
Abstract
PURPOSE Multimorbidity is associated with adverse outcomes, yet research on the determinants of its incidence is lacking. We investigated which sociodemographic, health, and individual lifestyle (eg, physical activity, smoking behavior, body mass index) characteristics predict new cases of multimorbidity.
METHODS We used data from 4,564 participants aged 50 years and older in the English Longitudinal Study of Aging that included a 10-year follow-up period. Discrete time-to-event (complementary log-log) models were constructed for exploring the associations of baseline characteristics with outcomes between 2002-2003 and 2012-2013 separately for participants with no initial conditions (n = 1,377) developing multimorbidity, any increase in conditions within 10 years regardless of initial conditions, and the impact of individual conditions on incident multimorbidity.
RESULTS The risks of developing multimorbidity were positively associated with age, and they were greater for the least wealthy, for participants who were obese, and for those who reported the lowest levels of physical activity or an external locus of control (believing that life events are outside of one’s control) for all groups regardless of baseline conditions (all linear trends <.05). No significant associations were observed for sex, educational attainment, or social detachment. For participants with any increase in conditions (n = 4,564), a history of smoking was the only additional predictor. For participants with a single baseline condition (n = 1,534), chronic obstructive pulmonary disease (COPD), asthma, and arrhythmia showed the strongest associations with subsequent multimorbidity.
CONCLUSIONS Our findings support the development and implementation of a strategy targeting the prevention of multimorbidity for susceptible groups. This approach should incorporate behavior change addressing lifestyle factors and target health-related locus of control.
INTRODUCTION
The rising tide of multimorbidity (2 or more concurrent conditions)1 is a major challenge facing health care systems worldwide.2–4 Multimorbidity is associated with significant reductions in functional status and quality of life,5,6 increased risk of premature death,7 and substantially increased use of health service care.8,9 A number of interventions have been developed and evaluated for improving health and health care outcomes of persons with prevalent multimorbidity, although uncertainties remain about their effectiveness.10,11
An alternative strategy would be preventing the development of multimorbidity,12 which could be achieved through better implementation of multiple existing, condition-specific, preventive strategies.4,13–15 It may be possible, however, to develop more efficient strategies addressing common determinants of multimorbidity across a wide range of conditions. Ascertaining the key determinants of multimorbidity is an essential prerequisite for developing our knowledge of the pathogenesis of multimorbidity, for the early identification of individuals at risk, and for informing effective public health and health care–oriented strategies.12
Consistent associations have been found, mostly in cross-sectional studies,16 between multimorbidity and older age, lower socioeconomic status, and mental health problems, and less consistently with the female sex.4,8,13,17–19 Large gaps remain in our knowledge regarding determinants of multimorbidity, however. Longitudinal investigations are needed to confirm observations from cross-sectional studies and to explore lifestyle predictors, as well as sociodemographic factors.16,20,21 A recent systematic review also highlighted the lack of studies investigating the impact of specific conditions with the development of multimorbidity.16,22
We sought to help redress these gaps in the current understanding through the present study. Our goal was to use longitudinal data to investigate which sociodemographic, health, and lifestyle characteristics (eg, physical activity, smoking behavior, body mass index [BMI]) were predictive of incident conditions during a 10-year period. We explored factors associated with time to subsequent multimorbidity for participants with no conditions at baseline, and with time to any increase in conditions for all participants, regardless of baseline morbidity, as well as the impact of individual conditions.
METHODS
Study Design and Data Source
The English Longitudinal Study of Aging (ELSA) cohort was selected to be representative of adults aged 50 years and older living in private households in England.23 ELSA collects information from participants through face-to-face interviews every 2 years (baseline in 2002-2003), with an additional nurse visit at every 2-year wave. Detailed descriptions of the sampling and data collection methods are published elsewhere.23–26 We included participants who were interviewed in all 6 consecutive waves of ELSA from 2002-2003 to 2012-2013.
Multimorbidity
At each wave, participants self-reported whether a physician had diagnosed any of the following 15 conditions included in ELSA (excluding eye conditions, which are not typically included in measures of multimorbidity): hypertension, ischemic heart disease (angina or myocardial infarction), congestive heart failure, heart arrhythmia, diabetes mellitus, stroke, chronic obstructive pulmonary disease, asthma, arthritis (any), osteoporosis, cancer (any), Parkinson’s disease, 1 or more affective mental health conditions (depression, anxiety, or emotional problems), 1 or more psychotic mental health conditions (schizophrenia, psychosis, bipolar disorder, or hallucinations), and dementia (including Alzheimer’s disease). For an affective mental health condition, we ascertained at each follow-up whether the condition(s) was in remission. At each wave, variables were created for the number of conditions reported by participants, whether they had multimorbidity (2 or more conditions), and whether they reported an increased number of conditions since the previous wave.
Participant Characteristics
We obtained information from 2002-2003 on participants’ age (5-year groups), sex, total wealth (converted to quintiles), education level (higher, intermediate [secondary/high school], no qualifications), BMI category (assessed at the 2004-2005 nurse visit), smoking behavior (never, past, current), physical activity (Allied Dunbar fitness survey: high, moderate, low/sedentary),27 social detachment,28 whether they live alone, and locus of control (the extent to which they believe life events are outside their control). Details on the derivation of covariates are provided in the Supplement Appendix, available at http://www.AnnFamMed.org/content/16/4/322/suppl/DC1/.
Statistical Analysis
We present trends in multimorbidity and individual conditions across the 10-year study and the patterns of co-occurring conditions in 2012-2013 with relative risks.
We constructed 3 discrete time-to-event complementary log-log models (equivalent to Cox proportional hazards models for continuous time) to explore the associations of baseline characteristics with acquiring incident conditions between 2002-2003 and 2012-2013 (a nonparametric specification of the baseline hazard was used). The first model included individuals with no initial conditions and used having 2 or more incident conditions (multimorbidity) as the outcome. The second included all participants, regardless of baseline morbidity, with 1 or more incident conditions as the outcome. Ordinal variables were entered as dummy variables to investigate any threshold effects in their categories and as continuous variables to test for linear trends. The final model was constructed with individual conditions in 2002-2003 as predictors, included participants with 1 initial condition only, and used 1 or more incident conditions (and therefore multimorbidity) as the outcome. This model controlled for baseline characteristics.
Longitudinal sample weighting was used to account for differential nonresponse, the details of which are provided in the ELSA technical report.23 Multiple imputation of missing data was used throughout. All analyses were conducted using Stata\SE v15.1 (Stata Corp).
RESULTS
A total of 12,100 participants completed the baseline interview, of whom 4,564 (37.7%) completed all 5 subsequent 2-year waves and were included in our analyses. The characteristics of this sample are displayed in Table 1. The prevalence of multimorbidity and individual conditions across the study period is shown in Table 2. The mean follow-up period was 10.14 years (SD = 0.26 years). Of the 1,477 participants with no initial conditions, 377 (25.5%) developed incident multimorbidity, and 901 (61.0%) reported 1 or more incident conditions. Similarly, 1,001 of 1,534 (65.3%) participants with a single condition in 2002-2003 reported 1 or more new conditions (and therefore incident multimorbidity) within 10 years.
Participants’ Characteristics at Baseline (2002-2003) and Outcomes at End of Study (2012-2013)
Prevalence of Multimorbidity and Individual Conditions From 2002-2003 to 2012-2013 in the Full Sample (N = 4,564)
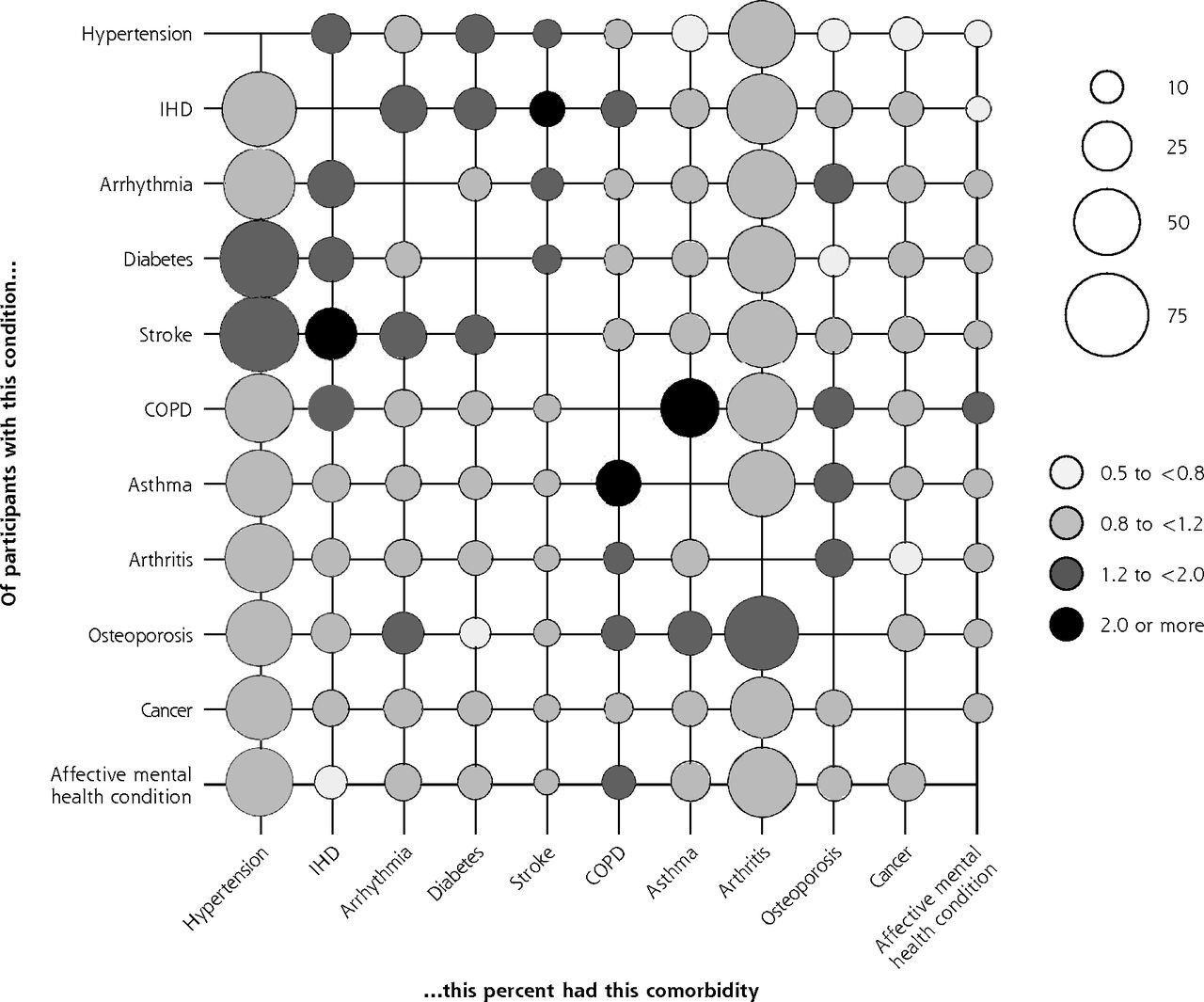
Hypertension and arthritis were the most prevalent and the most commonly comorbid conditions in 2012-2013 (Figure 1). The overall prevalence of multimorbidity in 2012-2013 was 63.5% (95% CI, 62.1%-64.9%). Findings from the time-to-event analyses are displayed in Table 3 and Table 4.

Prevalence of comorbidities on the x-axis for participants who have the condition on the y-axis, with associated relative risks (data from 2012-2013).
COPD = chronic obstructive pulmonary disease; IHD = ischemic heart disease.
Note: Conditions with a prevalence <5% were excluded (see Table 2). Relative risks are for having the comorbidity on the x-axis given the individual has the condition on the y-axis.
Effect of Baseline Characteristics on Time to Developing Incident Multimorbidity Between 2002-2003 and 2012-2013: Complementary Log-Log Models
Relative Association Between the Presence of Individual Conditions on Time to Developing Incident Multimorbidity Between 2002-2003 and 2012-2013: Complementary Log-Log Model
Factors Associated With Incident Multimorbidity
The following associations were found for individuals with no baseline conditions (Table 3):
Incidence of multimorbidity accelerated with increasing age (linear trend, P <.001). There was a threshold effect for wealth, in that the least wealthy were more than twice as likely to develop incident multimorbidity at any wave as the wealthiest (hazard ratio [HR] = 2.19; 95% CI, 1.50-3.19; P <.001). Sex, education, and living alone were not significant.
Greater risk of multimorbidity at any wave was associated with being obese (HR = 1.92; 95% CI, 1.43-2.59; P <.001), and decreasing physical activity (linear trend, P = .031). Believing life events are outside one’s control (external locus of control) represented a 41% increased risk of multimorbidity at any wave (95% CI, 10%-82%; P = .007). Smoking behavior and social detachment were not associated.
Factors Associated With an Incident Condition
The model investigating factors associated with any increase in reported conditions (Table 3) showed trends similar to the model for individuals with no initial conditions. Increasing age, being in the least wealthy quintile, being obese, decreasing physical activity, and having an external locus of control were all significantly associated with acquiring an incident condition. Additionally, being a current smoker accelerated the acquisition of an incident condition (HR = 1.21; 95% CI 1.07-1.36; P = .002), with a marginal trend for having smoked in the past.
Impact of Individual Conditions
In the model comparing the effects of individual conditions on incident multimorbidity (Table 4), the conditions significantly more predictive than hypertension (the modal category used as the reference) were arrhythmia (HR = 1.55; 95% CI, 1.06-2.26; P = .024), chronic obstructive pulmonary disease (COPD) (HR = 2.32; 95% CI, 1.55-3.46; P <.001) and asthma (HR = 1.33; 95% CI, 1.05-1.70; P <.019).
Sensitivity Analyses
We conducted further analyses using outcome measures derived from condition counts that separated ischemic heart disease into angina and myocardial infarction, and combined COPD and asthma into a respiratory condition. The pattern of results described above was unaltered.
DISCUSSION
Our analysis of a large, nationally representative cohort, followed up for 10 years, identified a number of sociodemographic and lifestyle factors associated with incident multimorbidity, which were similar across baseline morbidity groups, and identified specific conditions associated with a relatively increased risk of developing multimorbidity.
Comparison With Previous Studies
Our findings confirm previous consistent findings for 2 sociodemographic factors: increased risk of multimorbidity with older age and lower socioeconomic status.4,16,21 The lack of association with female sex and with education is not new; previous findings are inconsistent on the association of these 2 factors with multimorbidity.16 Our observation that lower physical activity, higher BMI, smoking, and external locus of control are associated with increased risk of multimorbidity confirms previous findings.21, 29–33 Our findings extend knowledge of this area in one further regard: we found that COPD, asthma, and arrhythmias are associated with higher risk of multi-morbidity, thereby facilitating the identification of high-risk populations based on clinical diagnoses.
Strengths and Limitations
The longitudinal, prospective nature of these data, the consistency with previous studies, the simultaneous adjustment for multiple associated factors, and the observed linear trends (indicative of dose-response relationships) provide support for a causal relationship between the identified factors and incident multimorbidity. The key strengths of ELSA are the size of the cohort, and the breadth of sophisticated measures available for use as covariates, spanning socioeconomic, lifestyle, and health behavior domains. These measures allowed a more thorough and comprehensive investigation of risk factors than is usually achievable with electronic health record data sets.
The presence of conditions was self-reported by participants, which may be less reliable than ascertaining diagnoses from medical records. The reports of conditions were also restricted to those included in the ELSA interview. As such, the prevalence and incidence rates reported are likely to be underestimated. Self-reports of conditions may also depend on the number of physician visits, for which we were not able to control. Although the initial ELSA cohort was sampled to be representative of private residents in England aged 50 years and older, loss to follow-up during successive waves meant that representativeness was lost. Sample weights to adjust for differential nonresponse were provided with the ELSA data, which were used in all relevant analyses. Our measure for locus of control was a single, unvalidated item, and it could not distinguish between a genuine external locus or a functionally external locus because of a lack of resources or abilities.
Implications for Policy, Clinical Practice, and Research
Whereas much of current efforts are being aimed at improving care processes and outcomes for people with multimorbidity,10, 34 our findings suggest that there is scope for a prevention strategy focusing on reducing the incidence of multi-morbidity. A number of the factors in our analyses are risk factors for multiple individual conditions (smoking behavior, being obese, and low levels of physical activity) and are amenable to change through available behavior-change interventions. Locus of control has been linked to behavior change,31,35 and can be successfully modified by existing interventions.36
Taken together, these findings suggest that future work aimed at reducing the incidence of multimorbidity should design and evaluate interventions that include evidence-based components addressing behavioral change for promoting healthy lifestyles. Additionally, such interventions should seek to help patients gain a more internal health-related locus of control to empower them to achieve and maintain such change, with the potential for synergistic effects. The cost-effectiveness of such interventions should be compared against current practices in the delivery of condition-specific preventative care. In the absence of such more complex interventions, health policy and clinical practice oriented to the implementation and delivery of existing behavior change should be prioritized. High-risk populations can be defined based on the sociodemographic and clinical factors identified in this study.
Identifying specific patterns in the development of multimorbidity was beyond the scope of this study. Further research on multimorbidity clusters is needed to clarify relevant mechanisms: co-prevalence with increasing age (eg, osteoporosis and arthritis) vs shared pathophysiology (eg, hypertension and coronary artery disease). Future work should also account for morbidity burden—for example, the level of control of such conditions as diabetes, ischemic heart disease, and arthritis—which may provide a more meaningful measure of morbidity to clinicians and patients than using counts of conditions.
Footnotes
Conflicts of interest: authors report none.
Funding support: There was no direct funding for this study. Dr Mounce was supported by the National Health Service, Cambridgeshire, and through an National Institute for Health Research Clinical Scientist Award granted to Dr Valderas.
Supplementary materials: Available at http://www.AnnFamMed.org/content/16/4/322/suppl/DC1/.
- Received for publication November 20, 2017.
- Revision received April 3, 2018.
- Accepted for publication April 19, 2018.
- © 2018 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- Analytical approaches to evaluate risk factors of multimorbidity: a systematic scoping review protocol
- Association of polydoctoring and mortality among persons over 85 years with multimorbidity: a prospective cohort study in Japan
- Work-Family conflict among hotel housekeepers in the Balearic Islands (Spain)
- Effects of individual and parental educational levels on multimorbidity classes: a register-based longitudinal study in a Danish population
- Magnitude, pattern and correlates of multimorbidity among patients attending chronic outpatient medical care in Bahir Dar, northwest Ethiopia: the application of latent class analysis model
- Multimorbidity of chronic non-communicable diseases: burden, care provision and outcomes over time among patients attending chronic outpatient medical care in Bahir Dar, Ethiopia--a mixed methods study protocol
- Household and area-level social determinants of multimorbidity: a systematic review
- Biomarkers in the prediction of multimorbidity: scoping review
- Sociodemographic and lifestyle predictors of incident hospital admissions with multimorbidity in a general population, 1999-2019: the EPIC-Norfolk cohort
- Multimorbidity of chronic non-communicable diseases and its models of care in low- and middle-income countries: a scoping review protocol
- Prevalence, characteristics, and patterns of patients with multimorbidity in primary care: a retrospective cohort analysis in Canada
- In This Issue: Teachable Moments for Patients, Practices, and Systems