
Abstract
PURPOSE The purpose of this study was to examine the incremental effect of performance coaching, delivered as part of a multicomponent intervention (Ottawa Model for Smoking Cessation [OMSC]), in increasing rates of tobacco-dependence treatment by primary care clinicians.
METHODS In a cluster-randomized controlled trial, 15 primary care practices were randomly assigned to 1 of the following active-treatment conditions: OMSC or OMSC plus performance coaching (OMSC+). All practices received support to implement the OMSC. In addition, clinicians in the OMSC+ group participated in a 1.5-hour skills-based coaching session and received an individualized performance report. All clinicians and a cross-sectional sample of their patients were surveyed before and 4 months after introduction of the interventions. The primary outcome measure was rates of tobacco-dependence treatment strategy (Ask, Advise, Assist, Arrange) delivery. Secondary outcomes were patient quit attempts and smoking abstinence measured at 6 months’ follow-up.
RESULTS Primary care clinicians (166) and patients (1,990) were enrolled in the trial. Clinicians in the OMSC+ group had statistically greater rates of delivery for Ask (adjusted odds ratio [AOR] = 1.69; 95% CI, 1.05-2.72), Assist (AOR = 1.64; 95% CI, 1.08-2.49), and Arrange (AOR = 2.01; 95% CI, 1.22-3.31). Sensitivity analysis found that the rate of delivery for Advise was greater only among those clinicians who attended the coaching session (AOR = 1.65; 95% CI, 1.10-2.49; P = .02). No differences were documented between groups for cessation outcomes.
CONCLUSIONS Performance coaching significantly increased rates of tobacco-dependence treatment by primary care clinicians when delivered as part of a multicomponent intervention.
- smoking cessation
- primary care
- audit and feedback
- randomized controlled trial
- coaching
- quality improvement
- knowledge translation
- Ottawa Model for Smoking Cessation
INTRODUCTION
Smoking cessation is arguably the most powerful preventive intervention available in primary care practice.1-3 The 5 As strategy (Ask, Advise, Assess, Assist, Arrange) is the basis for tobacco-dependence treatment in clinical settings; however, integrating evidence-based tobacco-dependence treatment into clinical practice routines remains a challenge.1-8 The important role of family medicine in addressing tobacco use with patients is well recognized, and multiple international guidelines and reports have identified the need to increase rates of tobacco-dependence treatment in primary care settings.1-9
Strategies, including clinician training, electronic health record (EHR) prompts, and adjunct counseling, have been shown to significantly increase rates of tobacco-dependence treatment in primary care settings.10-14 Meta-analyses show that multicomponent interventions combining several intervention strategies are the reference standard for increasing clinician performance in delivering tobacco-dependence treatment.1 The Ottawa Model for Smoking Cessation (OMSC) is a multicomponent quality improvement intervention for addressing tobacco use with smokers in clinical settings that has been implemented in more than 350 hospitals and primary care practices in Canada (http://www.ottawamodel.ca).15-18 The OMSC supports primary care teams with the introduction of a systematic, team-based approach to addressing tobacco-dependence treatment delivery based on 10 best practices.19 Evaluations of the OMSC in primary care settings have documented a significant increase in clinician delivery of evidence-based tobacco-dependence treatments.14-15 Despite an overall increase in treatment rates, significant variability in rates of tobacco-dependence treatment delivery can exist among individual clinicians exposed to the OMSC—even within the same practice.15-16 This variability suggests that the intervention does not take hold among all clinicians in the same way; clinician-level factors may be responsible for some of the observed variance.20-23
Continuing medical education for tobacco-dependence treatment typically involves a single session using didactic training methods. Tobacco-dependence treatment can be a complex clinical intervention, however, requiring a number of skills; 1-time didactic educational sessions may be inadequate for some clinicians. Active forms of continuing medical education, such as interactive training including audit and feedback, are promising methods for ensuring the implementation of evidence-based guidelines within general practice.24-26 Evidence from the health care quality improvement literature suggests that reinforcement training and peer coaching may improve physicians’ and medical residents’ patterns of practice.27-33
The primary objective of this study was to compare the incremental effectiveness of clinician performance coaching when delivered as part of a multicomponent intervention (OMSC) on rates of tobacco-dependence treatment in family practice, compared with the multicomponent intervention alone. Secondary objectives were assessments of the effect of the intervention on patient quit attempts and smoking abstinence.
METHODS
Study Design
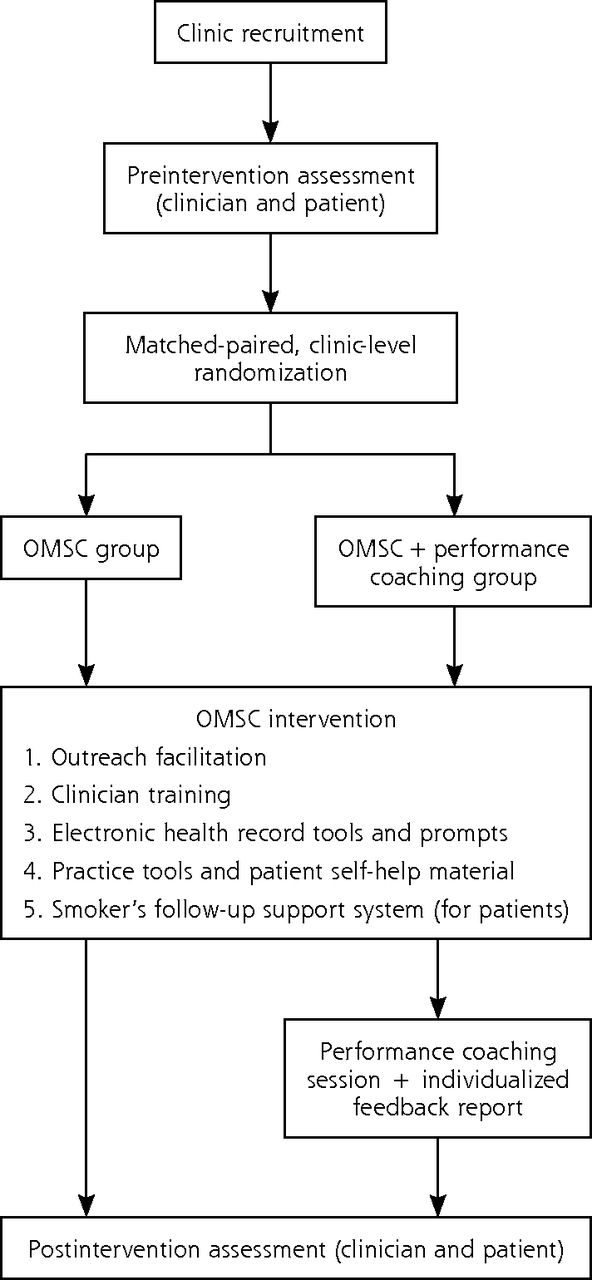
A cluster-randomized controlled trial was undertaken with family health teams (≥5 clinicians) in the province of Ontario, Canada (Figure 1). The complete research protocol for the trial has been published.19 Family medicine practices were matched and randomly assigned to 1 of the following intervention arms: OMSC or OMSC plus clinician performance coaching (OMSC+). From each of the participating practices, a cross-sectional sample of eligible tobacco users was recruited before and after intervention to assess clinicians’ performance in tobacco-dependence treatment delivery (4 As), patient quit attempts, and biochemically verified 7-day point-prevalence abstinence. The trial was approved by the Ottawa Health Science Network Research Ethics Board.

Randomized controlled trial study design.
OMSC = Ottawa Model for Smoking Cessation.
Randomization and Concealment
The average rate for delivery of the Advise strategy for each practice at baseline was used to match practices before randomization because previous evaluations of the OMSC have shown imbalance in this variable.15,16 Randomization was conducted by the Research Methods Centre (University of Ottawa Heart Institute, Ottawa, Ontario, Canada), which was blind to practice identifiers. Patients and research assistants were blinded to their practice’s group assignment.
Clinical Model
The OMSC is grounded in the latest evidence-based guidelines for tobacco treatment and uses an adaptation of the well-known 5 As model, which includes the following15,16: (1) Asking all patients about their smoking status; (2) delivering personalized Advice to quit smoking to all smokers and offering support with cessation; (3) Assisting patients ready to quit smoking by developing a personalized plan for quitting that involves scheduling a dedicated visit to deliver evidence-based counseling to support cessation, set a quit date, select a quit-smoking pharmacotherapy, and provide self-help material; and (4) Arranging follow-up support, which includes counseling and management of pharmacotherapy to prevent relapse, for 2 to 6 months. Follow-up is typically scheduled monthly after a patient’s quit date. Patients had the option to receive additional telephone-based support between clinic appointments.
Ottawa Model for Smoking Cessation Intervention
The OMSC intervention model supports teams in implementing the 5 As clinical model by using a quality improvement process focused on the introduction of the OMSC 10 Best Practices for delivering tobacco-dependence treatment (Table 1).18 All teams were exposed to this multicomponent intervention that combines several evidence-based strategies including (1) outreach facilitation, (2) clinician training, (3) EHR tools and prompts, (4) practice tools and patient self-help material, and (5) smoker’s follow-up system.5,10,11 Table 2 provides a description of the OMSC intervention components.
OMSC 10 Best Practices
Summary of OMSC Multicomponent Intervention Components
Ottawa Model For Smoking Cessation Plus Clinician Performance Coaching
The OMSC+ group received the same multicomponent intervention as the OMSC group. In addition, general practitioners and nurse practitioners received a supplemental 1.5-hour coaching session approximately 4 weeks after the launch of the OMSC at their clinic and received an individualized performance report. The performance coaching intervention was delivered in a group format, at each practice location, by a trained tobacco-dependence treatment specialist using a standardized facilitation guide. Given that clinician self-efficacy (ie, confidence) is associated with rates of tobacco-dependence treatment delivery, this intervention was designed to influence the following 4 factors known to affect self-efficacy: (1) skills training, (2) personal experience, (3) modeling of behaviors, and (4) positive social or environmental supports.34,35 During this session, clinicians identified personal barriers as well as success strategies for tobacco-dependence treatment delivery. The session facilitator introduced 7 techniques that clinicians could use in their practices to address known barriers, with a particular focus on addressing patient resistance, ambivalence, stress, and mental health issues.18 Peer-to-peer exchange and role modeling were used as teaching techniques.34
Data Collection
All participating clinicians and patients provided written informed consent. The characteristics of practices and clinicians were collected at baseline. At each practice, before implementation of the intervention, consecutive patients arriving for appointments were screened for eligibility. Eligible patients were aged ≥18 years, smoked an average of at least 5 cigarettes per day, were scheduled for an annual examination or nonurgent medical appointment with a physician and/or nurse practitioner, and were able to read and understand English or French. Patients were not required to be ready to quit smoking to be eligible to participate. All patient participants completed an exit survey after their clinic visit and were contacted by telephone 6 months (±2 weeks) after their clinic visit to assess cessation outcomes. After practices had implemented the intervention for at least 4 months, postimplementation data were collected from clinicians via a follow-up survey and from a second cross-sectional sample of patients using procedures identical to those used at baseline.
Outcome Measures
The primary outcome was rates of clinician tobacco-dependence treatment delivery of 4 of the 5 As (Ask, Advise, Assist, Arrange). We chose not to examine the Assess component in the present study to reduce respondent burden. The study exit survey asked patients whether or not (binary scale: yes, no) at today’s clinic appointment their physician or another member of the team asked them about their smoking status (Ask), advised them to quit smoking (Advise), provided assistance with quitting (Assist), or arranged follow-up support (Arrange). For the Assist strategy, supplemental data were collected regarding the type of assistance (eg, providing self-help materials, setting a quit date, discussing or prescribing smoking-cessation drugs). Patient exit interviews have been used in most previous evaluations of tobacco-dependence treatment interventions in primary care; they have been shown to be more reliable than clinician self-report.36
Patient self-reports of quit attempts lasting 24 hours or more after their index visit, 7-day point-prevalence abstinence (not having smoked even a puff in the past 7 days), and 12-week continuous abstinence (not having smoked even a puff from week 14 up to week 26) were assessed at the 6-month telephone follow-up interview.36 The NicAlert saliva cotinine test was used for biochemical validation (>10 ng/mL) of smoking status.37,38 Participants were mailed the NicAlert test, instruction sheet, and a prepaid package for returning the kit. Patients lost to follow-up were assumed to be active smokers.37
Sample Size and Analysis
Sample-size calculations were adjusted for the cluster-randomized controlled trial design and informed by previous OMSC evaluations.15,16 All calculations were based on a 1-sided test with 80% power, an α level of .05, and intraclass correlation coefficients (ICCs) of 0.05 for 4 As and 0.01 for cessation.39 Sample-size calculations indicated that 10 practices per group with 60 patients per practice were required to detect a minimum difference of 10% between intervention groups for 4 As delivery and 5% for smoking abstinence.
Multilevel models account for the clustered design. A 3-level generalized linear mixed model estimated the effect of the intervention for each outcome measure with the following levels: patients (level 1), clinicians (level 2), and clinics (level 3). Wald tests were used to obtain P values, adjusted odds ratios [AORs], and 95% CIs. Both practice-level ICCs (ie, variation between practices) and clinician-level ICCs (ie, variation between individual clinicians) were calculated. ICC is measured on a scale from 0 to 1, with a value close to 0 indicating that the clusters were similar.38 Data analysis was conducted on an intention-to-treat basis (ie, all clinicians and all patients as allocated to the intervention). Sensitivity analysis examined attendance at the coaching session. All analyses were conducted using SAS 9 (SAS Institute Inc).
RESULTS
Recruitment Flow
Fifteen practices and 166 clinicians were enrolled in the trial. The study was conducted from September 2013 to May 2015. The patient sample comprised 1,123 eligible smokers who participated in the preassessment and a second cross-sectional sample of 867 smokers who participated in the postassessment. Six-month telephone follow-up data were available for ~77% of patients at both the pre- and postassessments, with no between-group differences. The Consolidated Standards of Reporting Trials (CONSORT) study flow diagram is shown in Supplemental Figure 1, http://www.annfammed.org/content/16/6/498/suppl/DC1.
Practice, Clinician, and Patient Characteristics
There were no differences in practice and clinician characteristics between intervention groups (Supplemental Table 1, http://www.annfammed.org/content/16/6/498/suppl/DC1). Patient characteristics are presented in Supplemental Table 2, http://www.annfammed.org/content/16/6/498/suppl/DC1.
Rates of Tobacco-Dependence Treatment Delivery
Both the OMSC and OMSC+ groups documented significant increases in rates of Ask, Advise, and Assist between the pre- and postassessments (Table 3).
Clinician Performance in 4 As Delivery and Patient Outcomes at Postintervention Assessment by Intervention Group
Clinicians in the OMSC+ group had statistically greater performance in the rates of Ask (AOR = 1.69; 95% CI, 1.05-2.72), Assist (AOR = 1.64; 95% CI, 1.08-2.49), and Arrange (AOR = 2.01; 95% CI, 1.22-3.31) compared with the OMSC group (Table 4). No significant difference was observed in the rates of Advise in the intention-to-treat analysis.
Clinician Performance in Tobacco-Dependence Treatment Delivery at Postassessment by Intervention Group
A total of 34% of clinicians randomized to the OMSC+ group did not attend the performance coaching session, owing to annual leave, maternity leave, or illness. Sensitivity analysis found that rates of Ask (AOR = 1.51; 95% CI, 1.01-2.26), Advise (AOR = 1.65; 95% CI, 1.10-2.49), and Assist (AOR = 1.50; 95% CI, 1.03-2.19) were significantly greater among clinicians who attended the coaching session compared with clinicians who were not exposed to performance coaching (Supplemental Table 3, http://www.annfammed.org/content/16/6/498/suppl/DC1).
Clinicians who documented lower performance at baseline (<40%) had greater overall increases in rates of Ask and Advise relative to higher-performing clinicians (Figure 2). Changes in rates of Assist and Arrange were found to be similar between low- and high-performing clinicians. Clinicians were more likely to Ask, Advise, and Assist if the patient was seen in the clinic for a first visit or annual examination compared with other types of appointments (Supplemental Table 4, http://www.annfammed.org/content/16/6/498/suppl/DC1). Clinicians’ beliefs about the importance of cessation were associated with rates of Ask (AOR = 4.36; 95% CI, 2.05-9.29; P < .001). Patient readiness to quit and smoking-related illness were also associated with 4 As delivery (Supplemental Table 4).
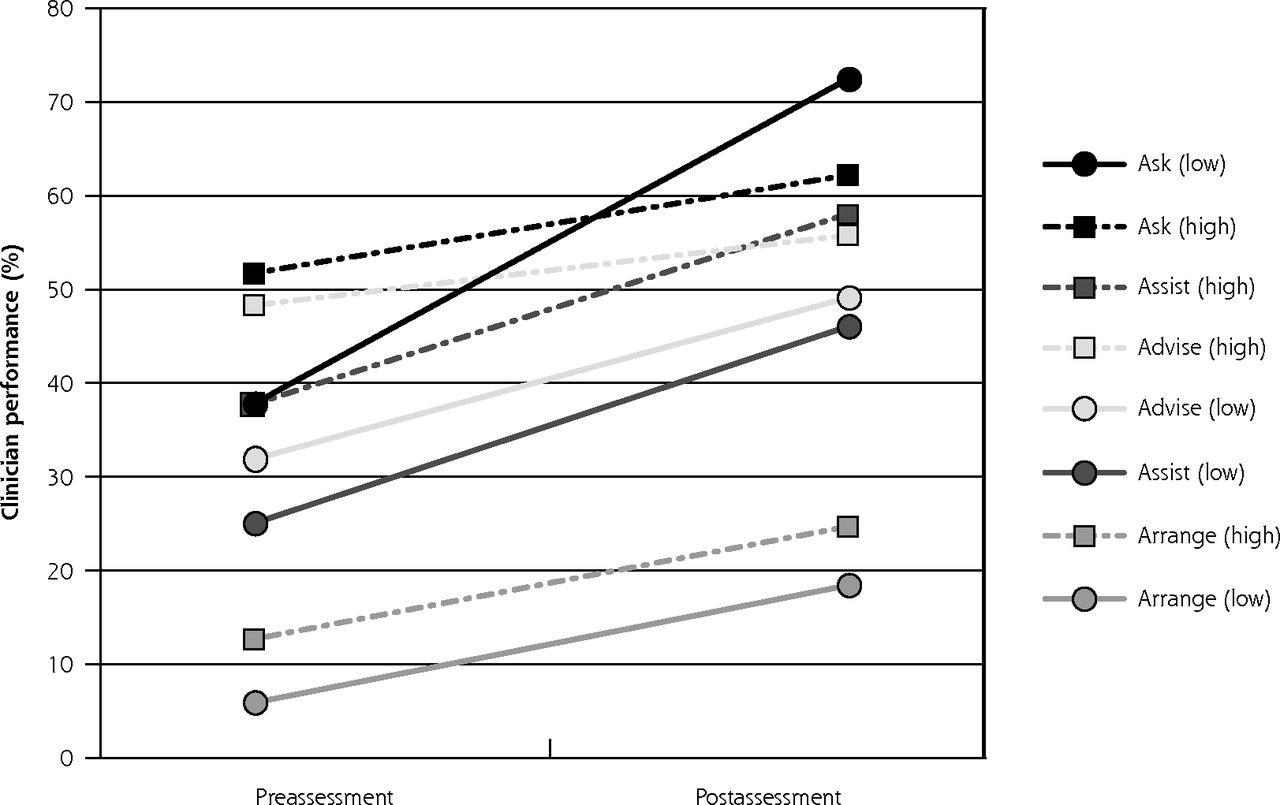
Clinician performance in tobacco-dependence treatment delivery at pre- and postassessment in the intervention group according to clinic baseline performance.
Note: Low-performing clinics had a baseline rate of Advise <40.5%; high-performing clinics had a baseline rate of Advise ≥40.5%.
Cessation Outcomes
Multilevel regression analysis showed a borderline effect of intervention group on quit attempts (AOR = 1.36; 95% CI, 1.00-1.84) but no significant effect on patient smoking cessation (Table 4). A small decrease was observed in self-reported 7-day point-prevalence abstinence between the pre- and postassessments in the OMSC+ group. There were no statistically significant differences in rates of smoking abstinence between groups.
Patients were significantly more likely to be abstinent at the follow-up if they were ready to quit smoking in the next 30 days at the index visit, reported high self-efficacy with quitting, did not report anxiety or depression, and had a dedicated smoking cessation visit scheduled at the primary care clinic (Supplemental Table 5, http://www.annfammed.org/content/16/6/498/suppl/DC1).
DISCUSSION
Consistent with earlier evaluations of the OMSC, both of the active-intervention groups increased rates of tobacco-dependence treatment delivery. There was a further incremental increase in the rates of tobacco-dependence treatment delivered by clinicians when the multicomponent intervention was combined with clinician performance coaching. The performance coaching intervention was informed by behavior change theory, quality improvement literature, and previous research. Participants received coaching from both a trained tobacco-dependence treatment specialist and higher-performing peers from their own practice setting. The coaching sessions were well attended, well received, and were easily implemented in the context of general practice. A small number of trials have evaluated the efficacy of reinforcement contact, educational outreach visits, or performance feedback after tobacco-dependence treatment training and found them to be associated with desirable changes in clinician behaviors.40-46 Evidence from the broader primary care literature has documented the value of educational outreach visits, audits, and feedback.26-28 Systematic reviews have found that feedback is most effective when delivered by a respected colleague, presented frequently, and features both specific goals and action plans.26-28 Performance feedback has also been found to be particularly useful in assisting clinicians with low baseline performance.26,27 In the present study, we also observed that clinicians with lower baseline performance with respect to Ask and Advise showed greater overall increases in treatment rates relative to higher-performing colleagues.
The coaching session did not significantly affect 6-month smoking abstinence rates when compared with the OMSC intervention. It is possible that the strength of the intervention program was insufficient in producing clinic-wide patient-level increases in cessation, a finding that has been reported by others.47-49 Smokers enrolled in the present study were heavily nicotine dependent, and it is likely that more-intensive treatment may be needed to support cessation in this patient population. Importantly, and unlike other evaluations in primary care, our study included all smokers and not just those ready to quit smoking. Patients who scheduled for a quit plan visit were significantly more likely to report abstinence from smoking, suggesting that this is an important component of treatment success. Changes in clinician-level behavior observed among practices exposed to the OMSC can be lever aged to facilitate the uptake of evidence-based treatment in future research.
Our findings should be interpreted in light of certain study limitations. First, the study compared 2 active-intervention arms and did not include a control condition. All participating practices were family health teams in the province of Ontario, Canada; the generalizability to other practice models or to other health care systems would require further examination. The assessment was based on patient report of 4 As delivery, which may be subject to reporting bias. Electronic health record data collection for 4 As delivery was not established in clinics at baseline and as such could not be used to examine pre- and post-rates of 4 As delivery. We reported on data for same-day clinic encounters, and as such our findings may not be comparable to studies or reports that use longer time frames (ie, previous 12 months). Our study provides evidence regarding the value of performance coaching when delivered as part of a multicomponent intervention rather than as a stand-alone intervention. We tested a single coaching session, and it is possible that exposure to additional coaching sessions might further increase the likelihood of tobacco-dependence treatment delivery. The optimal amount and frequency of performance coaching is an area for future research.
Identifying and evaluating simple, effective techniques for promoting tobacco-dependence treatment delivery is essential to improving the reach of tobacco-dependence treatment interventions in primary care settings. This study lends support for the integration of performance coaching in the design and delivery of multicomponent interventions to further increase rates of tobacco-dependence treatment delivery, particularly among low-performing clinicians.
Acknowledgments:
The authors thank the staff and clinicians of the primary care clinics involved in this study for their participation. Our thanks to Kelly Cobey and Klea Bertakis for reviewing this manuscript.
Footnotes
Funding support: This study was funded by a grant-in-aid from the Heart and Stroke Foundation of Canada (Grant #NA7193).
Conflicts of interest: R.D.R. has received speaker and consulting fees from Pfizer and Johnson & Johnson; K-A.M. has received speaker fees from Pfizer; A.L.P. has received speaker and consulting fees from Pfizer and Johnson & Johnson. All others report none.
To read or post commentaries in response to this article, see it online at http://www.AnnFamMed.org/content/16/6/498.
Previous presentation: Partial results of this paper were presented at the Society for Research on Nicotine and Tobacco Annual Meeting; March 8-11, 2017; Florence, Italy.
Clinical trial registry: NCT01603524.
Supplementary materials: Available at http://www.AnnFamMed.org/content/16/6/498/suppl/DC1/.
- Received for publication April 3, 2018.
- Revision received July 20, 2018.
- Accepted for publication September 1, 2018.
- © 2018 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}