
Article Figures & Data
Figures
- Figure 1
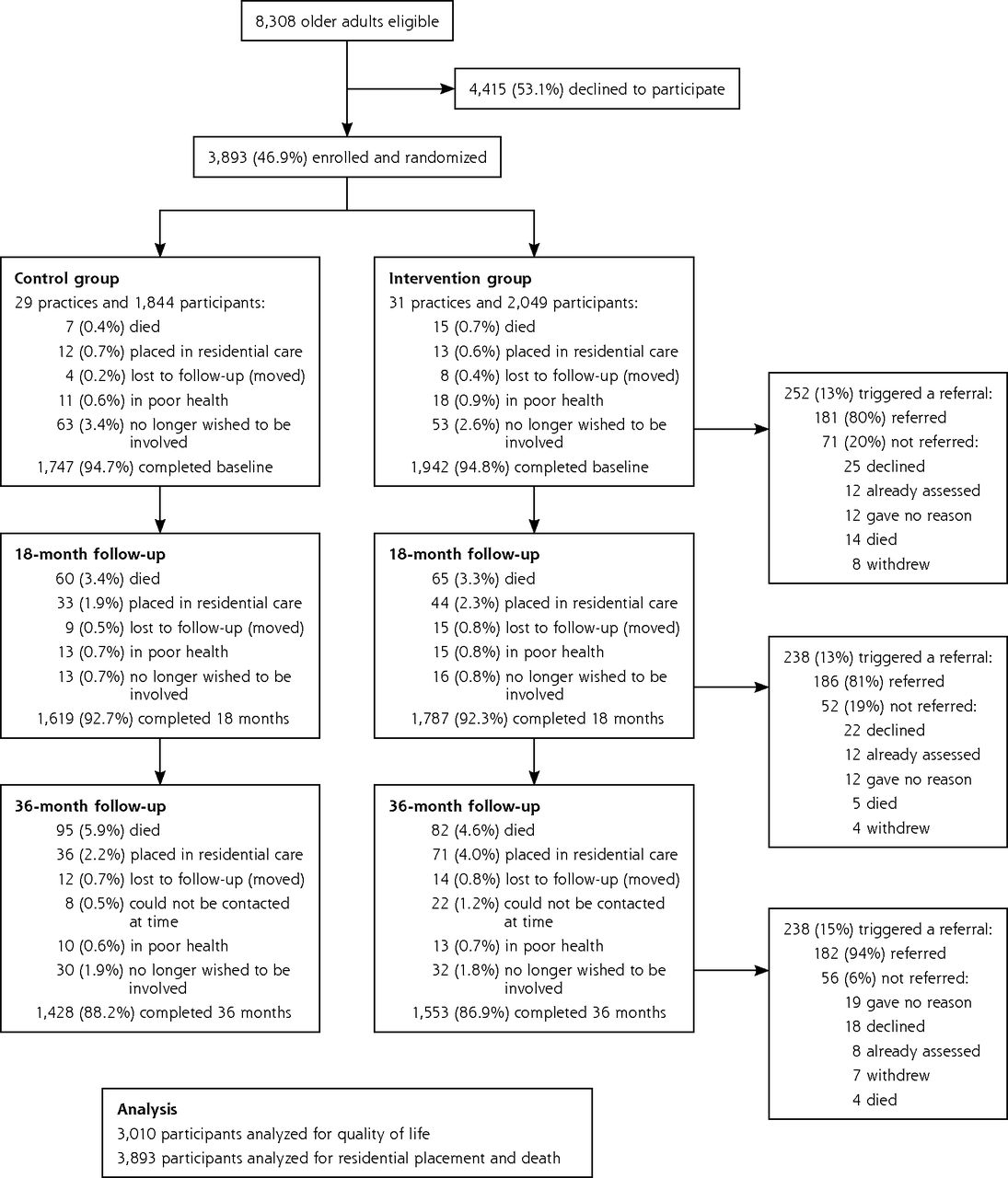
Flow of patients through the BRIGHT trial and numbers triggering referral and referred.
Note: Referral for assessment and services was triggered by a Brief Risk Identification Geriatric Health Tool (BRIGHT) score of 3 or higher.
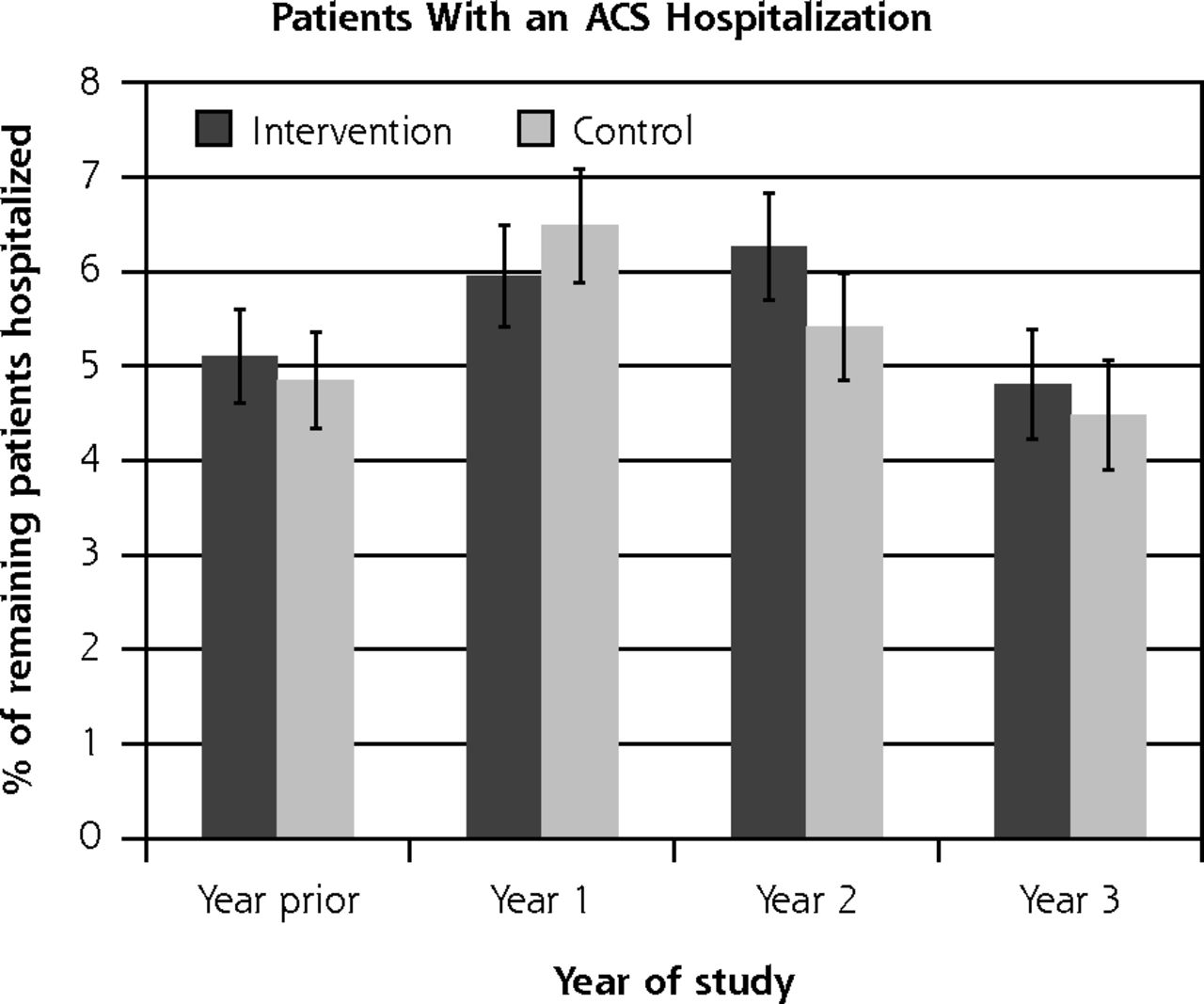
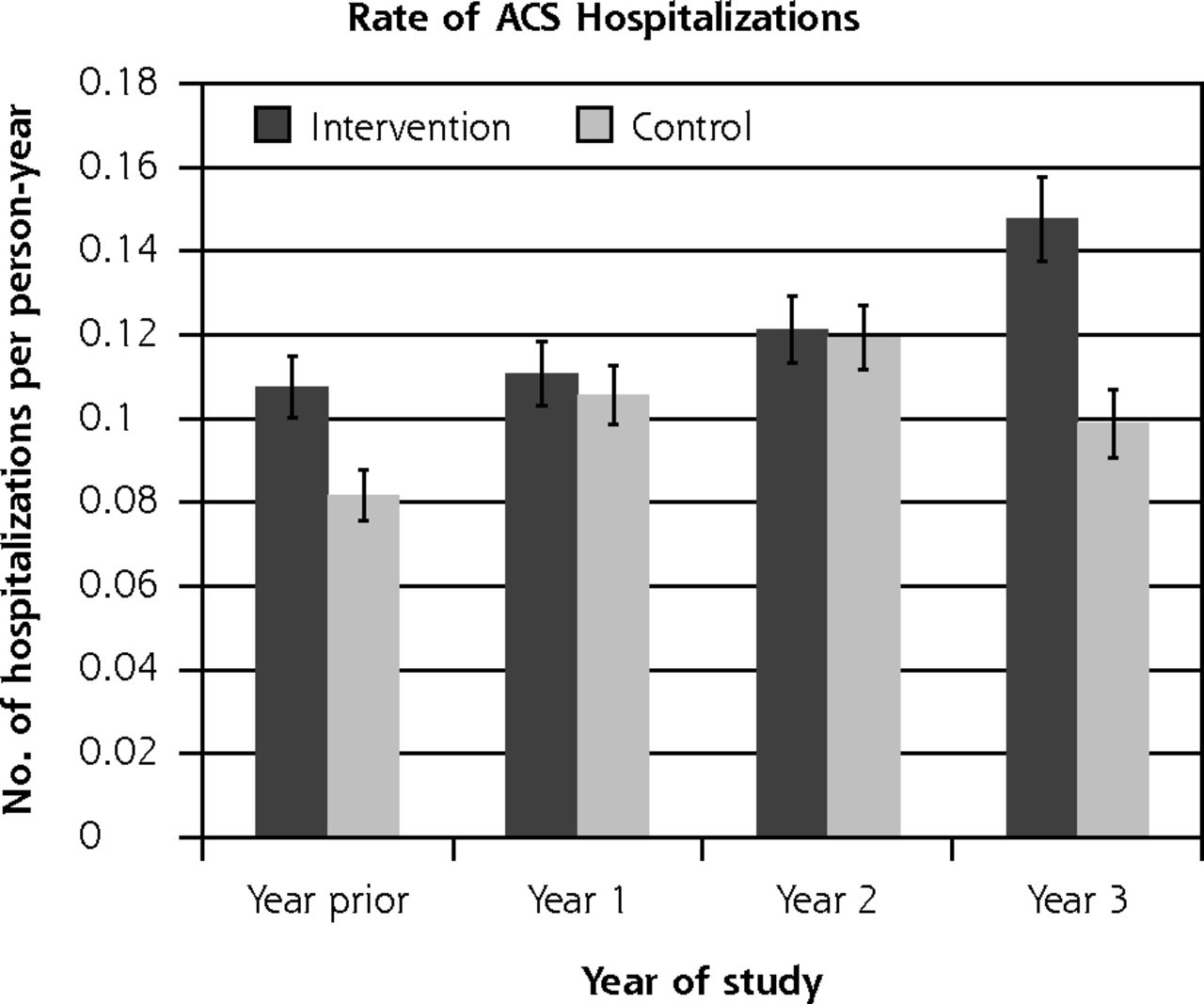
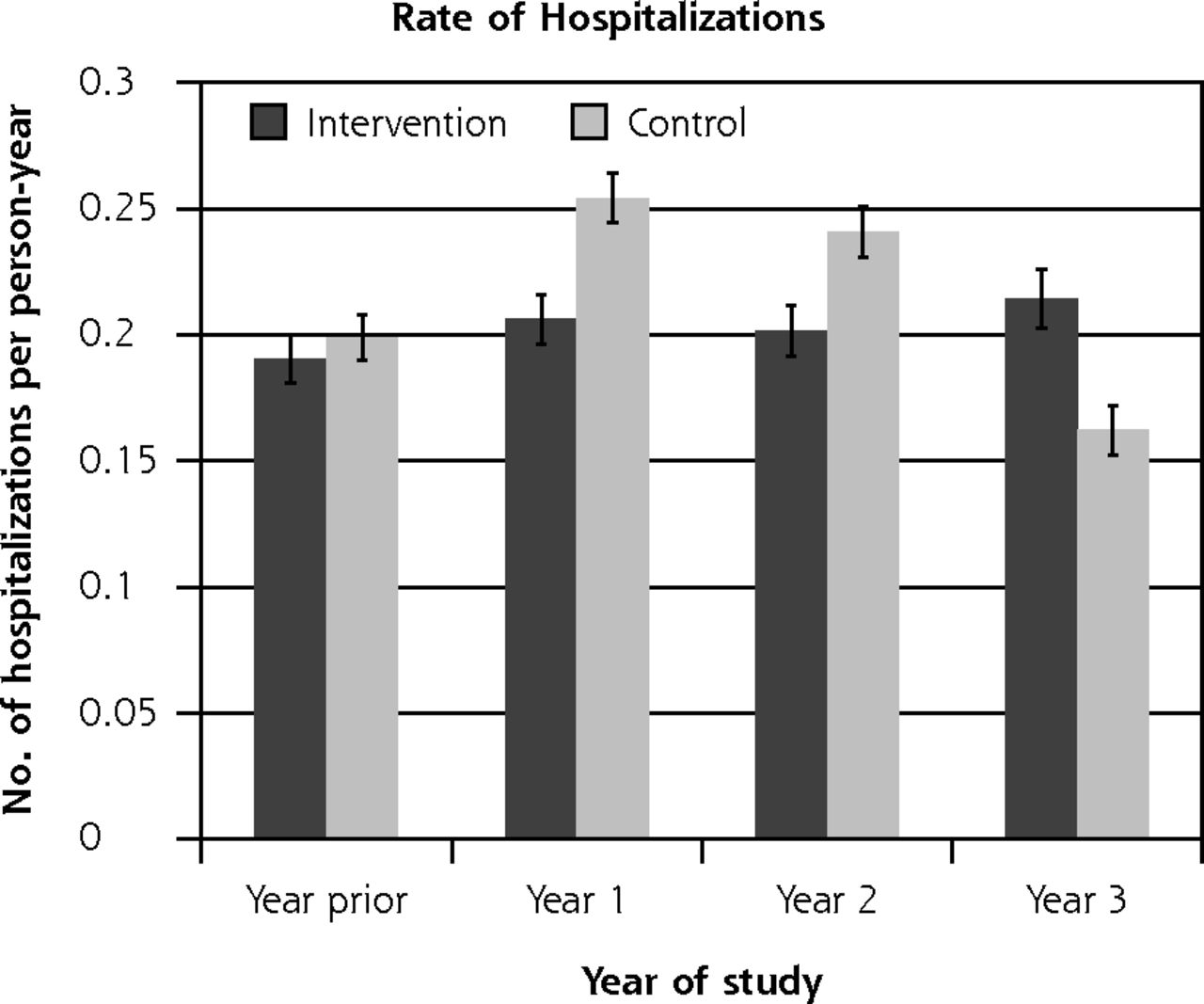
- Figure 2
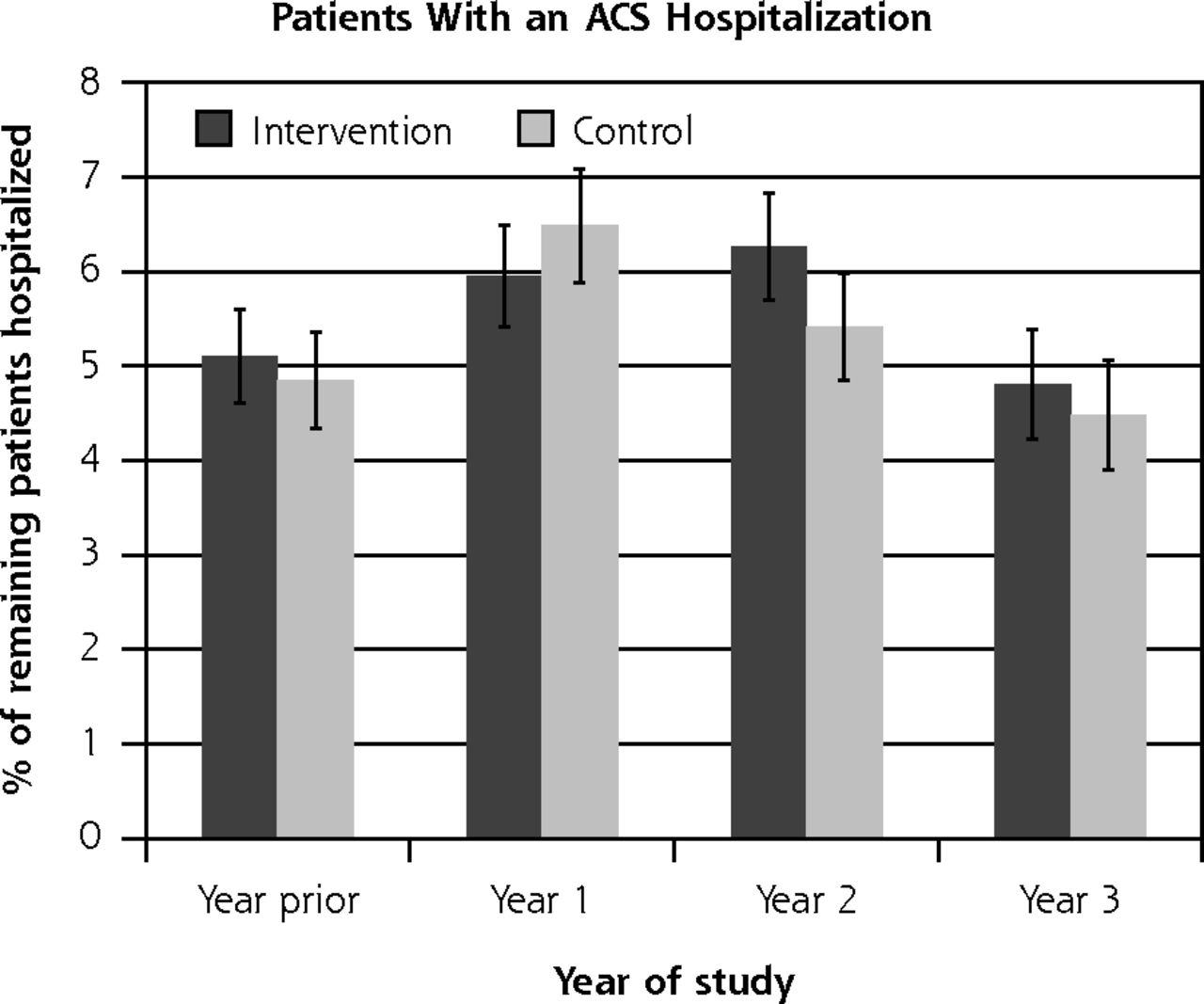
Ambulatory care–sensitive hospitalizations and overall hospitalizations, by study group.
ACS = ambulatory care sensitive (hospitalizations resulting from diseases sensitive to good primary health care setting).
Notes: Hospitalizations were ascertained by matching encrypted National Health Identification (NHI) number, a unique identifier, with centrally held records of all hospital admissions from the New Zealand Ministry of Health27,28 at the end of the trial. International Classification of Diseases codes can be found and are used frequently in New Zealand.17 There was no significant difference between groups in the percentage of patients with an ACS hospitalization (P = .82 binomial mixed model regression, controlled for prior hospitalization and clustering) and rate of ACS hospitalizations (P = .88 Poisson mixed model regression, controlled for number of prior hospitalizations and clustering), or in the percentage of patients with any hospitalization (P = .88 binomial mixed model regression, controlled for prior hospitalization and clustering) and rate of any hospitalization (P = .68 Poisson mixed model regression, controlled for number of prior hospitalizations and clustering).
- Figure 3
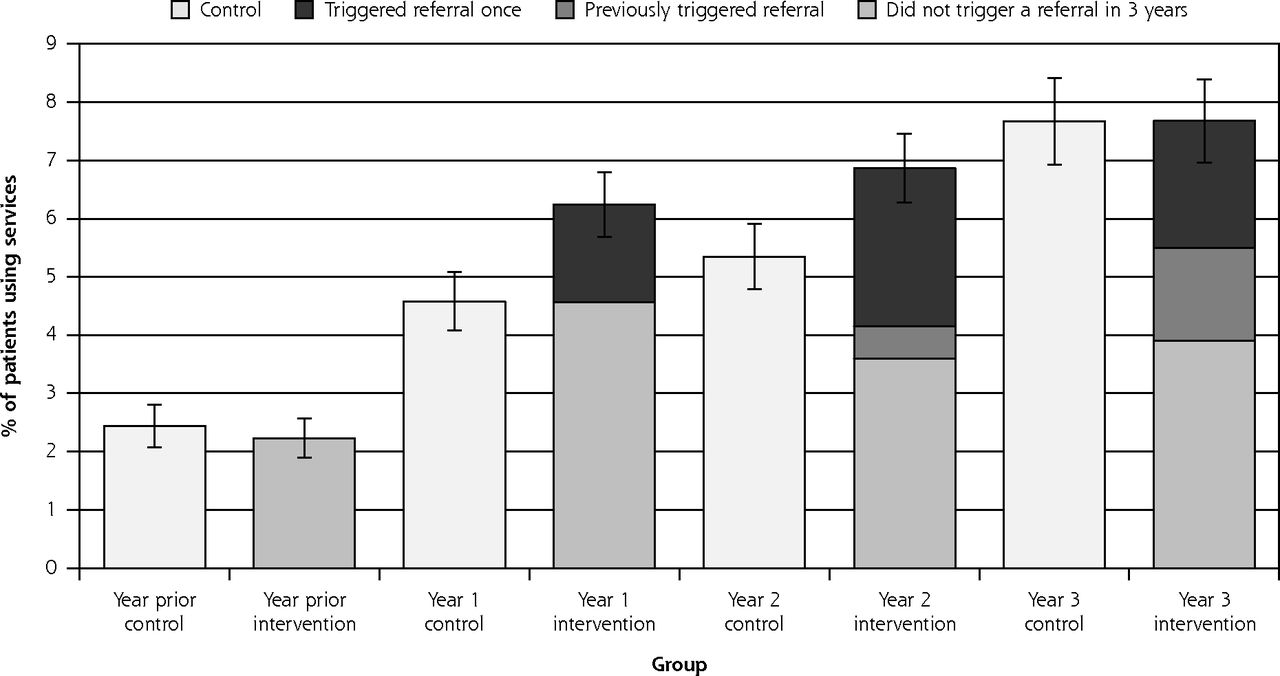
Use of geriatric assessment and rehabilitation community services.
Notes: There was no significant difference between intervention and control groups over time in the percentages of patients who had a geriatric assessment and/or used rehabilitation community services during the trial (P = .09). Figure shows all outpatient geriatric assessment and rehabilitation services used, including comprehensive assessment, physiotherapy, occupational therapy, social work, gerontology nursing, and case management by group. Shown for the intervention group are patients for whom Brief Risk Identification Geriatric Health Tool (BRIGHT) scores triggered referral once (darkest section of bar), had triggered previously (dark section of bar), and did not trigger during the 3 years (lighter section of intervention bars). Lightest bar is the control group.
- Figure 4
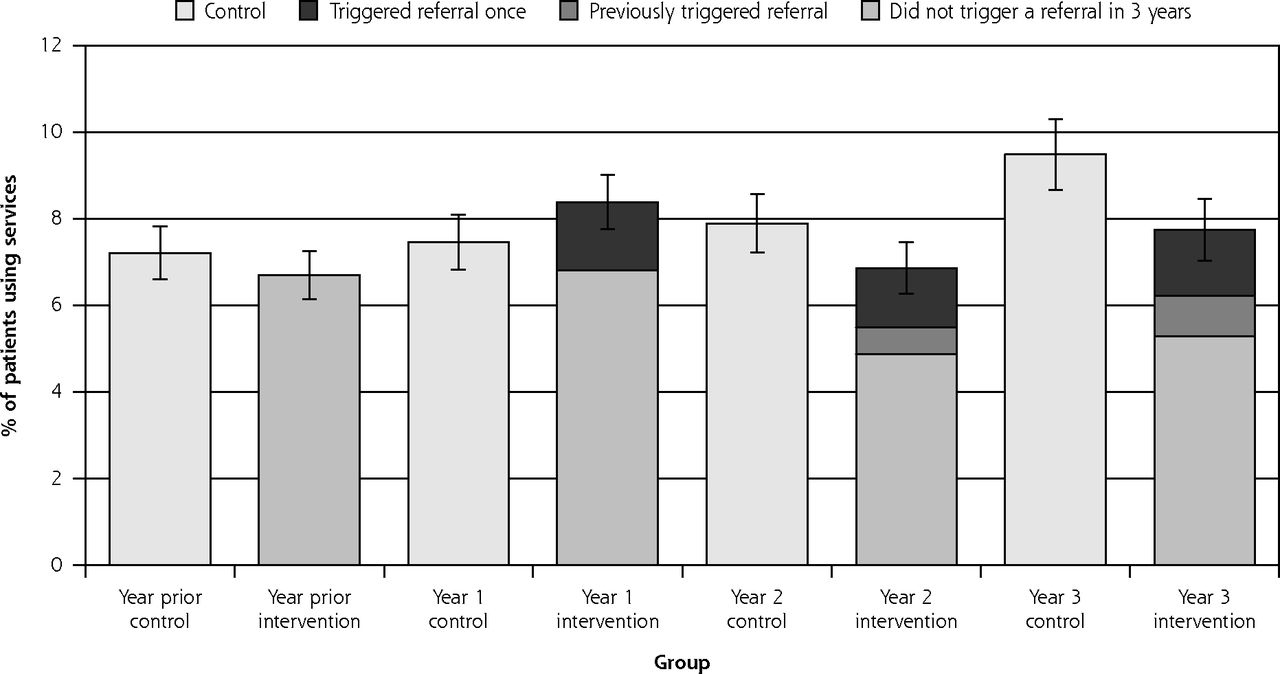
Use of emergency departments.
Notes: There was no significant difference between intervention and control groups over time in emergency department use during the trial (P = .27). Shown for the intervention group are patients for whom Brief Risk Identification Geriatric Health Tool (BRIGHT) scores triggered referral once (darkest section of bar), had triggered previously (dark section of bar), and did not trigger during the 3 years (lighter section of intervention bars). Lightest bar is the control group.




Tables
Characteristic Na Intervention Mean (SD) or No. (%) Control Mean (SD) or No. (%) P Value Total Mean (SD) or No. (%) Demographics Age, mean (SD), y 3,753 80.4 (4.6) 80.3 (4.5) .53 80.3 (4.6) Sex, female, No. (%) 3,737 1,101 (56) 951 (54) .21 2,052 (55) Married, No. (%) 3,711 1,038 (53) 945 (54) .66 1,983 (53) Living alone, No. (%) 3,738 824 (42) 724 (41) .57 1,548 (41) Education, No. (%) 3,598 .64 Primary school 270 (14) 251 (15) 521 (14) Secondary school 882 (47) 763 (45) 1,645 (46) Tertiary qualification 739 (39) 693 (41) 1,432 (40) Main lifetime occupation, No. (%) 3,706 .97 Professional 681 (35) 639 (36) 1,320 (36) Managerial/technical 935 (48) 793 (45) 1,728 (47) Clerical/laborers 332 (17) 326 (19) 658 (18) Clinical characteristics Total medications, mean (SD) 2,849 4.29 (3.24) 4.10 (3.11) .01 4.20 (3.18) Hospitalized in last 12 mo, No. (%) 3,752 158 (8) 152 (9) .52 310 (8) Diagnoses, No. (%)b Hypertension 3,551 1,054 (57) 930 (55) .22 1,984 (56) Myocardial infarction 3,478 497 (27) 459 (28) .97 956 (27) Cerebrovascular accident 3,416 213 (12) 172 (11) .18 385 (11) COPD 3,441 126 (7) 124 (7) .65 250 (7) Total No., mean (SD)c 3,524 0.46 (0.66) 0.46 (0.62) .72 0.45 (0.64) Smoking, No. (%) 3,720 .57 Never smoker 905 (46) 804 (46) 1,709 (46) Past smoker 1,002 (51) 896 (51) 1,898 (51) Current smoker 54 (3) 59 (3) 113 (3) Fell in last 12 mo, No. (%) 3,721 622 (32) 576 (33) .47 1,198 (32) Support services, No. (%) Any home help 3,727 589 (30) 445 (25) .01 1,034 (28) Home help more than once a week 1,027 99 (17) 38 (9) <.001 137 (13) Any personal care 3,727 92 (5) 49 (3) .002 141 (4) Personal care more than once a week 139 83 (92) 46 (94) .72 129 (93) Cognition, AMTS score, mean (SD) 3,714 9.31 (1.02) 9.4 (0.89) <.001 9.35 (0.96) Depression, GDS-15 score ≥5, No. (%) 3,726 184 (9) 158 (9) .66 342 (9) Disabled subgroup Sex, female, No. (%) 148 58 (61) 30 (57) .63 88 (59) Age, mean (SD), y 148 80.0 (5.2) 81.5 (5.5) .12 8.5 (5.3) SPPB score, mean (SD) 148 5.6 (3.2) 6.0 (3.4) .60 5.7 (3.3) Grip strength, mean (SD), kg 144 23.0 (9.4) 24.0 (11.2) .09 23.3 (10.0) -
AMTS = Abbreviated Mental Test Score (higher score indicates better cognition; score of ≥7 is considered normal); COPD = chronic obstructive pulmonary disease; GDS-15 = 15-item Geriatric Depression Scale (higher score indicates more depressive symptoms; score of ≥5 is considered moderate depressive symptoms); SPPB = Short Physical Performance Battery for physical function (measures physical performance, a combination of balance, gait speed, and chair stands; scores range from 0 to 12; a higher score indicates better function).
-
↵a Total with complete data included in analysis.
-
↵b Ascertained by the question “Have you ever been told by a doctor that you have or have had: high blood pressure, asthma, diabetes, arthritis/rheumatism, epilepsy, Parkinson’s disease, osteoporosis, heart attack or angina, stroke, chronic bronchitis or emphysema, hip fracture, knee replacement, hip replacement, depression, or mental illness?”
-
↵c Excluding hypertension.
-
Outcome Na Time point, mo Intervention Mean (SD) or No. (%) Control Mean (SD) or No. (%) P Valueb Function, NEADL score, mean (SD) 3,190 0 19.6 (2.4) 19.8 (2.1) .13 18 19.4 (2.8) 19.4 (2.7) 36 19.4 (3.0) 19.3 (3.0) WHOQOL-BREF scores, mean (SD) Physical 3,741 0 70.4 (16.4) 71.4 (16.3) .007 3,410 18 70.3 (16.8) 70.5 (17.0) 3,010 36 70.5 (15.8) 70.0 (15.7) Psychological 3,732 0 73.0 (11.8) 73.7 (12.0) .005 3,407 18 72.5 (12.5) 72.9 (12.4) 3,010 36 72.7 (12.5) 72.1 (12.2) Social 3,729 0 79.0 (13.4) 79.6 (13.3) .13 3,401 18 79.6 (13.0) 79.3 (13.3) 3,005 36 79.3 (11.9) 79.3 (12.2) Environmentalc 3,742 0 80.2 (11.2) 80.3 (11.4) .20 3,411 18 80.7 (11.5) 80.2 (11.8) 3,010 36 80.6 (10.7) 80.3 (11.0) AM-PAC scores, mean (SD) Physical and movement 2,118 0 64.7 (6.7) 65.1 (6.9) .03 18 64.1 (7.1) 64.2 (7.1) 36 62.9 (6.9) 62.8 (9.7) Personal care instrumental 2,117 0 60.5 (8.6) 60.8 (8.9) .42 18 59.8 (8.8) 59.6 (9.1) 36 60.6 (9.4) 60.6 (9.3) Depression, GDS-15 score, mean (SD) 3,187 0 1.8 (1.8) 1.7 (1.9) .053 18 1.9 (2.0) 2.0 (2.1) 36 2.0 (2.1) 2.1 (2.1) Satisfaction with your last consultation with the primary care physician, No. (%) “Involves you,”d very good/excellent 3,128 0 1,294 (85.8) 1,217 (86.0) .21 18 1,317 (82.6) 1,182 (78.2) 36 1,225 (76.2) 1,126 (74.1) “Time spent,”e very good/excellent 3,145 0 1,232 (79.2) 1,199 (81.4) .11 18 1,209 (75.5) 1,105 (72.6) 36 1,119 (69.4) 1,026 (67.0) “Care and concern,”f very good/excellent 3,137 0 1,350 (85.9) 1,262 (85.7) .16 18 1,332 (83.3) 1,184 (77.9) 36 1,260 (78.2) 1,149 (75.3) Support services, No. (%) Any home help 3,727 0 589 (30) 445 (25) .80 3,406 18 538 (30) 426 (26) 3,011 36 627 (40) 502 (35) Home help more than once a week 1,025 0 99 (17) 38 (9) <.01 960 18 80 (15) 51 (12) 1,128 36 85 (14) 54 (11) Any personal care 3,727 0 92 (5) 49 (3) .23 3,405 18 102 (6) 79 (5) 3,011 36 104 (7) 80 (6) Personal care more than once a week 139 0 83 (92) 46 (94) <.01 177 18 89 (89) 70 (91) 184 36 94 (90) 73 (91) Disabled subgroup SPPB score, mean (SD) 149 0 5.6 (3.2) 6.0 (3.4) .28 112 18 7.0 (3.2) 6.9 (3.0) 78 36 7.1 (3.0) 8.3 (2.2) Grip strength, mean (SD), kg 144 0 23.0 (9.4) 24.0 (11.2) .07 122 18 22.9 (9.5) 24.8 (11.4) 89 36 23.2 (8.9) 24.5 (11.5) 30-m walk distance, mean (SD), m 93 0 32.2 (28.3) 26.5 (8.2) .051 74 18 35.1 (35.3) 42.4 (64.6) 60 36 33.6 (17.5) 27.1 (6.4) 3-m gait speed, mean (SD), m/sec 138 0 5.8 (5.1) 4.7 (2.6) .04 123 18 5.0 (3.3) 5.2 (4.1) 89 36 5.0 (3.5) 3.8 (1.9) -
AM-PAC = Activity Measure for Post-Acute Care (measures functional ability, a higher score indicates better function); GDS-15 = 15-item Geriatric Depression Scale (higher score indicates more depressive symptoms and a score of ≥5 is considered moderate depressive symptoms); NEADL = Nottingham Extended Activities of Daily Living Scale (score ranges from 0 to 22; higher score indicates greater independence); SPPB = Short Physical Performance Battery (measures physical performance, a combination of balance, gait speed, and chair stands; scores range from 0 to 12; a higher score indicates better function); WHOQOL-BREF = abbreviated version of the World Health Organization Quality of Life Scale (scores range from 1 to 100; a higher score means better QOL).
-
↵a Total with complete data included in analysis.
-
↵b Result of generalized regression models with repeated measures adjusted for clustering by practice and region, and applies to the change over the 3 time points.
-
↵c Domain of the WHOQOL-BREF (maximum score is 100; higher score indicates better quality of life).
-
↵d Ascertained by asking “[How satisfied are you with] how much the doctor involves you in decisions about your care?”
-
↵e Ascertained by asking “[How satisfied are you with] the amount of time your doctor spends with you?”
-
↵f Ascertained by asking “[How satisfied are you with] the doctor’s care and concern for you?”
-
Supplemental Appendixes 1-2
BRIGHT SCREEN (Brief Risk Identification for Geriatric Health Tool)
Files in this Data Supplement:
- Supplemental data: Appendixes 1-2 - PDF file; 2 pages + cover
In Brief
The Cluster-Randomized BRIGHT Trial: Proactive Case Finding for Community-Dwelling Older Adults
Ngaire Kerse , and colleagues
Background Researchers in New Zealand assessed the effectiveness of a case finding strategy, which uses a screening survey?the Brief Risk Identification Geriatric Health Tool (BRIGHT)?to identify older adults with disability and refer them to geriatric services if necessary, as the first in a two-step process aimed at reducing disability and improving outcomes among older patients.
What This Study Found The BRIGHT screening intervention successfully identified older adults in need and increased residential care placement, but did not reduce the use of acute hospital services. After 36 months, patients in the intervention group who used the annual screening tool were more likely than those in the control group to have been placed in residential care. In addition, intervention patients had smaller declines in average scores for physical health-related quality of life and psychological health-related quality of life. Hospitalization, disability, and use of services, however, did not differ between groups.
Implications
- The case-finding strategy was effective in increasing identification of older adults with disability, but there was little evidence of improved outcomes.
- The authors call for further research to test primary care integration strategies.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preventive interventions to improve older peoples health outcomes: systematic review and meta-analysis
- Community based complex interventions to sustain independence in older people: systematic review and network meta-analysis
- Primary Care Variation in Rates of Unplanned Hospitalizations, Functional Ability, and Quality of Life of Older People
- In This Issue: Research Briefs and New Clinical and Policy Insights