
Article Figures & Data
Figures
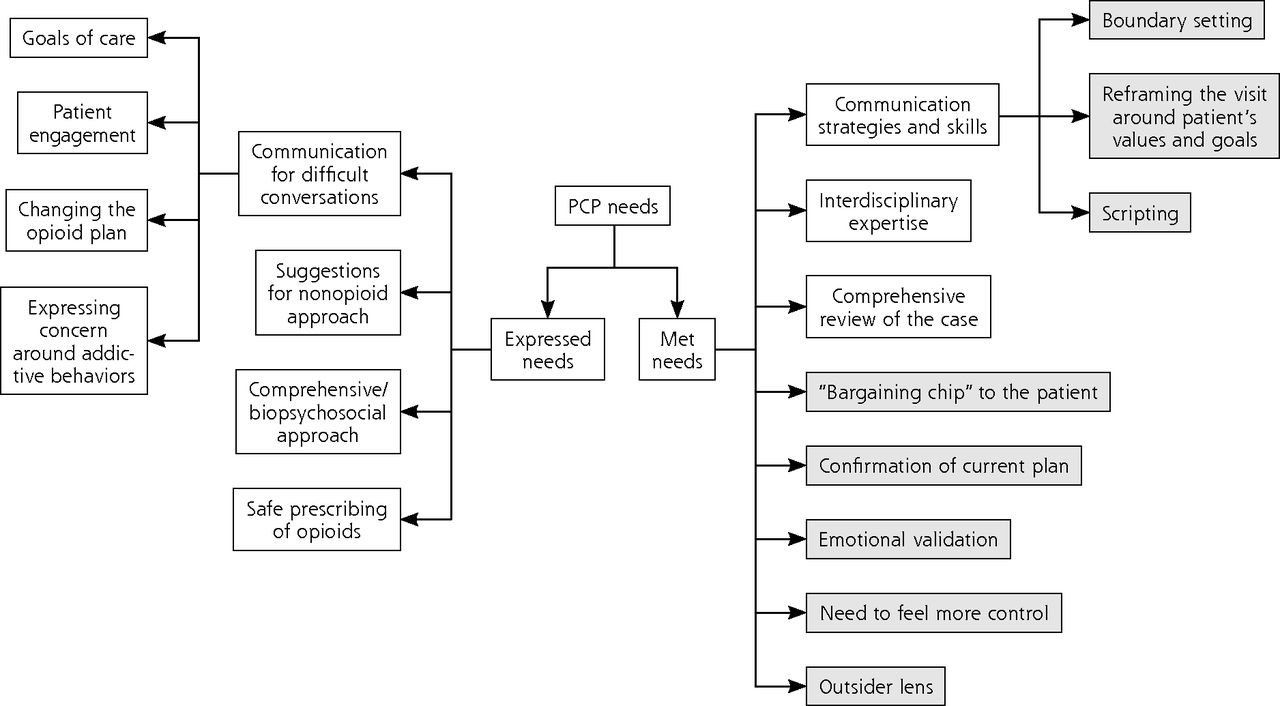
- Figure 1.
Heuristic map of results.
PCP = primary care provider.
Note: Shading indicates a need that was identified only after the consultation and was not listed in the expressed needs for the referral.

Tables
Expressed Need Description Exemplar Quote Safety in prescribing opioids PCPs requested guidance around the safety in prescribing opioid analgesics as it relates to dosing and medication choice; performing a benefit vs risk assessment (as it relates to the patients’ other medical and psychological comorbidities and other prescribed medications); approach to tapering; and managing acute-on-chronic pain flares. “Is it appropriate to continue the patient’s current pain regimen unchanged? [This patient] is very functional on this regimen, but there are concerns about its safety as he ages and some intermittent aberrant drug testing, early refill requests, and hx of overdose in the year 2015.” (RefQ1) Communication for difficult conversations PCPs requested consultation guidance on navigating conversations related to patients’ goals of care, and how to engage patients and promote self-efficacy in their treatment plan particularly around nonopioid options and when changing the opioid plan or tapering, particularly connected to expressing their concern for addictive behavior. “This patient has not been interested in engaging in conversation about her regimen, her pain management, or pretty much anything else. She wants to see us as little as possible and get her medications. How do I approach that? How do I engage her? Or do I put up firmer lines if she stays unengaged?” (RefQ14) Suggestions for nonopioid approaches PCPs requested guidance in offering nonopioid approaches to pain management, including both pharmacologic and nonpharmacologic options, in patients with or without known substance use disorders. “What are other nonopioid therapies I can use in this patient [with fibromyalgia] to improve pain control?” (RefQ33) Comprehensive/biopsychosocial approach PCPs sought guidance on creating a plan in partnership with their patients that included addressing underlying psychological comorbidities that affect their chronic pain and/or addiction. “Do I make engagement with CHA Psych a condition of ongoing buprenorphine prescribing? Most importantly: I think part of the problem here is that she does not acknowledge the role of her mental health situation and opiate dependence in furthering her chronic pain—she continues to look for a physical cause of her pain, to focus on that, and to focus on oxycodone as ‘the only thing that helps.’” (RefQ23) CHA Psych = Cambridge Health Alliance Department of Psychiatry; hx = history; PASS = Pain & Addiction Support Services; PCP = primary care provider; RefQ = referral question.
Met Need (No. of PCPs Identifying Need) Description Exemplar Quote “Bargaining chip” to the patient (11 PCPs) PCPs expressed a need to take ownership of the decisions off themselves to some degree. Using the PASS consultation service as a way to externalize the decision-making process allowed them to maintain their relationship with the patient to help increase patient buy-in and collaboration with the patient. “And so looking for additional—like I said, I think the biggest thing was that bargaining chip with the patient. I needed something that could take the pressure off of me in making this decision around whether she should be prescribed opiates or not.” (P1) Communication strategies and skills (13 PCPs) PCPs needed PASS to help with boundary setting, patient engagement with/buy-in for nonpharmacologic treatment options or any change in the treatment plan, and a reframing of the visit that focused on the patient’s function, values, and goals. “...or the young lady who I wasn’t so sure she should be on opioids, they talked about how to drill down to what her priorities are, and how you might frame it as, like, ‘I do really want to help you with your pain. I’m not sure that the pain is ever going to go away completely, but you know, I’m wondering what would feel good to you in terms of your quality of life, if we were able to get the pain decreased? What would you be able to do, what are your goals?’ And so, trying to frame it in more of that strength-based approach, rather than, ‘These medicines are dangerous. You need to get off of them.’ (P11) Comprehensive review of the case (12 PCPs) PCPs appreciated the chance to both (a) go through the referral process itself, which gave them time and space to think about the case, clarify their own needs as they prepared for the meeting, and talk through ambiguity in the case; and (b) hear an outside team’s comprehensive summary of the case. “It was very helpful. I think the great thing was that [PASS member] always starts off with doing a summary, based on a very intensive chart review, to get everybody on the same page about what this case is about. Which I think works beautifully, because it’s also helpful for me to see what an outsider who’s reviewing the chart is taking away from all our massive documentation and notes and everything like that. And I think, in this particular case, she captured probably 90% of the essence of the patient, which I was very happy about. Because it was a very complicated patient.” (P5) Confirmation of current plan (13 PCPs) PASS helped reinforce PCPs’ decision that they were leaning toward before the consultation. PCPs had trepidation about changing the plan at times, and they felt their need was met when PASS said they were on the right track or validated their assessment and/or treatment plan. “So it was useful just in backing up what I thought needed to happen...” (P10) Emotional validation (13 PCPs) PCPs expressed needing an acknowledgment of how difficult and/or complex the case was so they did not feel so alone with a challenging case. This included validation of complexity of the case and feeling a sense of relief in discussing the case with the PASS team. “I think it’s also been helpful to have a group of folks review the case and also validate the feelings that this is a really tough situation. And there’s no one great answer to things. And also just feeling like, okay, I’m not alone in feeling overwhelmed with this patient. So I think that’s all been helpful.” (P5) Interdisciplinary expertise (14 PCPs) PCPs needed to take a more global, biopsychosocial approach to management. They also needed specific knowledge and resources that they may not have including approaches to chronic pain management, assessment of potential underlying OUD, opioid dosing and tapering, nonopioid pharmacologic options, and other treatment options. “It wasn’t just physicians on the PASS team. There were— there’s a social worker, and a behavioral therapist. There’s so many different perspectives. And having each person’s input, and saying, ‘We’re available to do these kinds of things for pain,’ it was helpful to know what kind of resources they had that were beyond what we normally think of in primary care.” (P4) Need to feel more control (13 PCPs) PCPs experienced feeling “stuck” with patients after exhausting all options. At times, PCPs held mistrust of the patient and needed help with managing complications with the health care system. This was especially true for legacy patients (“inherited patients”) whose plan was set before the PCP assumed his/her role. As a result, PCPs were looking for a concrete plan with specific recommendations from PASS. “It kind of felt like Groundhogs Day where I was—we were saying kind of the same thing over and over, and he was still resisting over and over. And I felt like I really wasn’t going anywhere for multiple visits at a time. That I was like ‘Okay, this is not productive for either of us. So I feel like we need to kind of get this from a different angle.’” (P4) Outsider lens (11 PCPs) PCPs needed a new perspective on the case from clinicians not currently immersed in the patient’s care. They stated that they valued an outsider perspective that incorporated multiple angles when doing a case review. “I think, well, part of it was just to have someone else look at the picture..., because you’re so involved in that case that you’re not sure if you’re just making things up or not.” (P8) OUD = opioid use disorder; PASS = Pain & Addiction Supportive Services; P = participant; PCP = primary care provider.
The Article in Brief
Multidisciplinary Approach for Managing Complex Pain and Addiction in Primary Care: A Qualitative Study
Randi G. Sokol , and colleagues
Background Between 11% to 40% of adults in the U.S. experience chronic pain, and primary care physicians may feel ill-equipped to effectively and safely care for patients with chronic pain, addiction or both.
What This Study Found Researchers from Tufts University conducted a study to evaluate the effectiveness of an interdisciplinary consultation service that supports primary care physicians (PCPs) who care for patients experiencing chronic pain and addiction. The goal was to identify new and effective strategies that clinics can use to support PCPs.
From that interdisciplinary consultation service, the researchers collected and thematically analyzed 66 referral questions and 14 interviews with PCPs to better understand the types of support physicians would find most beneficial.
PCPs’ expressed needs included needing expertise in addiction, safe prescribing of opioids, non-opioid treatment options, communication strategies for difficult conversations, a comprehensive review of the case, and a biopsychosocial approach to management. Some additional needs were identified after interviews, including confirmation of their medical decision-making process, emotional validation, feeling more control, having an outside entity take the burden off the PCP for management decisions, boundary setting, and reframing the visit to focus on the patient’s function, values, and goals.Implications
- An interdisciplinary consultation service can effectively support primary care physicians who care for patients battling pain and addiction. The authors offer potential strategies that health systems can use to support PCPs in caring for patients living with chronic pain and addiction.




{kind=link}