
Article Figures & Data
Figures
- Figure 1
Overview of study design.
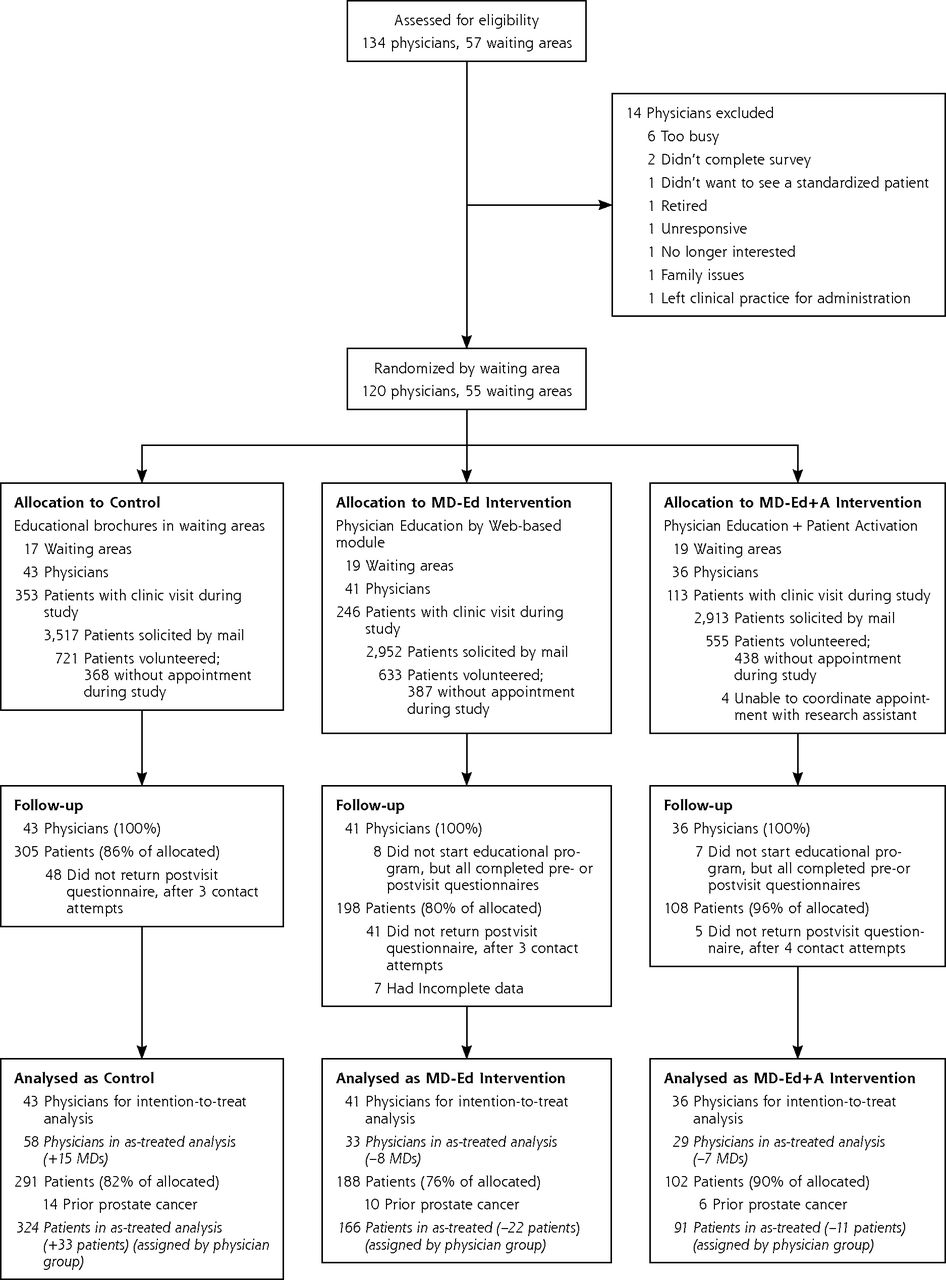
- Figure 2
Subject flow through Men’s Health Decisions study.


Tables
Characteristic Control MD-Ed MD-Ed+A Patients, No. (%)a 291 (50) 188 (32) 102 (16) Sex, male Age, mean (SD), y 63 (7) 63 (7) 64 (7) Ethnicity, %b Hispanic 7 9 8 White 84 79 82 African American 7 10 6 Asian 7 4 2 Other/Hawaiian/American-Indian 5 9 11 Education (%) <High school 2 3 2 High school graduate or GED 10 7 7 Some college or 2-year degree 22 30 35 ≥4-Year college graduate 66 61 56 Marital status, % Divorced/separated/widowed/never married/single 25 23 26 Married/living as married 75 77 74 Employed full or part time, % 44 44 35 Annual household income, % <$30,000 10 13 13 $30,000 to <$75,000 26 27 27 $75,000 to <$100,000 18 18 11 3$100,000 47 42 48 Prior experience with prostate cancer, % Prior screening with PSA test 82 82 86 <1 year ago 57 54 53 1–2 years ago 30 33 26 Family member diagnosed with prostate cancer (brother, father, grandfather) 17 22 16 Close relationship with someone diagnosed with prostate cancer, 41 43 40 Someone close who died of prostate cancer 15 14 12 General health status Overall health status reported, mean (SD)c 3.5 (1) 3.5 (1) 3.5 (1) Poor, % 2 3 3 Fair, % 9 13 13 Good, % 35 28 33 Very good, % 40 43 34 Excellent, % 13 13 18 -
GED=general equivalency degree; MD-Ed=physician education; MD-Ed+A=physician education with patient activation.
-
↵a Patients’ responses for items in this table varied between 91 and 98%.
-
↵b Patients had the opportunity to self-identify more than 1 ethnic group, so sum may exceed 100%.
-
↵c Scored on a range in which 1 = poor, 5 = excellent.
-
Characteristic Control MD-Ed MD-Ed+A Physician demographics Physician, No. (% of group total)a 43 (36) 41 (34) 36 (30) Sex, male, % 69 66 75 Age, mean (SD), y 43 (8) 42 (9) 43 (5) Year finished clinical training, % 1970 to 1994 28 31 34 1995 to 1999 30 28 28 2000 to 2009 43 41 38 Ethnicity, % Asian 23 54 31 White 67 334 60 Practice characteristics Years at current practice site, No. (SD) 8 (5) 7 (6) 9 (6) Total time allocation per week, % (SD) Patient care 86 (14) 85 (17) 83 (18) Administrative activities 10 (10) 14 (16) Teaching, research, or other 8 (7) 10 (13) 9 (8) Patient mix in typical week Patients aged ≥18 y, No. (SD) 113 (103) 77 (44) 105 (103) Patients aged >50 y, mean No. (SD) 28 (12) 29 (14) 31 (11) New patient visits, % (SD) 14 (14) 15 (14) 11 (9) Follow-up visits, % (SD) 62 (16) 63 (18) 69 (15) Urgent/emergency care, % (SD) 22 (13) 20 (12) 18 (13) Inpatient care, % (SD) 4 (6) 3 (6) 3 (4) Prior experiences with prostate cancer Family member with prostate cancer, % 23 12 22 Know anyone diagnosed with prostate cancer, % 40 24 36 Know anyone died of prostate cancer, % 19 15 12 Cared for a patient whose experience changed how physician thought about prostate cancer, % 45 49 33 Male physician >50 y (n = 6), who had PSA testing, % 5 6 4 Overall PSA shared decision making, summed mean score (SD)b 15.9 (1.3) 16.1 (1.6) 16.1 (1.7) PSA shared decision making, mean score (SD)c How often do you offer your patients choices in their medical care? 4.1 (0.5) 4.1 (0.5) 4.1 (0.6) How often do you discuss the pros and cons of each choice with your patients? 3.8 (0.5) 3.8 (0.5) 3.8 (0.6) How often do you ask your patients to state which choice or option they would prefer? 3.8 (0.6) 4.0 (0.5) 3.9 (0.7) How often do you take your patients’ preferences into account when making treatment decisions? 4.1 (0.5) 4.2 (0.6) 4.3 (0.5) Time discussing PSA screening, mean score (SD)d With a typical average risk patient, how much time do you usually spend discussing the risks and benefits of PSA screening? 2.65 (0.6) 2.6 (0.7) 2.4 (0.7) -
MD-Ed = physician education; MD-Ed+A = physician education with patient activation; PSA = prostate-specific antigen.
-
↵a Response rates for these items varied between 97% and 100%.
-
↵b Instrument scale derived from Kaplan.22,23 Scale scores ranged from 5 to 20.
-
↵c Scores ranged from 1 to 5; higher scores indicate more shared decision making.
-
↵d Scores ranged from 1 = never to 4 = in depth.
-
- Table 3
Perceptions of Shared Decision Making Around Prostate Cancer Screening Discussions: Intention-to-Treat Analysis
Perception Control MD-Ed MD-Ed vs Control AMD (95% CI) MD-Ed+A MD-Ed+A vs Control AMD (95% CI) Patient self-report, total patients, No. 291 188 102 Patients who reported discussing PSA screening, No. (%) 111 (38) 78 (41) 0.03 (−0.05 to 0.12) 66 (65) 0.27 (0.14 to 0.40) Overall PSA shared decision making, summed mean score (SD)a 11.8 (3.0) 11.4 (3.0) −0.29 (−1.30 to 0.71) 12.4 (3.0) 0.87 (−0.17 to 1.90) PSA shared decision-making, mean score (SD)b Discussed pros and cons of PSA screening 3.0 (0.7) 2.9 (0.9) −0.09 (−0.36 to 0.19) 3.2 (0.8) 0.26 (−0.02 to 0.54) Offered me choices about whether to get PSA 2.8 (0.8) 2.8 (1.0) −0.01 (−0.31 to 0.27) 3.0(0.9) 0.27 (−0.02 to 0.58) Asked me to state whether I wanted a PSA 2.8 (0.8) 2.8 (1.0) 0.03 (−0.29 to 0.24) 3.0 (0.9) 0.32 (−0.006 to 0.64) Took my preferences into account when deciding 3.1 (0.7) 2.9 (0.9) −0.18 (−0.44 to 0.08) 3.2(0.7) 0.11 (−0.14 to 0.38) Patient values, mean score (SD)c When faced with an important decision about your health, how important is it that you help decide what to do? 6.4 (1.2) 6.5 (0.9) 0.17 (−0.04 to 0.38) 6.4 (1.1) 0.01 (−0.24 to 0.27) How much do you worry about being diagnosed with prostate cancer? 3.0 (1.6) 3.2 (1.7) 0.29 (−0.04 to 0.62) 2.7 (1.4) −0.30 (−0.69 to 0.09) How worried would you be if you knew that you had prostate cancer cells in your body, even if they might not cause any harm? 4.3 (1.8) 4.5 (1.8) 0.23 (−0.11 to −0.56) 3.6 (1.5) −0.70 (−1.10 to −0.30) How much would it bother you to have some difficulty controlling your urine? 5.6 (1.4) 5.7 (1.3) 0.01 (−0.29 to 0.31) 5.2 (1.4) −0.49 (−0.83 to −0.14) How much would it bother you if you could rarely, if ever, get enough of an erection to have sex? 5.7 (1.7) 5.6 (1.6) −0.01 (−0.035 to 0.33) 5.4 (1.7) −0.20 (−0.30 to 0.20) Unannounced standardized patient report, No. of visits 43 41 36 Overall PSA shared decision making, mean score (SD)a 10.0 (3.1) 10.2 (3.0) 0.002 (−1.15 to 1.15) 10.7 (2.7) 0.32 (−0.90 to 1.54) PSA shared decision-making, mean score (SD)b Discussed pros and cons of PSA screening 3.0 (0.9) 3.1 (0.9) 0.11 (−0.26 to 0.47) 3.2 (0.8) 0.18 (−0.21 to 0.57) Offered me choices about whether to get PSA 2.7 (1.1) 2.7 (1.1) −0.06 (−0.60 to 0.47) 3.0 (0.9) 0.25 (−0.30 to 0.80) Asked me to state whether I wanted a PSA 2.1 (1.0) 2.0 (0.9) −0.18 (−0.59 to 0.24) 2.3 (0.8) −0.02 (−0.45 to 0.41) Took my preferences into account when deciding 2.3 (1.0) 2.4 (1.0) 0.12 (−0.24 to 0.49) 2.4 (0.9) −0.01 (−0.40 to 0.38) Pre-post change in shared deicision making, by physician self-report, No. of physiciansd 43 41 36 Change in shared decision making, summed mean score (SD)e 0.2 (1.5) 0.2 (1.5) −0.05 (−0.72 to 0.61) 0.1 (1.5) −0.10 (−0.77 to 0.56) Physician shared decision making, mean score (SD) How often do you offer your patients choices in their medical care? 0.1 (0.6) 0.1 (0.6) 0.07 (−0.18 to 0.33) −0.03 (0.6) −0.11 (−0.37 to 0.15) How often do you discuss the pros and cons of each choice with your patients? 0.2 (0.7) 0.0 (0.6) −0.21 (−0.49 to 0.07) 0.2 (0.5) 0.07 (−0.21 to 0.35) How often do you ask your patients to state which choice or option they would prefer? 0.0 (0.7) 0.0 (0.6) −0.02 (−0.34 to 0.30) 0.0 (0.7) −0.01 (−0.33 to 0.30) How often do you take your patients’ preferences into account when making treatment decisions? 0.0 (0.6) 0.0 (0.6) 0.09 (−0.20 to 0.38) −0.1 (0.7) −0.05 (−0.35 to 0.24) Pre-post change in physician self-reported scores, mean (SD)d With a typical average-risk patient, how much time do you usually spend discussing the risks and benefits of PSA screening? 0.1 (0.7) 0.3 (0.6) 0.18 (−0.13 to 0.49) 0.6 (0.7) 0.46 (0.15 to 0.78) -
AMD= adjusted mean difference; MD-Ed = physician education; MD-Ed+A = physician education with patient activation; PSA = prostate-specific antigen. Notes: Between-arm contrasts estimated in mixed-effects models for clustered data, with statistical adjustments for health system site.
-
↵a Instrument scale derived from Kaplan. Scale scores ranged from 4 = strongly disagree to 16 = strongly agree.
-
↵b Item scores ranged from 1 = strongly disagree to 4 = strongly agree.
-
↵c Item scores ranged from 1 = not at all to 7 = a great deal.
-
↵d Preintervention to postintervention change. Scale scores ranged from 1 = never to 5 = in depth.
-
↵e Instrument scale derived from Kaplan.
-
- Table 4
Characteristics of Clinic Visits With Study Physician, as Reported by Patients and Unannounced Standardized Patients: Intention-to-Treat Analysis
Characteristic Control MD-Ed MD-Ed vs Control AMD (95% CI) MD-Ed+A MD-Ed+A vs Control AMD (95% CI) Clinic visits by patients, No. 291 188 102 Discussed prostate cancer screening, % 38 41 0.03 (−0.05 to 0.12) 65 0.27 (0.14 to 0.40) Time spent with physician, % <10 min 19 24 0.06 (−0.01 to 0.13) 15 −0.02 (−0.10 to 0.05) 10–20 min 59 55 −0.04 (−0.16 to 0.07) 54 −0.05 (−0.17 to 0.06) >21–30 min 22 21 −0.02 (−0.11 to 0.06) 31 0.07 (−0.04 to 0.18) Discussed health prevention (exercise, nutrition, screening tests, etc), % 74 74 0.01 (−.007 to 0.10) 79 −0.04 (−0.13 to 0.05) Doctor addressed main concern during this visit, % 100 100 −0.05 (−0.10 to 0.003) 100 −0.02 (−0.06 to 0.09) Satisfaction with this visit, No. (SD)b 18 (3) 18 (2) 0.04 (−0.54 to 0.61) 18 (3) 0.22 (−0.45 to 0.88) Clinic visits by unannounced standardized patients, No. 43 41 36 Physician engaged in discussion on PSA, % 19 33 0.16 (−0.04 to 0.37) 32 0.032 (−0.10 to 0.54) Physician elicited preference for PSA test, mean score (SD)c 2.3 2.4 0.12 (−0.24 to 0.49) 2.4 −0.01 (−0.40 to 0.38) Doctor neither suggested nor recommended for or against PSA test, % 15 33 0.16 (−0.05 to 0.37) 50 0.32 (0.10–0.54) -
AMD = adjusted mean difference; MD-Ed = physician education; MD-Ed+A = physician education with patient activation; PSA = prostate-specific antigen Note: Between-arm contrasts in outcome means estimated in mixed-effects models for clustered data, with statistical adjustments for health system site.
-
a Percentage yes vs no or don’t know.
-
↵b Sum of 5 satisfaction items, ranging from 5 = least satisfied to 20 = most satisfied.
-
↵c Scored on a range from 1 to 5, where 1 = strongly agree and 5 = strongly disagree.
-
The Article in Brief
Pairing Physician Education With Patient Activation to Improve Shared Decisions in Prostate Cancer Screening: A Cluster Randomized Controlled Trial
Michael S. Wilkes , and colleagues
Background Because of controversies surrouding prostate cancer screening, most expert groups recommend shared decision making between patient and doctor. This study tests whether educating primary care physicians and "activating" their patients has a synergistic effect on (1) perceived shared decision making, (2) rates of prostate cancer screening discussion, and (3) final physician prostate cancer screening recommendations.
What This Study Found Pairing a brief 20- to 30-minute Web-based educational intervention for physicians with a companion intervention for patients about counseling for prostate cancer screening appears to improve shared decision making rates and influence physicians' attitudes about screening. Prostate cancer screening discussion rates are higher among patients who receive the combination of physician education and patient activation compared with physician education alone or usual education. Standardized patients (actors trained to simulate real patient cases and later report on the encounter) also report that physicians seeing patients who receive the combined intervention are more likely to be neutral in their final recommendations about whether the patient should obtain a prostate-specific antigen blood test This shift in physicians' attitudes from a pro-screening bias to neutral counseling persists 3 months after the intervention. There is no difference in patients' ratings of shared decision making between the groups.
Implications
- Coupling physician education with patient activation, the authors conclude, has the potential to encourage shared decision making around issues of medical uncertainty, such as prostate cancer screening, and improve the appropriate utilization of medical services.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Patient Communication Preferences for Prostate Cancer Screening Discussions: A Scoping Review
- Teaching clinicians shared decision making and risk communication online: an evaluation study
- Strategies to evaluate healthcare provider trainings in shared decision-making (SDM): a systematic review of evaluation studies
- The Effect of Anal Dysplasia and Cancer Screening Education on Attitudes, Beliefs, and Self-Efficacy
- Training primary care physicians to offer their patients faecal occult blood testing and colonoscopy for colorectal cancer screening on an equal basis: a pilot intervention with before-after and parallel group surveys
- Shared Decision Making, Contextualized
- In This Issue: A Diversified Portfolio