability (P <.01); food insecurity was most prevalent (48% of caregivers vs 33% of non-caregivers, P <.01). In the early pandemic, caregivers had higher odds than non-caregivers of financial strain, both incident (adjusted odds ratio [AOR] = 2.1; 95% CI, 1.6-2.7) and worsening (AOR = 2.0; 95% CI, 1.4-2.8); incident interpersonal violence (AOR = 2.0; 95% CI, 1.5-2.7); incident food insecurity (AOR = 1.6; 95% CI, 1.2-2.1); incident transportation difficulties (AOR = 1.9; 95% CI, 1.3-2.6); and incident housing insecurity (AOR = 1.6; 95% CI, 1.1-2.3).
CONCLUSION The coronavirus disease 2019 (COVID-19) pandemic increased risk of incident and worsening HRSVs for caregivers more than for non-caregivers. COVID-19 response and recovery efforts should target caregivers to reduce modifiable HRSVs and promote the health of caregivers and those who depend on them.
Annals Online First article
INTRODUCTION
Throughout the coronavirus disease 2019 (COVID-19) pandemic, family and friend caregivers have played an especially critical role in ensuring the health and well-being of a substantial population of chronically ill and vulnerable people.1 In 2020, 21% of US adults were providing unpaid care to at least 1 family member or friend with health conditions or functional limitations—a substantial increase from 18% in 2015.2 Two-thirds of care recipients are aged 65 years or older, 63% have a long-term physical disability, 32% have cognitive difficulties, and most fall into 1 or more categories of high risk2 for COVID-19 infection and associated poor outcomes. To keep care recipients safe in the ever-changing pandemic environment, the work of many caregivers intensified—more than one-half reported an increase in caregiving intensity and burden following the start of the pandemic.3 In a national sample of caregivers, 83% reported increased caregiving-related stress following the start of the pandemic; increased stress was significantly higher among women caregivers (87%) than men (74%).2
Before the COVID-19 pandemic, caregivers had significantly poorer physical and mental health than non-caregivers.4–11 In addition, caregiving has been associated with health-related socioeconomic vulnerabilities (HRSVs)—including financial strain, food insecurity, transportation difficulties, and others—that are modifiable factors compounding the negative effects of caregiving on physical and mental health.2 Pre-pandemic, 1 in 10 caregivers struggled to pay for food and other necessities for themselves and their care recipient, and women (61% of all US caregivers) were at higher risk for HRSVs than men.12–15
The National Women’s COVID-19 Health Study was designed to capture the experiences of US women early in the pandemic.16 A prior analysis found that nearly one-half of all women experienced incident or worsening HRSVs in the early pandemic period and those who did had 2 to 4 times higher odds of depression, anxiety, and traumatic stress symptoms.16 The present analysis examines differences in prevalence of HRSVs before the pandemic and early in the pandemic for caregivers compared with non-caregivers. We hypothesized that caregivers would be significantly more likely to experience pandemic-related incident and worsening HRSVs compared with non-caregivers. Data are needed that describe HRSVs among caregivers, especially pandemic-related incident or worsening HRSVs, to facilitate caregiver policy and intervention development and inform COVID-19 response and recovery efforts.
METHODS
Design
The National Women’s COVID-19 Health Study, conducted April 10-20, 2020, used a cross-sectional survey design that has been described in depth.16 The University of Chicago Institutional Review Board approved the study protocol and all participants provided digital documentation of informed consent.
Setting
The study was conducted in the United States.
Participants
English-speaking women aged 18 or more years were recruited from a research panel created by Opinions 4 Good. This research panel uses a non-probability, convenience sampling strategy to recruit participants online and through partnering organizations. Panelists were recruited to The National Women’s COVID-19 Health Study via e-mail. Each e-mail included a unique, 1-time use survey link. Panelists’ sociodemographic data, maintained by Opinions 4 Good, facilitated targeted recruitment to fulfill a nested quota sample of 3,200 women. The sample quotas matched the distribution of age and education of the 2018 US population of adult women and oversampled East/Southeast Asian women (Chinese, Filipino, Japanese, Korean, and/or Vietnamese) to achieve the goals of the primary study, which included subanalyses among race/ethnic groups, including East/Southeast Asian women.
Measures
Self-administered, web-based surveys captured: (1) sociodemographic and self-rated health characteristics, (2) caregiving status, (3) main health condition of the care recipient, (4) 6 pre-pandemic HRSVs including financial strain, food insecurity, housing insecurity, interpersonal violence, transportation difficulties, and utilities difficulties, and (5) change in each of the 6 HRSVs “since the start of the pandemic.”
Caregiving status was assessed by a yes/no item from the 2018 Behavioral Risk Factor Surveillance Study questionnaire: “During the past 30 days, did you provide regular care or assistance to a friend or family member who has a health problem or disability?” Participants who indicated “Yes,” were asked “What is the main health problem, long-term illness or disability that the person you care for has?” and provided with a list of 14 conditions.
Pre-pandemic HRSVs were assessed using the Centers for Medicare & Medicaid Services Accountable Health Communities (AHC) screening tool17 and categorized as present or absent using the AHC instructions. Changes in HRSVs “since the start of the pandemic” were assessed using an adaptation of the AHC screening tool questions that used a 5-point Likert response scale (Supplemental Table 1). Change in each HRSV was categorized as: secure (absent pre-pandemic and early pandemic), incident (absent pre-pandemic and present early pandemic), persistent or improved (present pre-pandemic and unchanged or improved early pandemic), and worsening (present pre-pandemic and worse early pandemic). An HRSV was considered incident if the HRSV was absent pre-pandemic based on AHC instructions and the participant indicated a negative change in the early pandemic (eg, food secure pre-pandemic and “a lot more worried” about running out of food in the early pandemic; housing secure pre-pandemic and indicating “I have a place to live today, but I am worried about losing it in the future” in the early pandemic).
Statistical Analysis
Of 3,634 eligible persons contacted, 3,200 were surveyed (88% cooperation rate, calculated as the number of participants who completed the survey divided by the number of eligible persons contacted).18 Of 3,200 participants, 3,167 (99%) were eligible for this analysis (complete data for variables needed for weights and caregiving status). Of the 33 excluded, 24 were excluded due to missing income data required for weights and 9 were excluded due to missing caregiver status.
Post-stratification sample weights were generated using the raking-ratio method with marginal distributions matched to 2018 US population estimates. All analyses were weighted. Differences in sociodemographic and health characteristics by caregiving status were examined using χ2 tests. Prevalence of pre-pandemic HRSVs and change in HRSVs were described by caregiving status. Multivariate logistic regression was used to model the odds of (1) each pre-pandemic HRSV, (2) early pandemic incidence of at least 1 HRSV, (3) incidence of each HRSV among those without that HRSV pre-pandemic, and (4) worsening of each HRSV among those with that HRSV pre-pandemic. All models were adjusted for the following baseline covariates: age, race and ethnicity, marital status, education, income, number of people in household, number of children in household, self-reported physical health and mental health, and number of comorbidities. Covariates were selected for inclusion if known to be associated with HRSVs or caregiving status. No model covariate selection procedures were used. Due to small or null sample size, odds of incident utilities difficulties and worsening housing insecurity could not be calculated. All analyses were performed using Stata/SE version 15.1 (StataCorp LLC). Results from unadjusted logistic regression models are reported in Supplemental Table 2 and Supplemental Table 3.
RESULTS
Nearly 1 in 3 US women (30%, n = 950) in this study were caregivers in the early pandemic phase. The most common conditions among recipients were old age/infirmity/frailty (14%), mental illness (11%), heart disease (9%), and diabetes (9%). Of care recipients, 8% had Alzheimer’s disease or a related dementia. Differences in sociodemographic and health characteristics between caregivers and non-caregivers are shown in Table 1.
Weighted Baseline Characteristics by Caregiving Status (N = 3,167)
Pre-Pandemic Health-Related Socioeconomic Vulnerabilities
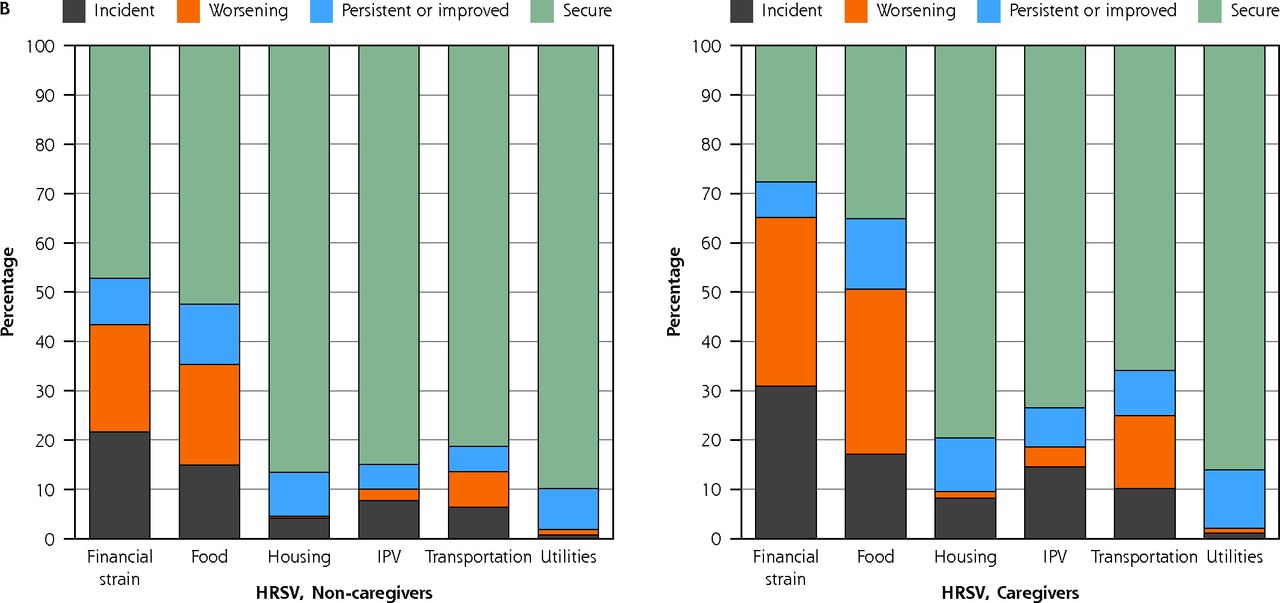
Most caregivers (63%) had 1 or more pre-pandemic HRSVs, but rates were also high among non-caregivers (47%, P <.001). Nearly one-half (42%) of caregivers had 2 or more HRSVs compared with 28% of non-caregivers (P <.01). The most prevalent pre-pandemic HRSVs for caregivers and non-caregivers were food insecurity (48% vs 33%) and financial strain (42% vs 31%) (Figure 1A). When comparing prevalence of HRSVs by main condition of the care recipient, caregivers of people with arthritis/rheumatism had the highest prevalence (87%) of at least 1 pre-pandemic HRSV (66% were food insecure and 63% were experiencing financial strain). Caregivers of people with dementia (47%) and old age/infirmity/frailty (45%) had the lowest prevalence of at least 1 pre-pandemic HRSV (Table 2).


Weighted prevalence of pre-pandemic socioeconomic vulnerabilities (A) and early pandemic changes in socioeconomic vulnerabilities (B) by caregiving status.
AHC = accountable health communities; HRSV = health-related socioeconomic vulnerabilities; IPV = interpersonal violence.
Note: Calibration weights were utilized and were generated based on the following variables: age group, race, education, income, and region. Change in each HRSV was categorized as: secure (absent pre-pandemic and early pandemic), incident (absent pre-pandemic and present early pandemic), persistent or improved (present pre-pandemic and unchanged or improved early pandemic), and worsening (present pre-pandemic and worse early pandemic).
Weighted Pre-Pandemic Prevalence of Caregiver Socioeconomic Vulnerabilities by Condition of Care Recipient
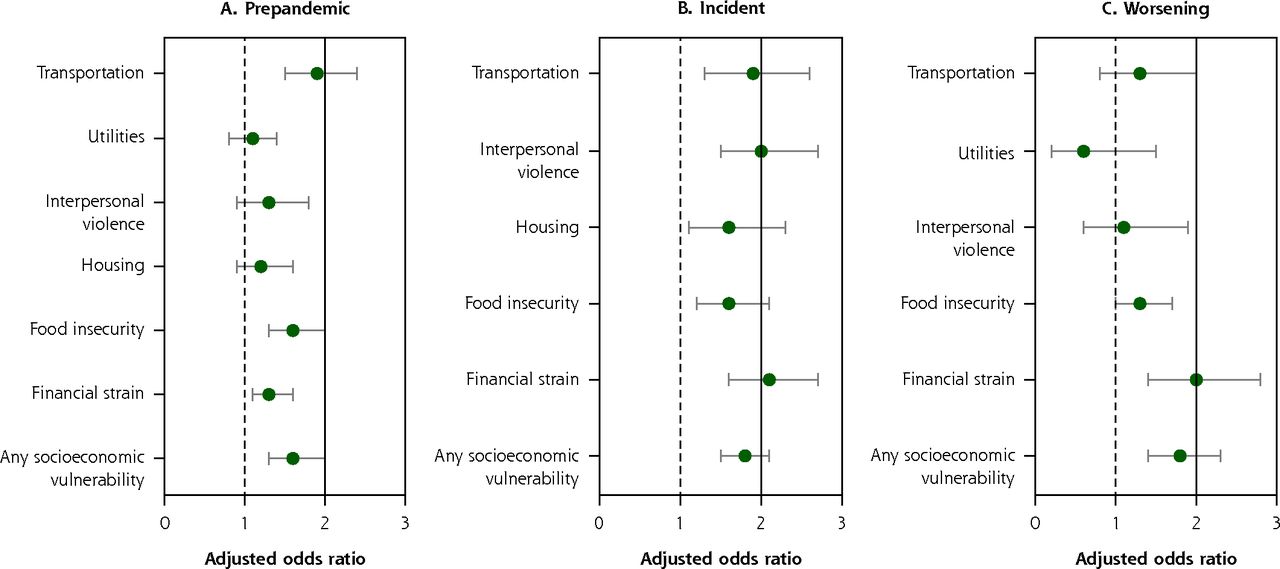
After adjusting for sociodemographic and health characteristics, caregivers had higher adjusted odds of having at least 1 pre-pandemic socioeconomic vulnerability compared with non-caregivers (adjusted odds ratio [AOR] = 1.6; 95% CI, 1.3-2.0) (Figure 2A). Specifically, caregivers had significantly higher adjusted odds of pre-pandemic financial strain (AOR = 1.3; 95% CI, 1.1-1.6), food insecurity (AOR = 1.6; 95% CI, 1.3-2.0), and transportation difficulties (AOR = 1.9; 95% CI, 1.5-2.4) compared with non-caregivers.

Adjusted odds of socioeconomic vulnerabilities: pre-pandemic (A), incident (B), and worsening (C) for caregivers compared with non-caregivers (referent group).
HRSV = health-related socioeconomic vulnerabilities.
Notes: Calibration weights were utilized and were generated based on the following variables: age group, race, education, income, and region. Sample sizes for participants with incident utilities (B) and participants with worsening housing (C) were too small to include in the models. Models adjusted for age, race/ethnicity, marital status, education, income, number of people in household, number of children in household, self-reported physical health and mental health, and number of comorbidities. Change in each HRSV was categorized as: secure (absent pre-pandemic and early pandemic), incident (absent pre-pandemic and present early pandemic), persistent or improved (present pre-pandemic and unchanged or improved early pandemic), and worsening (present pre-pandemic and worse early pandemic).
Early Pandemic Changes in Health-Related Socioeconomic Vulnerabilities
In the early pandemic, 54% of caregivers reported at least 1 incident HRSV compared with 38% of non-caregivers; incidence was higher for every HRSV. Due to higher incidence of individual HRSVs, the difference in prevalence of HRSVs between caregivers and non-caregivers widened for all HRSVs (Supplemental Table 4). The most common incident HRSVs for caregivers and non-caregivers were financial strain (31% vs 22%) and food insecurity (17% vs 15%) (Figure 1B). More caregivers also experienced at least 1 worsening HRSV compared with non-caregivers (50% vs 32%). The most common worsening HRSVs for caregivers and non-caregivers were financial strain (34% vs 22%) and food insecurity (34% vs 20%) (Figure 1B).
In the early pandemic, caregivers had higher adjusted odds of experiencing at least 1 incident HRSV (AOR = 1.8; 95% CI, 1.5-2.1) compared with non-caregivers (Figure 2B). Specifically, caregivers had higher odds of incident financial strain (AOR = 2.1; 95% CI, 1.6-2.7), interpersonal violence (AOR = 2.0; 95% CI, 1.5-2.7), food insecurity (AOR = 1.6; 95% CI, 1.2-2.1), housing insecurity (AOR = 1.6; 95% CI, 1.1-2.3), and transportation difficulties (AOR = 1.9; 95% CI, 1.3-2.6).
In the early days of the pandemic, caregivers had higher adjusted odds of experiencing at least 1 worsening HRSV (AOR = 1.8; 95% CI, 1.4-2.3) compared with non-caregivers (see Figure 2C). Specifically, caregivers had higher adjusted odds of worsening financial strain (AOR = 2.0; 95% CI, 1.4-2.8). See Supplemental Appendix.
DISCUSSION
Consistent with prior US population estimates, one-third of women in this national, early COVID-19 pandemic sample identified as a caregiver. Caregiving in the early pandemic was associated with significantly higher odds of incident HRSVs for every type examined (financial strain, food insecurity, housing insecurity, interpersonal violence, and transportation difficulties), and disparities in prevalence between caregivers and non-caregivers widened for each type, increasing by as much as 9 percentage points (financial strain). In prior studies (not specific to caregivers), these socioeconomic disadvantages were associated with poorer physical and mental health19–25 in both pre- and early pandemic16 phases. Widening HRSV disparities could increase these health disparities and negatively affect the health of care recipients.
Our findings, using data from a national, cross-sectional study16 conducted in April 2020, corroborate those of Beach et al,26 both describing increased worry about food and finances since the start of the pandemic among unpaid family and friend caregivers compared with non-caregivers. That study26 did not assess pre-pandemic HRSVs and, therefore, could not differentiate between new and worsening pandemic-related conditions among caregivers. Importantly, we found that caregivers experienced more new-onset and worsening of prevalent HRSVs in the early pandemic than non-caregivers. HRSVs are potentially modifiable through provision of community resources (eg, food pantries for food insecurity), but early in the pandemic, the Centers for Disease Control and Prevention guidelines (ie, social distancing and masks) and state mandates (ie, stay at-home orders and business closures) limited access to these resources. COVID-19 response and recovery efforts should formally recognize and work to remediate the disproportionate impact of the pandemic on HSRVs among caregivers.
The high rates of financial strain among caregivers found in this study are noteworthy: caregivers of loved ones with arthritis, asthma, and diabetes had the highest prevalence of financial strain during the pandemic onset. Though early pandemic employment rates were higher among caregivers than non-caregivers (56% vs 43%), fewer caregivers were in the highest household income bracket (≥$100,000, 25% vs 31%). Caregiver’s household size was larger (59% vs 46% with 3 or more) and included more children (26% vs 20% with 2 or more) who were now at home due to school closures. Though we did not examine changes in employment or income in this study, a 2019 national study of caregivers reported 61% were employed (similar to the 56% in this study), and that 6 in 10 caregivers endorsed caregiving-related negative impacts on their work.27 Such impacts may have been exacerbated during the pandemic due to state-mandated closures of resources relied upon by employed caregivers—adult daycare, home help, and respite centers.28
Historically, friend and family caregivers have been an invisible, mostly unpaid health care workforce whose efforts represent substantial cost savings to the health care system. In 2017 (the latest available data), the services of unpaid caregivers were valued at more than $470 billion dollars—a value that steadily rose from prior years and exceeded the total value of paid long-term care services as well as out-of-pocket health care spending.29 During the pandemic, caregivers’ responsibilities have grown, with increased needs for emotional support, medical support tasks, and assistance with everyday errands and daily food preparation.30 The value of caregivers’ efforts—both in terms of health care cost savings and lives saved—was likely far higher during the pandemic than before. The increased responsibilities and effects could be seen as a socioecological component of burden that is not captured in existing measures and suggest a need to broaden burden assessments to consider how circumstances affecting the general population may have greater impacts on caregivers.
An especially concerning finding of our study is the incidence of interpersonal violence associated with the early pandemic. More than 1 in 4 caregivers reported experiencing interpersonal violence in the early pandemic—and for more than one-half (15% overall), this was new. We found no prior studies examining interpersonal violence or related constructs (ie, domestic violence, intimate partner violence) among caregivers in the early pandemic. However, a rate of 25% is more than 3 times the pre-pandemic rate of interpersonal violence among women (7%) reported in a national, 10 site clinical study using the same measure.31 Additionally, physician and public health scientists have indicated that pandemic-related mandates (ie, stay-at home orders) and other stressors (eg, loss of employment or income) created conditions likely to increase rates of intimate partner violence, especially among women.32–35 These concerns are supported by hyperlocal data from police reports of rising rates of domestic violence calls.31,32 Prior studies of violence by care recipients toward family caregivers highlight the need for clinicians to sensitively address this violence given the unique relationship between the caregiver and care recipient. Clinical guidelines and interventions specific to caregivers who are abused are needed to implement this call-to-action, especially given the pandemic-related increase in interpersonal violence among caregivers.
Limitations
This study should be interpreted in light of several limitations. Participants were enrolled from a non-probability research panel with a very high response rate, which may limit generalizability. Using a previously enrolled research panel, however, allowed rapid enrollment of a large sample to study early pandemic effects. In addition, use of post-stratification sample weights for the variables of age group, race, education, income, and region in all analyses forces the sample to match the marginal distributions of 2018 US population estimates on these factors, increasing likelihood of generalizability. Notably, the proportion of caregivers and the sociodemographic and health characteristics of the study participants were similar to other studies, including a 2020 nationally representative probability sample of caregivers.2,27 For example, the proportion of non-Hispanic White caregivers was 61% in our study and in this national sample.2 Also, caregiving experience differed depending on the care recipients’ condition(s). Though we were able to qualitatively compare rates of HRSVs by care recipient’s main condition, sample size limited these analyses. Lastly, this survey was done at a single time point and some responses, including those assessing pre-pandemic states, may be subject to recall or other bias. This study did not directly assess changes in caregiving demand or habits, including caregiving intensity.
CONCLUSIONS
As of 2020, more than 53 million Americans provided care for a friend or family member—a number projected to grow as the population ages and fertility rates decline. Additionally, people having long-term COVID-19 complications may rely on friend and family caregivers.36–39 Supports for caregivers, including financial support, supportive workplace policies, community-based resources, and other infrastructure that reduces health-related socioeconomic vulnerabilities are essential to ensuring caregivers can continue to provide needed support for a growing population of vulnerable care recipients. COVID-19 response and recovery efforts, including the American Jobs Plan, should emphasize building infrastructure that reduces modifiable HRSVs among caregivers.
Footnotes
Conflicts of interest: Lindau is the founder and Chief Innovation Officer of NowPow, LLC, a Unite Us company. She is also founder and President of MAPSCorps, 501c3. Neither the University of Chicago nor University of Chicago Medicine is endorsing or promoting any NowPow/MAPSCorps/Unite Us entity or its business, products, or services. The research described here is conducted under the auspices of a University of Chicago conflict of interest management plan. Lindau holds debt in Glenbervie Health, LLC and health care–related investments managed by third parties. Lindau is a contributor to UpToDate, Inc. All other authors have no conflicts of interest to declare.
Funding support: Research reported in this publication was supported by 5R01AG064949 (K.B., S.T.L., J.A.M., V.W), 5R01MD012630 (K.B., S.T.L., J.A.M., V.W), R21CA226726 (S.T.L.), and 1R01DK127961 (S.T.L., J.A.M., V.W). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Previous presentation: Portions of the research reported in this publication were presented as a poster at the Interdisciplinary Association of Population Health Sciences; October 18, 2021; Baltimore, Maryland.
- Received for publication October 27, 2021.
- Revision received March 25, 2022.
- Accepted for publication April 1, 2022.
- © 2022 Annals of Family Medicine, Inc.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.