
Article Figures & Data
Figures
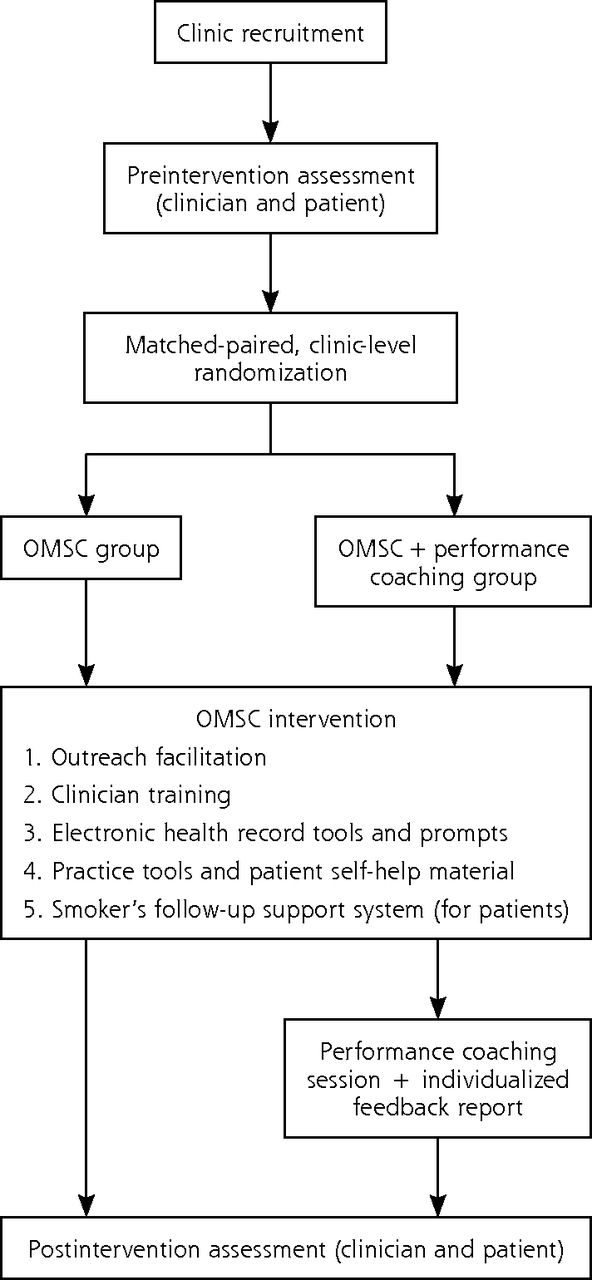
- Figure 1
Randomized controlled trial study design.
OMSC = Ottawa Model for Smoking Cessation.
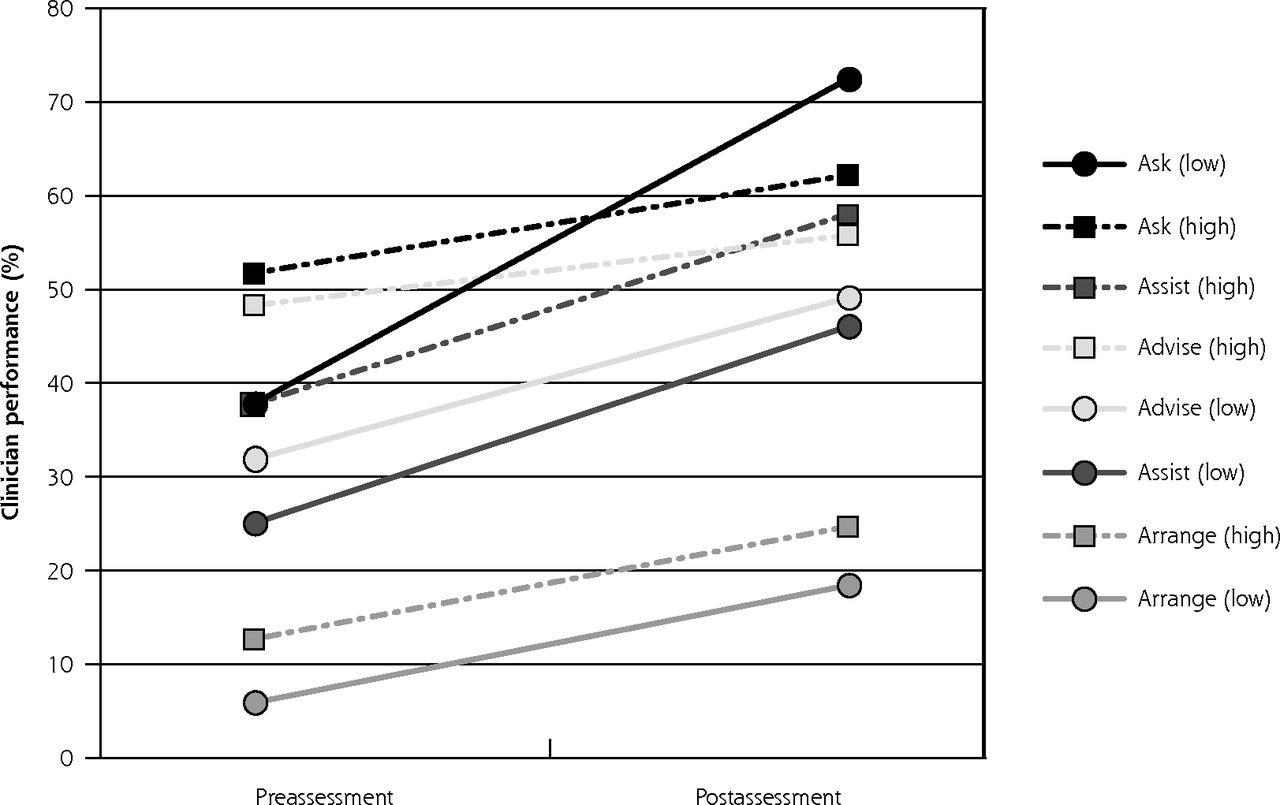
- Figure 2
Clinician performance in tobacco-dependence treatment delivery at pre- and postassessment in the intervention group according to clinic baseline performance.
Note: Low-performing clinics had a baseline rate of Advise <40.5%; high-performing clinics had a baseline rate of Advise ≥40.5%.

Tables
1. Clinic task force formed 2. Clinic tobacco-control protocol developed 3. Tobacco use queried and documented for all clinic patients 4. Training in tobacco-dependence treatment completed by clinicians in past year 5. Specific staff identified to provide tobacco-dependence treatment 6. Self-help materials available to patients, family members, and staff 7. EHR or other real-time prompt in place to inform GP/NP of patient smoking status, advice delivery, and quit plan consult forms 8. Process to follow-up tobacco users for at least 2 to 6 months after clinic visit 9. Process to evaluate quality of program implementation in place 10. Process to provide feedback to practices about clinic performance in tobacco-dependence treatment delivery EHR = electronic health record; GP = general practitioner; NP = nurse practitioner; OMSC = Ottawa Model for Smoking Cessation.
Adapted with permission from Papadakis S, Cole AG, Reid RD, et al. Increasing rates of tobacco treatment delivery in primary care practice: Evaluation of the Ottowa Model for Smoking Cessation. Ann Fam Med. 2016:14(3):235-243.
Component Description Outreach facilitation visits Trained outreach facilitator works with each primary care clinic over a 3-month period to implement the program 7-step facilitation process used to introduce OMSC 10 Best Practices. Facilitators act by supporting clinics as follows: Review current clinic practices for delivery of evidence-based smoking cessation intervention and complete needs assessment Provide information and recommendations on integration of evidence-based smoking cessation strategies into clinical practice Facilitate development of clinic tobacco-dependence treatment protocol for integrating evidence-based smoking cessation strategies into all clinic appointments Define roles and responsibilities of clinic staff for delivering evidence-based smoking cessation treatments Support communications and training activities for members of clinic staff Clinician training Frontline physicians and nurse practitioners participate in 3-hour training session providing information and skills training for addressing tobacco use with patients in the context of a busy primary care practice setting Key staff responsible for delivering quit plan visits (eg, nurse, nurse practitioner, pharmacist) attend intensive 1-day training session teaching how to conduct quit plan and follow-up visits based on evidence-based practice Electronic health record tools and real-time prompts Real time point-of-care reminders (eg, standard smoking-status questions) introduced and embedded in vital-sign screening forms and prompts to document smoking status and deliver brief advice Standardized check-list style smoking cessation consult forms embedded into EHRs to guide tobacco treatment delivery for advice, quit plan, and follow-up visit Practice tools and patient self-help material All materials designed to support intervention delivery and reduce amount of face-to-face time required to support tobacco-dependence treatment delivery. Materials include the following: Patient tobacco use survey to document smoking history Patient self-help quit plan booklet for smokers ready to quit Patient self-help booklet for smokers not ready to quit Clinic waiting room posters and materials Smoker’s follow-up support system Patients ready to quit referred to smoker’s follow-up system including 5 triage calls or e-mails delivered over a 2-month period (3, 7, 14, 30, 60 days after quit date) by automated program. Patients struggling with quit attempt had additional telephone-based support arranged from trained smoking-cessation counselors, and as required, changes to their quit plan coordinated with primary care clinician EHR = electronic health record; OMSC = Ottawa Model for Smoking Cessation.
Adapted with permission from Papadakis S, Cole AG, Reid RD, et al. Increasing rates of tobacco treatment delivery in primary care practice: Evaluation of the Ottowa Model for Smoking Cessation. Ann Fam Med. 2016:14(3):235-243.
- Table 3
Clinician Performance in 4 As Delivery and Patient Outcomes at Postintervention Assessment by Intervention Group
Parameter OMSC OMSC+ Pre
n = 540Post
n = 394AOR (95% CI)a P
ValuebPre
n = 583Post
n = 473AOR (95% CI)a P
Valueb4 As delivery Ask 47.3 55.9 1.45 (1.10-1.92) .009 46.8 65.7 2.40 (1.83-3.14)c <.001 Advise 38.1 48.1 1.63 (1.20-2.11) .001 42.5 53.5 1.71 (1.31-2.24) <.001 Assist 35.1 42.8 1.44 (1.09-1.91) .011 33.3 53.9 2.62 (1.99-3.45) <.001 Set quit date 12.4 12.1 1.03 (0.68-1.55) .898 11.2 18.7 1.93 (1.33-2.79) .001 Self-help 10.0 11.1 1.19 (0.77-1.84) .444 10.8 19.4 2.05 (1.42-2.98) .001 Discuss medications 25.5 26.9 1.11 (0.81-1.51) .517 26.1 37.1 1.87 (1.41-2.50) <.001 Prescribe medications 8.7 8.8 1.11 (0.68-1.80) .670 9.1 12.2 1.47 (0.96-2.27) .080 Arrange 12.2 13.4 1.10 (0.73-1.66) .649 10.3 22.5 2.66 (1.84-3.84) <.001 Patient-level outcomes Quit attempts 29.0 30.0 1.01 (0.75-1.36)c .934 27.8 35.0 1.41 (1.07-1.86)c .015 7-day point-prevalence abstinence (self-reported) 4.6 9.1 2.18 (1.25-3.82)c .006 6.0 6.5 1.13 (0.65-1.96) .669 7-day point-prevalence abstinence (biochemically validated) 0.0 2.8 … … 0.3 2.5 13.03 (1.65-102.84)c .015 6-month continuous abstinence 4.1 6.6 1.75 (0.92-3.30) .086 4.0 4.8 1.30 (0.69-2.45) .423 AOR = adjusted odds ratio; OMSC = Ottawa Model for Smoking Cessation; post = postassessment; pre = preassessment.
↵a Controlling for clinic-level variance between clusters, patient sex, patient education, and self-reported anxiety or depression; based on inclusion of 15 clinics unless otherwise indicated.
↵b P value based on Wald statistic.
↵c The estimated G matrix for clinic-level variance was not a definite positive, so clinic-level variance was not included in this model.
- Table 4
Clinician Performance in Tobacco-Dependence Treatment Delivery at Postassessment by Intervention Group
Parameter OMSC
(n = 394)OMSC+
(n = 473)% Delta AOR
(95% CI)aP Value ICC Clinician ICC Clinic 4 As delivery Ask 55.9 65.7 9.8 1.69 (1.05-2.72) .03 0.126b 0.025 Advise 48.1 53.5 5.4 1.42 (0.82-2.46) .22 0.129 0.045 Assist 42.8 53.9 11.1 1.64 (1.08-2.49) .02 0.089c 0.027 Set quit date 18.9 25.7 6.8 1.70 (1.09-2.65) .02 0.037 0.035 Self-help 11.1 19.4 8.3 2.01 (1.15-3.52) .02 0.072 0.043 Discuss medications 26.9 37.1 10.2 1.75 (1.15-2.65) .01 0.069 0.026 Prescribe medications 8.8 12.2 3.4 1.44 (0.85-2.42) .18 0.002 0.026 Arrange 24.7 35.6 10.9 2.01 (1.22-3.31) .01 0.036 0.050 Patient-level outcome Quit attemptsd 30.0 35.0 5.0 1.36 (1.00-1.84) .05 … … 7-day point prevalence abstinence (self-reported)d 9.1 6.5 −2.6 0.73 (0.43-1.26) .26 … … 7-day point prevalence abstinence (biochemically validated)d 2.8 2.5 −0.3 1.05 (0.42-2.64) .92 … … Continuous abstinence 6.6 4.8 −2.2 0.82 (0.40-1.67) .58 0.038 0.030 AOR = adjusted odds ratio; ICC = intraclass correlation coefficient; OMSC = Ottawa Model for Smoking Cessation.
↵a Controlling for clinic-level variance between clusters, patient sex, patient education, and self-reported anxiety or depression; based on inclusion of 15 clinics unless otherwise indicated.
↵b P < .01.
↵c P = .05.
↵d For ICC Clinician and ICC Clinic, the estimated G matrix was not a definite positive; therefore, we could not calculate clinician or clinic ICC.
Supplemental Appendix
Supplemental Appendix
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file
The Article in Brief
From Good to Great: The Role of Performance Coaching in Enhancing Tobacco-Dependence Treatment Rates
Sophia Papadakis , and colleagues
Background This study examines the effect of 'performance coaching' as part of a multi-component approach to increasing rates of treatment for tobacco dependence by primary care clinicians.
What This Study Found Integrating 'performance coaching' into the design and delivery of multi-component tobacco treatment interventions significantly increases rates of tobacco dependence treatment by primary care clinicians. In a cluster-randomized controlled trial, 15 primary care practices, including 166 primary care clinicians and 1,990 patients, were randomly assigned to one of two interventions. Both interventions helped teams implement the 5As model of treating tobacco use (Ask, Advise, Assess, Assist and Arrange) in the context of 10 best practices for delivering tobacco treatment. One intervention group also provided a 1.5-hour coaching session and an individualized performance report for family physicians and nurse practitioners. Both groups increased rates of tobacco dependence treatment delivery, however clinicians who received performance coaching had statistically higher rates of providing three elements of the 5 As: asking patients about their smoking status, assisting patients ready to quit by developing a quit plan, and arranging follow-up support. In sensitivity analysis, rates of tobacco cessation advice were greater among clinicians who attended a coaching session. There were no differences in tobacco cessation outcomes between the two groups.
Implications
- According to the authors, this study supports the integration of performance coaching into multi-component interventions to further increase the delivery of tobacco treatment, particularly among low-performing clinicians.




{kind=link}
{kind=link}