
Abstract
PURPOSE Lesbian, gay, bisexual, and transgender (LGBT) people experience multiple disparities in access to care and health outcomes. We developed a quality improvement initiative, Transforming Primary Care for LGBT People, to enhance the capacity of federally qualified health centers (FQHCs) to provide culturally affirming care for this population.
METHODS The 1-year intervention blended the models of Practice Improvement Collaboratives and Project ECHO (Extension for Community Health Outcomes) to facilitate learning and translate knowledge into action. FQHC teams received coaching in creating LGBT-inclusive environments, collecting sexual orientation and gender identity (SOGI) data, taking risk-based sexual histories, and screening LGBT people for syphilis, chlamydia and gonorrhea, and HIV. We used a preintervention-postintervention evaluation design.
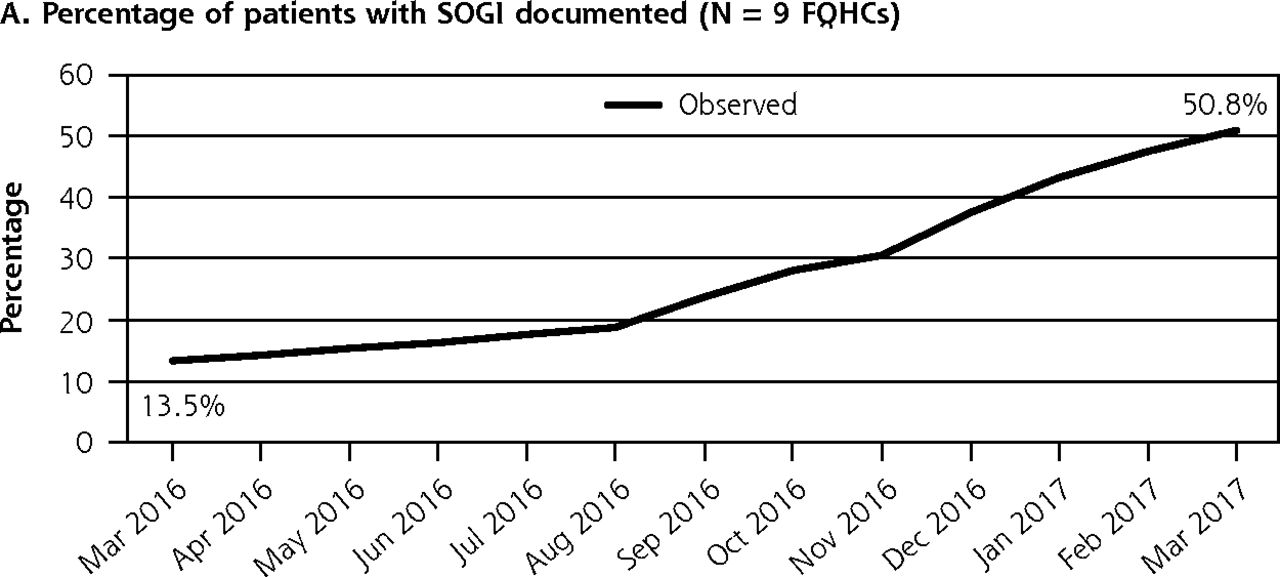
RESULTS We selected 10 FQHCs serving 441,387 patients in 123 clinical sites in 9 states. The intervention spread from 10 clinicians in 10 clinical sites to 431 clinicians in 79 clinical sites. FQHCs reported increases in culturally affirming practices, including collecting patient pronoun information (42.9% increase) and identifying LGBT patient liaisons (300.0% increase). Postintervention, among 9 FQHCs reporting SOGI data from electronic health records, SOGI documentation increased from 13.5% to 50.8% of patients (276.3% increase). Among 8 FQHCs reporting number of LGBT patients, screening of LGBT patients increased from 22.3% (95% CI, 4.9%-40.0%) to 34.6% (95% CI, 19.4%-48.6%) for syphilis (86.5% increase); from 25.3% (95% CI, 7.6%-43.1%) to 44.1% (95% CI, 30.2%-58.1%) for chlamydia and gonorrhea (109.0% increase); and from 14.8% (95% CI, 3.2%-26.5%) to 30.5% (95% CI, 26.7%-34.3%) for HIV (132.4% increase).
CONCLUSIONS FQHCs participating in this initiative reported improved capacity to provide culturally affirming care and targeted screening for LGBT patients.
- sexual orientation
- gender identity
- sexual and gender minorities
- sexually transmitted disease
- cultural competency
- intervention
- quality improvement
- Project ECHO
- Practice Improvement Collaborative
- vulnerable populations
- healthcare disparities
- primary health care
- practice-based research
Although acceptance of diverse gender identities and sexual orientations has increased in recent years,1 people who identify as lesbian, gay, bisexual, and transgender (LGBT) continue to encounter stigma, bias, and discriminatory experiences in their daily lives.2 (In this article, we use the initialism LGBT when referring to the sexual and gender minority population, but recognize that individuals may use a range of terms to describe their sexual orientation and gender identity.) Stress produced by chronic exposure to individual, interpersonal, and structural discrimination adversely influences health behaviors and outcomes for LGBT people. Anti-LGBT stigma also creates barriers to accessing health care, contributing further to health disparities.3–6 Transgender women and gay and bisexual men bear a disproportionate burden of HIV infection and sexually transmitted diseases (STDs), including syphilis and antimicrobial-resistant gonorrhea, compared with non-LGBT populations.7–10 Lesbian and bisexual women and transgender men are less likely to access cervical and breast cancer screening services.11,12 All LGBT subpopulations have documented disparities in smoking, substance use disorders, and psychological distress.6
The Centers for Disease Control and Prevention (CDC) recommends screening sexually active men who have sex with men (MSM) at least annually for HIV, syphilis, chlamydia, and gonorrhea.13 MSM may require extra genital screening depending on exposure, and more frequent screening depending on risk behavior.13 For transgender patients, CDC recommends screening based on current anatomy and sexual practices13; screening for women who have sex with women should be based on a history of sexual risk behaviors.13
Even with national dissemination of CDC guidelines for these populations, recommended STD and HIV screening is not being widely implemented; STDs are increasing among MSM, and HIV is increasing among young black MSM.7,8,14,15 Clinical barriers to screening include lack of time and training.14,16 Clinician bias also plays a role; many LGBT people report delaying medical care to avoid stigma and discrimination.17,18 Clinician discomfort with sexual history taking may be the most important barrier to screening. Despite the need for routine, risk-based sexual health histories to enable targeted HIV and STD screening and treatment, a majority of clinicians do not take comprehensive sexual histories.16,19
Studies also indicate a positive association between clinician knowledge of an LGBT patient’s sexual and gender identity, and the patient’s engagement in care.20–23 Most organizations, however, do not systematically collect sexual orientation and gender identity (SOGI) demographic data, putting the responsibility of disclosure entirely on patients and clinicians.24,25
Capturing SOGI patient data in electronic health records (EHRs) is recommended for informing clinical decision making and enhancing patient-physician communication, as well as monitoring and reducing health disparities.24–26 Uptake has been slow in part because EHRs were not required to have the capacity to collect SOGI data until January 2018.27 LGBT people are also more willing to engage in care and disclose their SOGI with clinicians trained in culturally affirming care, and in clinical environments that intentionally cue inclusiveness (eg, through LGBT rainbow stickers, nondiscrimination policies, and gender-inclusive language). Organizations need information and training to accomplish these changes, however.28,29
In light of these needs, the National Association of Community Health Centers in Washington, DC, the Weitzman Institute in Middletown, Connecticut, and The Fenway Institute, Fenway Health in Boston, Massachusetts, with funding and direct consultation by CDC, developed a national quality improvement initiative called Transforming Primary Care for LGBT People (Transforming LGBT Care). The initiative involved a 1-year intervention to increase culturally affirming primary care for LGBT people accessing federally qualified health centers (FQHCs).
In this article, we describe the preintervention and postintervention quantitative process and outcome data from Transforming LGBT Care. We conclude with implications for future interventions and the potential of such interventions to ultimately achieve health equity for LGBT people. The intervention’s focus on STD and HIV screening was chosen to align with CDC’s goals to reduce transmission among MSM and transgender women; however, the intervention’s larger aims to improve SOGI collection and LGBT culturally affirming primary care were intended to increase care engagement and reduce clinical care disparities among all LGBT populations. Planned future publications will report qualitative findings and cervical cancer, tobacco, and depression screening data.
METHODS
Setting
FQHCs are community-based organizations that receive federal grant funding from the US Health Resources and Services Administration (HRSA) Health Center Program and provide primary care and supportive services to medically underserved and vulnerable populations. In 2016, a total of 1,367 FQHCs were providing care to more than 27 million patients across the United States and territories. About 70% of FQHC patients live at or below the federal poverty guidelines, and about 22% are uninsured.30
Objectives
Transforming LGBT Care was developed by project staff and other expert advisors in LGBT population health, FQHC operations, health information technology, and quality improvement. The primary objectives were for FQHCs to (1) create more LGBT-affirming practice environments to ensure inclusion and safety; (2) improve collection, capture, and reporting of SOGI in the EHR; (3) improve collection, capture, and reporting of risk-based sexual health histories of LGBT patients in order to determine need, frequency, and anatomic sites for STD and HIV testing; and (4) increase the percentage of LGBT patients receiving appropriate STD and HIV screening.
FQHC Selection
In January 2016, project staff and advisors invited 12 FQHCs with a known interest in providing more LGBT-affirming care to respond to a competitive request for proposals. CDC funding allowed up to 10 FQHCs to participate. After careful review by internal and external experts, the 10 successful applicants demonstrated the highest level of commitment from leadership; had the systems necessary to implement the intervention; and agreed to all intervention and evaluation activities. FQHCs did not receive financial compensation for participating, and participation was voluntary.
Intervention Framework and Implementation
Transforming LGBT Care, which took place from March 2016 to March 2017, blended 2 evidence-based models: the Practice Improvement Collaborative31,32 and the Project Extension for Community Health Outcomes (ECHO).33 Both models help care teams apply established guidelines in real-world settings, and overcome barriers to implementation. To our knowledge, this intervention was the first to use these models for LGBT-affirming care, and the first ECHO to focus on a specific population, rather than a medical specialty or condition.
Practice Improvement Collaborative
A Practice Improvement Collaborative promotes systems improvement and implementation of best practices in designated topic areas by bringing cross-disciplinary teams together to learn from each other and from recognized experts. Activities typically involve learning sessions with instruction from experts; rapid cycle testing; and progress updates with coaches and other teams to stimulate further learning. Since 1986, more than 200 improvement collaboratives in hospital and ambulatory care settings, including FQHCs, have addressed diabetes, HIV, asthma, depression, and other conditions. Funding can come from federal agencies, sponsorships, and private foundations.34–36
For Transforming LGBT Care’s Practice Improvement Collaborative, each FQHC formed a team consisting of a quality improvement facilitator, a clinical “champion,” and 2 or 3 additional staff members. Several team members identified themselves or family members as LGBT, and several participated in local LGBT mobilization groups.
Teams received monthly coaching calls with qualified project staff, and accessed free resources from Fenway Health’s training center (www.lgbthealtheducation.org). Early on, teams developed question forms and workflows to determine where, when, and by whom SOGI and sexual behavior questions would be asked. Staff received role-appropriate training at staff meetings and, in real time, wrote scripts for answering patient questions. Several FQHCs had LGBT patient-advisory groups provide input and feedback. Teams also worked closely with information technology staff and EHR vendors to improve SOGI and sexual risk data capture. Each team used plan-do-study-act (PDSA) rapid cycle tests of change with the champion’s patient panel.37 Gradually, teams expanded the intervention’s procedures to additional clinicians and clinical sites within the FQHC, and helped respond when challenges arose.
To increase intervention buy-in from other FQHC staff, teams encouraged administrative leaders and governing board members to announce their support of the intervention to staff; trained all staff on LGBT health disparities and culturally affirming communication; and asked staff for feedback on proposed changes. Community engagement occurred through outreach coordinators and collaboration with local LGBT organizations.
Cross-FQHC collaborative learning took place through 2 in-person and 3 videoconference learning meetings; sharing of monthly reports of accomplishments and barriers; and contributing of questions and resources to a web-based platform.
Project ECHO
Project ECHO is a guided-practice knowledge-sharing model in which clinical specialist teams tele-mentor community clinicians in underserved areas through free videoconferencing software. Since 2003, there have been more than 40 ECHO programs on diverse conditions, including hepatitis C, pain management, diabetes, and substance use disorders. ECHO sessions typically have 15 to 20 participants, and run weekly to monthly for 2 hours. FQHCs may use HRSA grants to participate in ECHOs; private foundations also support ECHOs.38,39 Transforming LGBT Care’s ECHO mentored primary care and behavioral health clinicians in providing high-quality, informed, and affirming care to LGBT patients. Twice-monthly sessions facilitated by a multidisciplinary expert clinical team comprised brief didactic presentations followed by participant-led case consultation. ECHO sessions both enhanced and reinforced the practice improvement collaborative by focusing on STD and HIV screening, as well as other critical LGBT health topics, such as caring for youth and older adults, prescribing preexposure prophylaxis, screening for cervical cancer, and providing gender-affirming hormone therapy. A complete list of ECHO topics and an intervention timeline is given in Supplemental Appendix 1 (available at https://www.AnnFamMed.org/content/18/4/292/suppl/DC1/).
Data Collection and Evaluation
The Community Health Center, Inc Institutional Review Board reviewed and granted an exemption to conduct a program evaluation of this intervention.
Sociodemographic and Participation Data
Aggregate data on patient sociodemographic characteristics were obtained from HRSA’s 2016 Uniform Data System, an annual reporting system for tracking FQHC demographics, diagnoses, and services.30 Participation by FQHC sites and clinicians in intervention activities was recorded and tracked by project staff.
Implementation Science Framework
The intervention’s evaluation design was based on the Learning Evaluation Framework, a methodologic approach that blends quality improvement with implementation research methods to study health care innovations in primary care.40 The approach involves collecting standardized qualitative and quantitative process and outcome data within and across organizations, and providing feedback to organizations to encourage further improvement. For Transforming LGBT Care, all FQHCs received training and tools to capture quantitative data on screening and qualitative data on barriers and facilitators to implementation. Each team shared monthly data and progress reports with project staff and other teams to provoke insights and change.
Practice Assessment Survey
Project staff developed the practice assessment survey, a novel 27-question (93-item) questionnaire that assessed the intensity of FQHC practices in providing culturally affirming environments and systems of care for LGBT patients (Supplemental Appendix 2, available at https://www.AnnFamMed.org/content/18/4/292/suppl/DC1/). Senior clinical leaders at each FQHC completed the questionnaire at baseline and at the end of intervention. For evaluation purposes, we aggregated the data from all FQHC assessments; however, centers also received their own reports of assessment findings for self-reflection and planning. Survey data were analyzed using Stata, version 15 (StataCorp LLC).
Core Clinical Outcome Data
The core clinical measures are defined in Table 1. For each month of the intervention, FQHCs submitted deidentified and aggregated core clinical data on patients aged 13 years and older. For improved data integrity, FQHCs received coaching from project staff and resubmitted cleaned and corrected monthly data at the end of the intervention.
Core Clinical Outcome Measures
FQHCs were instructed to count patients as LGBT who identified their sexual orientation as “lesbian/gay” or “bisexual,” and/or their gender identity as “transgender man” or “transgender woman.” Some FQHCs also may have included patients who identified their sexual orientation as “something else” or their gender identity as “other.” Experts recommend collecting gender identity along with sex assigned at birth to best identify transgender people.41 This 2-step method makes it possible to identify as transgender anyone whose reported gender identity and sex assigned at birth do not correspond. Although the FQHCs collected sex assigned at birth, their EHRs could not extract and compare these data with gender identity. We were therefore unable to use the 2-step method for this analysis.
Core Clinical Analysis
SOGI documentation is necessary for identifying LGBT patients for screening. But because the intervention implemented SOGI documentation simultaneously with (rather than before) targeted STD and HIV screening, it was not possible to accurately count LGBT patients in the first months of the intervention. To evaluate improvements in STD and HIV screening over time, we therefore estimated the number of LGBT patients in the denominator by using an imputation method similar to the back-calculation approach customarily used to estimate HIV infections in a population that includes unknown (untested) cases.42–44 First, we observed that the total patient population of the FQHCs increased by an average of 1.5% per month during the intervention period. Next, we assumed that the rate of growth for LGBT patients was also 1.5%, and that the last month of the intervention provided the closest approximation of the actual LGBT patient population. We then back-calculated the LGBT denominator for all previous months, assuming the 1.5% monthly increase rate. LGBT patients were counted as screened for STDs and HIV even if their LGBT identity was not captured in the EHR at the time of screening. To assess significance of the estimates, we computed 95% CIs. The Supplemental Appendix 3 (available at https://www.AnnFamMed.org/content/18/4/292/suppl/DC1/) further explains the imputation method and assumptions.
Qualitative Data
Qualitative data included transcripts of mid-intervention interviews with FQHC teams and leadership, narrative progress reports, and FQHC presentations of lessons learned. For this article, qualitative data were used to provide context to the quantitative outcomes assessed before and after the intervention. A planned future publication will analyze qualitative data to determine facilitators and barriers to implementation. In addition, the Supplemental Appendix 4 (available at https://www.AnnFamMed.org/content/18/4/292/suppl/DC1/) provides intervention implementation tips and change ideas gleaned from the qualitative data.
RESULTS
Health Center Characteristics
The FQHCs participating in Transforming LGBT Care were located in rural and urban areas of the United States. Two were in Arizona; the other 8 were in California, Colorado, Connecticut, Louisiana, Michigan, North Carolina, Pennsylvania, and Texas. In total, the FQHCs served 441,387 unique patients at 123 clinical sites during calendar year 2016 (Supplemental Appendix 5, available at https://www.AnnFamMed.org/content/18/4/292/suppl/DC1/). Five FQHCs had a majority of Hispanic/Latino patients, 1 had a majority of black/African American patients, and 9 served patients experiencing homelessness. The mean percentage of adult patients (aged 18 years and older) was 71.6% (percentage of patients aged 13 years and older was not available).
FQHC Participation and Spread
FQHC teams had 100% participation in the coaching calls and learning meetings. Clinical teams attended 21 of 24 Project ECHO sessions (median = 23; range, 12 to 24) on average, and presented 65 cases total. An additional 9 FQHC teams joined the ECHO sessions but did not participate in other aspects of the intervention. Family practice clinicians comprised one-third of FQHC champions and two-thirds of ECHO participants.
The intervention expanded from 10 clinicians at 10 clinical sites (ie, 1 clinician at 1 clinical site per FQHC), to 431 clinicians at 79 clinical sites, although adoption varied greatly among FQHCs (Table 2).
Spread of the Transforming Primary Care for LGBT People Intervention Among FQHC Clinicians and Clinical Sites, 2016-2017
Culturally Affirming Practices
FQHCs reported improvements in LGBT culturally affirming training, practices, policies, and systems (Table 3). Percentage increases in the percentage following various practices were greatest for asking all patients SOGI questions (350% increase), having a staff member identified as an LGBT liaison or navigator for clients (300% increase), and training of all new hires in the behavioral health needs of LGBT clients (200% increase).
Key Findings of the Practice Assessment Survey, 2016-2017 (N = 10 FQHCs)
Core Clinical Outcomes
All FQHCs modified their workflows and EHRs to collect SOGI data. One FQHC (FQHC 8), however, could not capture SOGI data in their EHR until the end of the intervention, and was therefore excluded from core clinical data analyses. This FQHC reported initial staff resistance, a need for patient education and Spanish translations of questions, leadership turnover, competing priorities, and difficulty with implementing SOGI data fields into the EHR. Among the remaining 9 FQHCs, SOGI documentation increased from 23,835 patients (13.5%) to 104,583 patients (50.8%) over the intervention period, an increase of 276.3% (Figure 1 and Supplemental Appendix 6, available at https://www.AnnFamMed.org/content/18/4/292/suppl/DC1/).

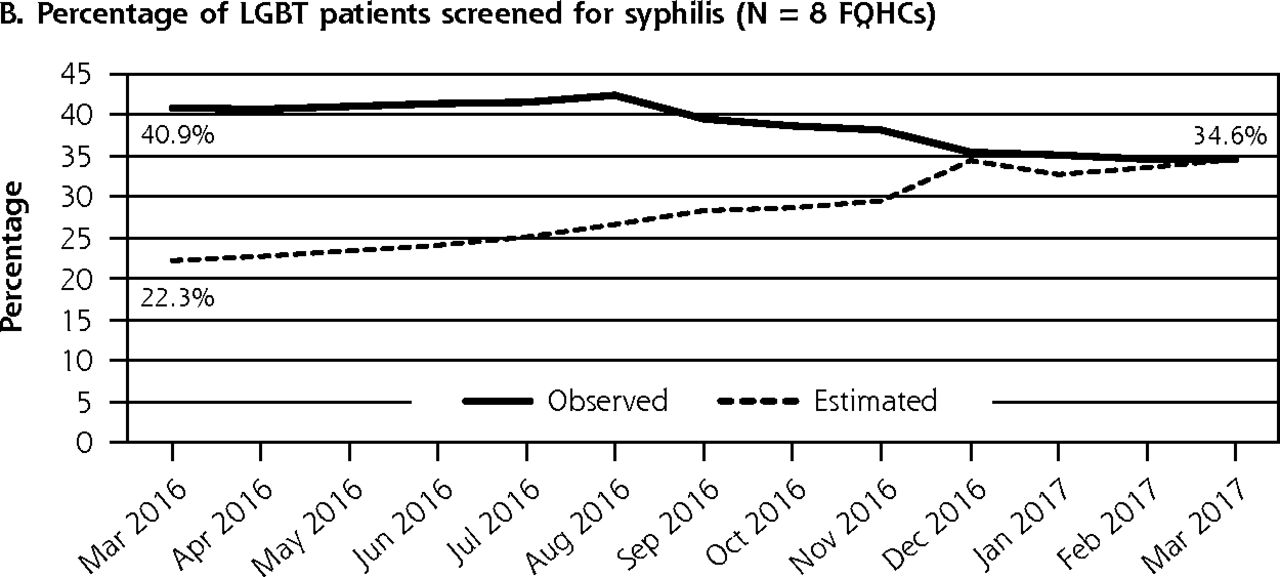
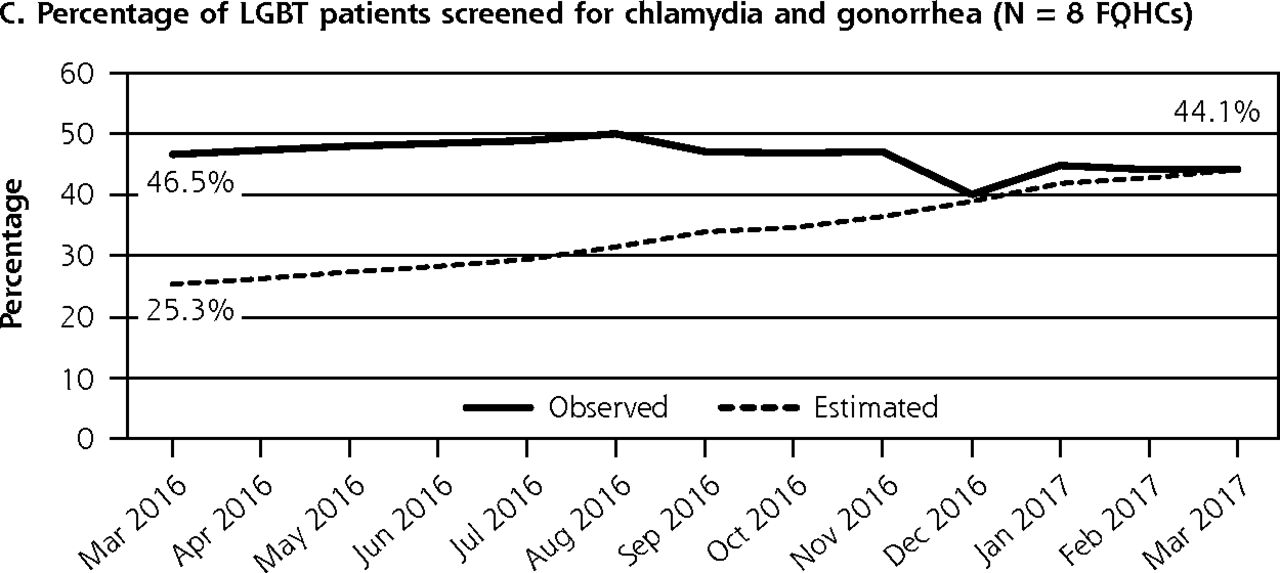
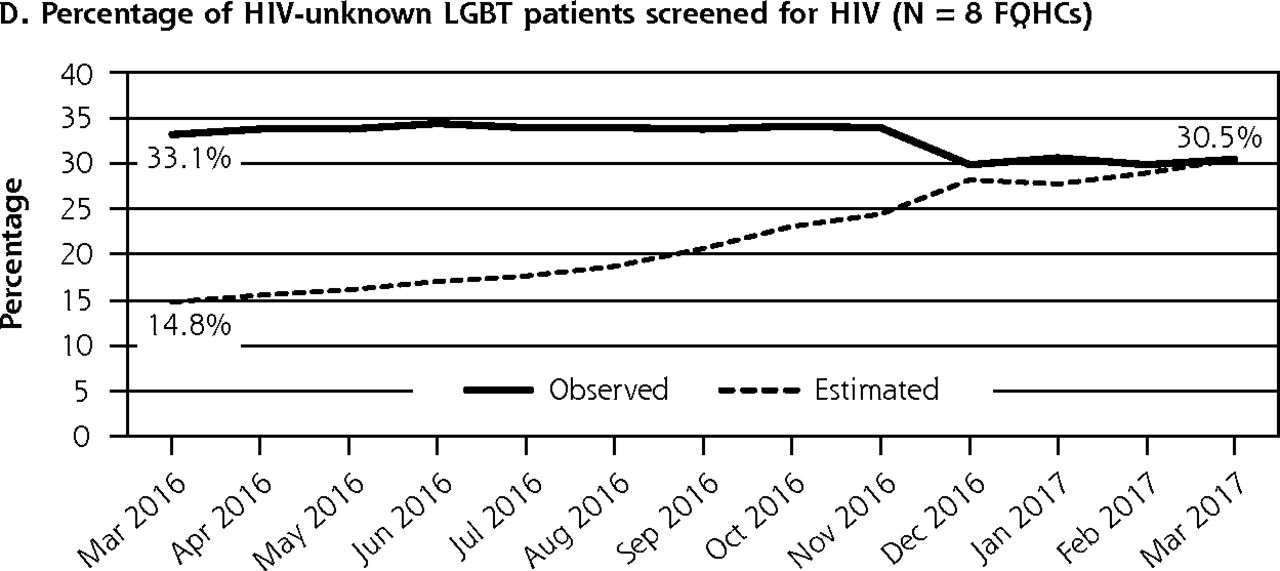
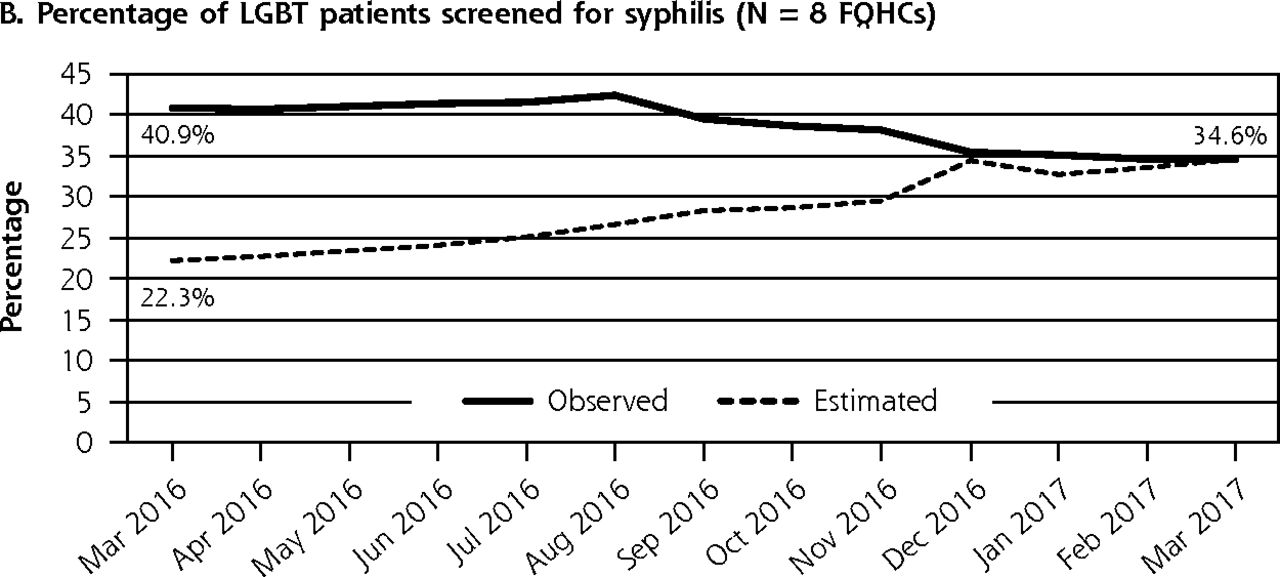
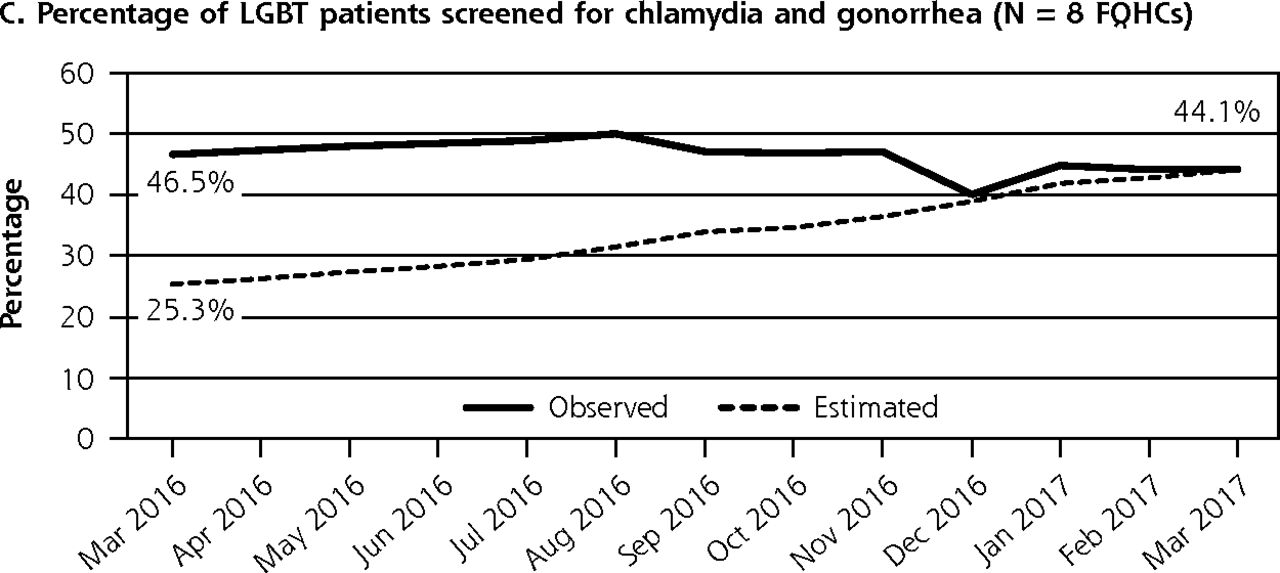
Core clinical outcomes from the Transforming Primary Care for LGBT People intervention, 2016-2017.
FQHC = federally qualified health center; LGBT = lesbian, gay, bisexual, and transgender; SOGI = sexual orientation and gender identity.
An additional FQHC (FQHC 6) lacked the necessary support from its EHR vendor and information technology staff to extract SOGI data from the EHR, and therefore could not report the number of LGBT patients. Of the patients in the other 8 FQHCs, 7,468 (7.6%) identified as LGBT. Among LGBT patients, the estimated percentage screened for syphilis increased from 22.3% (95% CI, 4.9%-40.0%) to 34.6% (95% CI, 19.4%-48.6%), an increase of 86.5%; the estimated percentage screened for chlamydia and gonorrhea increased from 25.3% (95% CI, 7.6%-43.1%) to 44.1% (95% CI, 30.2%-58.1%), an increase of 109.0%. Among HIV-unknown LGBT patients, the estimated percentage screened for HIV increased from 14.8% (95% CI, 3.2%-26.5%) to 30.5% (26.7%-34.3%), an increase of 132.4%.
With regard to risk-based sexual health screening of LGBT patients, 6 FQHCs reported improvements in screening, but 2 FQHCs could not implement screening. FQHC teams recognized the need for more time to develop cultural humility45 among clinicians—that is, increase their openness to aspects of LGBT cultural identity—before screening. Other FQHCs agreed that creating a more culturally affirming clinical environment through training staff in LGBT terms, concepts, and health disparities helped them with successfully collecting SOGI data and providing risk-based sexual health screening. Ultimately, because all FQHCs encountered challenges with capturing sexual risk information in structured formats within EHRs, we were unable to report these data.
DISCUSSION
Key Findings
Ambitious in mission and scope, Transforming LGBT Care brought together 10 geographically dispersed FQHCs to participate in an intensive 1-year intervention. The project was groundbreaking not only in its focus on LGBT health care, but also in its unique design incorporating Practice Improvement Collaboratives and Project ECHO. To our knowledge, this is the first published report of a national quality improvement collaborative focused on culturally affirming care for LGBT people, and the first Project ECHO to focus on a population instead of a disease, disorder, or medical specialty.
The strengths of Transforming LGBT Care were the reported performance improvements in SOGI documentation, targeted STD and HIV screening of LGBT patients, and LGBT culturally affirming practices and policies. These accomplishments are impressive given the short timeframe, lack of funding for participating FQHCs, and typical challenges encountered by primary care sites in implementing new systems and guidelines, and in modifying EHRs.14–16
FQHC teams demonstrated a strong commitment to the initiative by participating in nearly all intervention activities. Consistent with other interventions focused on translating knowledge into practice, selecting FQHCs based on leadership commitment, and engaging members of the LGBT community, may have set the stage for success.46–48 High participation may also have been facilitated by using web-based technologies to support collaborative learning, rather than multiple in-person meetings that have been a characteristic of other collaboratives.49
External forces likely influenced the intervention results. For example, cultural shifts in attitudes toward LGBT people, along with policies regarding LGBT people, may have affected staff buy-in and patient willingness to disclose.50 Notably, in March 2016, HRSA began requiring FQHCs to collect and report annual aggregated SOGI data on all adult patients (aged 18 years and older). Although the equivalent timing of Transforming LGBT Care was coincidental, the mandate likely made a large impact on the FQHCs’ motivation and performance. An analysis of the 2016 Uniform Data System found that 22.9% and 37.2% of all patients in HRSA-funded health centers had their sexual orientation and gender identity documented, respectively.51 These percentages are lower than the 50.8% of patients with SOGI documentation in the 9 Transforming LGBT Care FQHCs by March 2017; however, only 37.5% of patients in these centers had their SOGI documented by December 2016.
A challenge for the FQHCs was conducting and capturing risk-based sexual health screening. This finding is not surprising given the many documented barriers among clinicians in sexual history taking.16,20,52 Clinicians also encounter considerable difficulties when implementing any new guidelines or techniques to improve population health.53 Such barriers can have a ripple effect. For example, clinicians may find it easier to universally screen all LGBT people based on identity alone, rather than provide targeted screening according to the specific sexual practices (such as exposure site) according to CDC guidelines. In our intervention, although we estimated an increase in HIV and STD screening, our data did not tell us which screenings were based on specific sexual practices and exposure sites. Within the arena of primary care, there may still be a role for specialty clinics that focus almost exclusively on LGBT, sexual health, or both, and use clinicians who have more skills and training in taking sexual risk assessments. With regard to EHRs, vendors can provide more flexibility to modify patient characteristic fields and can consider creating structured sexual history data capture fields with STD testing decision support.
A planned future article analyzing qualitative data from Transforming LGBT Care will shed more light on the facilitators and barriers experienced by FQHCs, will help explain how each element of the intervention contributed to observed improvements, and will interpret the value of blending a Practice Improvement Collaborative with Project ECHO. Additionally, an analysis of 5 FQHCs that used SOGI data to assess for disparities in other primary care LGBT health care services (eg, depression, tobacco, and cervical cancer screening) is also being prepared for publication.
Limitations
Because this was a quality improvement project assessing outcomes before and after the project, without a control group, it is not possible to infer a causal relationship between the intervention and the increase in screening. In addition, we did not collect data on non-LGBT patients and do not have access to screening data in other FQHCs; therefore, we could not compare trends in STD screening. Moreover, the participating FQHCs were carefully selected and motivated to create change; therefore, the intervention may not be generalizable to FQHCs without these characteristics. Future intervention research should consider using control groups, making comparisons with non-LGBT patients, and reducing selection bias. Additionally, a longer follow-up period would allow researchers to measure improvements in health outcomes for LGBT patients, which is the ultimate goal of the intervention.
Another limitation is the practice assessment survey, which was a novel questionnaire that had not been tested for validity or reliability. Assessment findings were also subject to response bias, because FQHC staff who completed the questionnaire may have had an interest in demonstrating success. In addition, the assessment measured the intensity of standardized processes more than the level of standardization. Future assessments would benefit from reliability and validity testing as well as collection of data less prone to bias. Moreover, when measuring cultural affirmation, it is important to ask patients directly about their experiences, which we were not able to do in this iteration of the intervention.
The core analyses also had limitations. To estimate STD and HIV screening percentages, we used imputation and back-calculation to replace missing SOGI data. The imputation, however, did not account for the likelihood that some patients, such as adolescents, may have begun to identify as LGBT during the intervention year, leading to a small increase in the number of LGBT patients. In addition, the analysis did not account for churn (ie, patients who left the clinic over the year).
The analysis also counted LGBT patients as screened for HIV and STDs, even if their LGBT identity was not captured in the EHR until after the time of screening. Moreover, because of issues with EHR functionality, lesbian and bisexual women, and transgender men were included in the STD and HIV screening denominators. Neither of these populations have a known increased risk for these diseases, and therefore are less likely to need annual screening.13 With recent improvements in EHR capacity, FQHCs should now or soon be able to stratify the screening data by gender identity and sex assigned at birth in order to determine STD and HIV screening percentages specific to the higher risk groups of MSM and transgender women.
Further, the number of observed LGBT patients is likely an underestimate for several reasons. First, we do not know if the FQHCs included people as LGBT who self-identified their sexual orientation as “something else,” or their gender identity as “other” or “genderqueer.” Second, because FQHCs could not use the 2-step method to identify transgender people, they likely did not include several transgender people in the count. Third, some LGBT people may not have disclosed their SOGI due to concerns about discrimination. This may not be a large number of people, however; LGBT patients are more likely to answer SOGI questions compared with non-LGBT people.52,54
Implications
The FQHCs that participated in the intervention currently report efforts to sustain its positive effects. They continue to collect and track SOGI data, receive leadership support, and form committees. At least one has reported its LGBT population has grown. Some are furthering their education in transgender care and expanding LGBT-affirming practices into dental and recovery programs.
The willingness of FQHCs to actively participate in a time-intensive intervention without financial compensation suggests that this type of intervention is desirable and holds promise for national replication in other FQHCs or other primary care organizations with a strong commitment to improving LGBT health care. Future interventions may consider using a longer time period to implement a 4-phase process: (1) raise staff awareness and develop culturally affirming practices; (2) install SOGI documentation and data capture within structured EHR fields; (3) implement risk-based sexual health screening and data capture; and (4) use SOGI and risk-based screening to identify for whom, where, and how frequently STD and HIV screening is needed. Fortunately, EHR systems certified under the US Meaningful Use Stage III incentive program are now required to record SOGI data, making capture and extraction of these data more feasible.27
Those wishing to replicate the intervention on a large scale may need access to a similar type of expertise and infrastructure offered in Transforming LGBT Care. Alternatively, future interventionists may be able to create sized-down adaptations of the intervention, where small cohorts arrange peer-to-peer learning through free or low-cost videoconferencing software.
Ultimately, FQHCs and other primary care organizations have an opportunity and a responsibility to provide equitable care to people of all sexual orientations and gender identities. Even small changes to health care practices may make a large difference for people burdened by health disparities and discrimination. Further efforts, such as improving SOGI data capture in EHRs, and supporting primary care clinicians in taking more comprehensive sexual histories, are necessary for sustainable and wide-reaching change.
Larger-scale implementation of interventions similar to Transforming LGBT Care that focus on creating culturally affirming care environments alongside improvements in sexual health care have the potential to greatly advance health outcomes for LGBT communities. Early detection and treatment of HIV and STDs benefits individual health as well as public health by decreasing transmission risk. Better methods of sexual history taking and increased awareness of sexual and gender diversity can also potentially improve how clinicians interact with non-LGBT patients around sexual and reproductive health care. Finally, developing more inclusive and culturally affirming environments can increase LGBT engagement in health care, and eventually lead to better overall health and well-being.
Acknowledgments
We would like to acknowledge Russell Brown, Kathleen McNamara, and Ashley Barrington of the National Association for Community Health Centers, and Rodney VanDerWarker of Fenway Health, for their management of the writing of this article, for providing guidance and oversight before and during the intervention, and for their commitment to LGBT health equity. We would also like to acknowledge Emil Coman, PhD, PSTAT of the Weitzman Institute, Community Health Center, Inc, for his assistance with data analysis. And, finally, we would like to give a huge shout out to all of the Project ECHO staff!
Footnotes
Conflicts of interest: authors report none.
To read or post commentaries in response to this article, see it online at https://www.AnnFamMed.org/content/18/4/292.
Funding support: This work was supported by grant 6 NU38 OT00 02 23-05-03 from the Centers for Disease Control and Prevention.
Disclaimer: The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Prior presentations: Addressing the Health of LGBT People through Public Health & Primary Care Collaboration, Michigan LGBT Health Summit, Bay City, MI, Jun 13, 2016; Addressing the Health of LGBT People through Public Health & Primary Care Collaboration, Transforming Care: Midwest Conference on LGBTQ Health Equity and HIV/AIDS, Columbus, OH, Oct 21, 2016; Transforming Primary Care for LGBT People, 2016 National Coalition of STD Directors (NCSD) Annual Meeting, Phoenix, AZ, Dec 8, 2016; Transforming Primary Care for LGBT People, 2016 STD Prevention Conference, Atlanta, GA, Sep 20-23, 2016; Transforming Primary Care for LGBT People, 2017 Michigan STD & HIV Conference, Ann Arbor, MI, Aug 8, 2017; Transforming Primary Care for LGBT People, SYNChronicity 2017: The National Conference for HIV, HCV & LGBT Health, Arlington, VA, Apr 24-25, 2017; Improving Primary Care for LGBT People Through the Implementation of Sexual Orientation and Gender Identity Data Collection at FQHCs, 2017 Community Health Institute (CHI) & Expo, San Diego, CA, Aug 27-29, 2017; Dissemination and Implementation of Sexual Orientation and Gender Identity Data Collection in Federally Qualified Health Centers, 2017 APHA Annual Meeting & Expo, Atlanta, GA; Nov 4-8,2017; Outcomes of Implementing Sexual Orientation and Gender Identity (SOGI) Data Collection at Federally Qualified Health Centers, 2017 45th NAPCRG Annual Meeting, Montreal, Quebec, Canada, Nov 17-21, 2017; Using Quality Improvement Measures to Monitor and Assess Practice Transformation; Transforming Primary Care for LGBT People, 2018 STD Prevention Conference, Washington, DC, Aug 27-30, 2018.
Supplemental materials: Available at https://www.AnnFamMed.org/content/18/4/292/suppl/DC1/.
- Received for publication June 17, 2019.
- Revision received October 31, 2019.
- Accepted for publication November 11, 2019.
- © 2020 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Closing the gap on healthcare quality for equity-deserving groups: a scoping review of equity-focused quality improvement interventions in medicine
- A realist review of how, why, for whom and in which contexts quality improvement in healthcare impacts inequalities
- Qualitative inquiry into barriers and facilitators to transforming primary care for lesbian, gay, bisexual and transgender people in US federally qualified health centres