
Article Figures & Data
Figures
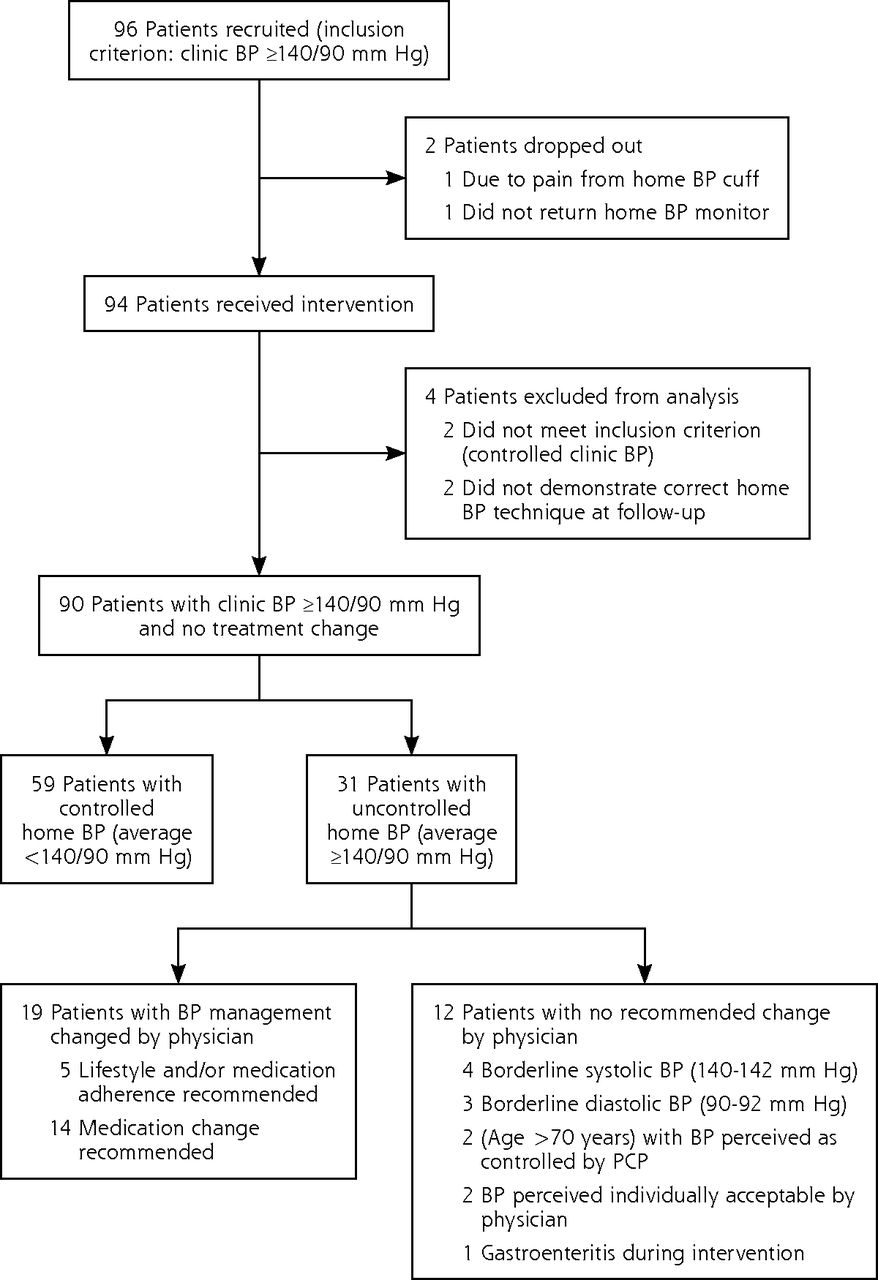
- Figure 1
Participant flow diagram.
BP = blood pressure; PCP = primary care physician.
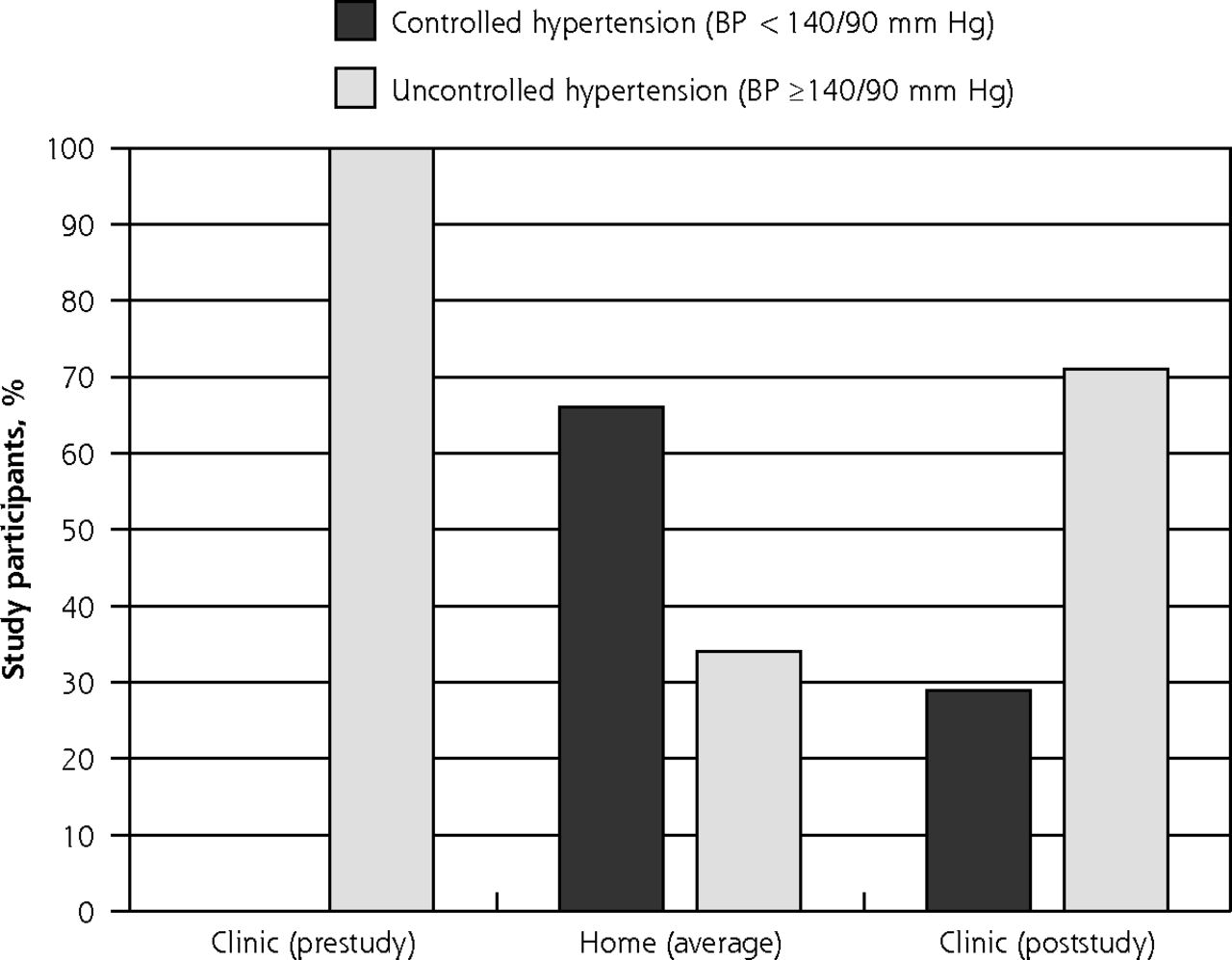
- Figure 2
Blood pressure values.
BP = blood pressure.


Tables
- Table 1
Sample Demographics, Overall and by Controlled and Uncontrolled Average Home BP Measurement
Home Blood Pressure Overall Controlled (<140/90 mm Hg) Uncontrolled (≥140/90 mm Hg) P Value Overall, No. (%) 90 (100.0) 59 (65.6) 31 (34.4) … Age, y, mean (SD) 61.7 (13.1) 61.4 (12.0) 62 (14.8) .75 <50, No. (%) 22 (22.2) 16 (22.0) 7 (22.6) 51-65, No. (%) 24 (26.6) 16 (27.1) 8 (25.8) ≥66, No. (%) 46 (51.1) 30 (50.8) 16 (51.6) Sex, No. (%) .34 Male 49 (54.4) 30 (50.8) 19 (61.3) Female 41 (45.6) 29 (49.2) 12 (38.7) Race, No. (%) .80 African American/black 9 (10.0) 5 (8.5) 4 (12.9) Caucasian/white 75 (83.3) 50 (84.7) 25 (80.6) Other 6 (6.7) 4 (6.8) 2 (6.4) BMI, mean (SD) 29.2 (6.1) 28 (5.7) 31.5 (6.5) .01 Education, No. (%) .52 High school diploma/GED or less 15 (16.7) 11 (18.6) 4 (12.9) Some college/2-year college degree 25 (27.8) 18 (30.5) 7 (22.6) 4-Year college degree/postgraduate work 24 (26.7) 13 (22.0) 11 (35.5) Postgraduate degree 26 (28.9) 17 (28.8) 9 (29.0) Smoking status (chart review), No. (%) .27 Current smoker 6 (6.7) 5 (8.5) 1 (3.2) Former smoker (last smoked >2 months) 30 (33.3) 17 (28.8) 13 (41.9) Never smoker 52 (57.8) 37 (62.7) 15 (48.4) Home BP readings, mean (SD) Home BP readings, total 73 (21.4) 72.1 (22.4) 74.9 (19.5) .55 Days from first to last home BP reading 14.1 (3.6) 14.2 (3.6) 14 (3.7) .76 Cardiovascular diseasesa (chart review), No. (%) Cardiovascular disease absent 47 (52.3) 27 (45.8) 20 (64.5) .09 Cardiovascular disease present 43 (47.7) 32 (54.2) 11 (35.5) Medications (self-reported) Total number OTC medications, mean (SD) 1.8 (1.5) 1.6 (1.4) 2.1 (1.6) .06 Report of lightheadedness, No. (%) 18 (20.0) 13 (22.0) 5 (16.1) .75 Medications (chart review) Dietary supplements 42 (46.7) 24 (40.7) 18 (58.1) .11 Psychoactive 26 (28.9) 17 (28.8) 9 (29.0) .98 Nonopioid 36 (40.0) 20 (33.9) 16 (51.6) .10 Opioid 14 (15.6) 10 (16.9) 4 (12.9) .61 Levothyroxine 12 (13.3) 8 (13.6) 4 (12.9) .93 Allergy 12 (13.3) 4 (6.8) 8 (25.8) .01 Total number of BP medications, mean (SD) 1 (0.9) 0.8 (0.8) 1.4 (1.1) .01 Total number of medications, mean (SD) 4.4 (2.9) 3.8 (2.7) 5.4 (3.1) .01 PROMIS scales (postsurvey) Adherence raw score, mean (SD) 34.9 (4.4) 35 (4.8) 34.8 (4) .97 Adherence T-score, mean (SD)b 48.7 (7.5) 49 (7.8) 48 (6.9) .77 Low, No. (%) 11 (21.6) 7 (25.0) 4 (20.0) … Moderate, No. (%) 29 (56.9) 16 (57.1) 13 (65.0) … High, No. (%) 8 (17.6) 5 (17.9) 3 (15.0) … BMI = body mass index; BP = blood pressure; GED = General Educational Development; OTC = over the counter; PROMIS = Patient-Reported Outcomes Measurement Information System.
Notes: P values based on c2 comparison (t test for continuous variables), by controlled vs uncontrolled. For the conrolled vs uncontrolled comparisons, column percentages are presented, unless noted, as a continuous outcome (mean, SD).
a Cardiovascular diseases: coronary heart disease, cerebrovascular disease, arrhythmia, heart valve disorder, heart failure, peripheral artery disease.24
↵b Adherence t scores grouped into low (>1 SD below mean), moderate (values within 1 SD above/below mean), and high (>1 SD above mean).
Mean (SD) Minimum Maximum Median Clinic BP (prestudy), mm Hg Systolic (n = 90) 158 (14) 131 207 154.5 Diastolic (n = 90) 91 (12) 63 132 92 Home BP (average), mm Hg Systolic (n = 90) 133 (10) 107 158 133.5 Diastolic (n = 90) 81 (8) 63 99 82 Clinic BP (poststudy)a, mm Hg Systolic (n = 70) 148 (18) 111 195 149.5 Diastolic (n = 70) 85 (11) 60 112 86 Prestudy clinic BP cutoff point Home BP<140/90 mm Hg,No. (%) <160/95 mm Hg (n = 39) 25 (64.1) >160/95 mm Hg (n = 51) 34 (66.7) <155/92 mm Hg (n = 32) 22 (68.8) >155/92 mm Hg (n = 58) 37 (63.8) BP = blood pressure.
↵a Poststudy sample size differed due to missing data (not all 90 patients had a 6-month follow-up visit).
Theme Quote Behavioral changes Healthier options “I am increasingly controlling the type of food I eat during the day.” Less salt “Reduce salt intake because one day I ate a small pack of pretzels inthe evening. My BP at the usual monitoring time (which was ~1.5hour of eating the pretzel) was noticeably higher than other days.So I am consciously trying to reduce the amount of salt especiallyfrom processed foods.” Physical activity “I am getting more regular exercise.”“Increased frequency and intensity of exercise” Practice relaxation “I love to meditate and I found that it had a direct effect on my BP - or seemed to.”“Yoga 3 or 4 times a week” Patients’ awareness of BP control status Realized BP truly uncontrolled “I thought it was better controlled, but realized it was not.”“As a result of the study findings my doctor has added a medication to better control my BP.” Reassured BP controlled “I found out that I do NOT have high blood pressure. When I’m in the clinic it is sky high. When I am at home, it is normal. I’d like to get off my medicine then test it at home to see if I need to stay on the low dose or not.” Recommendations for clinic Arm support while measuring BP at clinic “Second, and relatively easily achievable, providing something for the tested arm to rest on at a correct height while the reading is being taken.” BP measurement at the end of the visit “Don’t take blood pressure reading immediately upon entering the exam room! There is talking, moving around, no chance to sit quietly, and anxiety about the visit. Wait for physician consult to conclude, allow patient 10 minutes to sit quietly, then take the reading. Alternatively, put patient in room for 10 minutes with instructions before taking blood pressure.” Use average of multiple reading for diagnosis “My blood pressure fluctuates within minutes. I do not think you can assess what someone’s average blood pressure reading is by one or two readings. My blood pressure was 109/66 this morning. Just 6 months ago a cardiologist put me on high blood pressure medicine (which made me very sick) because my readings were high in the office. I think doctors need to study their patients’ general health in more detail before issuing these strong medicines.” BP = blood pressure.
Supplemental Appendixes
Supplemental materials
Files in this Data Supplement:
- Supplemental data: Appendixes - PDF file
The Article in Brief
Home Blood Pressure Monitoring in Cases of Clinical Uncertainty to Differentiate Appropriate Inaction From Therapeutic Inertia
Sonal J. Patil , and colleagues
Background Conventional clinic blood pressure measurements are frequently inaccurate, and physicians and patients are often reluctant to intensify hypertension treatment when convinced of falsely elevated readings in clinic. At the same time, clinic readings are routinely used for hypertension diagnosis, management, and physician performance measures. Additionally, there is evidence that BP measured at home, repeatedly, and then averaged provides more accuracy than clinic readings alone.
What This Study Found A pilot study from the University of Missouri concluded that a physician's decision not to intensify hypertension treatment is often a contextually appropriate choice. In two-thirds of cases where physicians did not change treatment for patients with hypertension, patients' blood pressure returned to normal in follow-up readings taken at home. This pre- and post-study tracked 90 patients with hypertension to understand the role that follow-up home blood pressure measures could play in understanding cases of "therapeutic inertia." Sixty-six percent of patients who had a blood pressure reading of 140/90 or higher when they were in the clinic and whose doctors did not change their treatment, had average readings under 140/90 when patients took their blood pressure at home. Additionally, when surveyed after the home blood pressure reading intervention, participants shared that home blood pressure monitoring enhanced their understanding of blood pressure control. Eighty-three percent of participants agreed that they would consider buying a home blood pressure monitor if it was covered by insurance.
Implications
- According to the authors, there are implications for health care quality metrics. Doctors' success rates in controlling hypertension are based solely on clinic blood pressure rates. The authors extrapolated the home blood pressure metrics to show that when home metrics replaced clinical ones, the departmen'�s hypertension control success rates rose from 58% to 86%. They conclude, "Most validated home blood pressure should be accepted and preferred for physician hypertension performance measures."




{kind=link}
{kind=link}