
Article Figures & Data
Figures
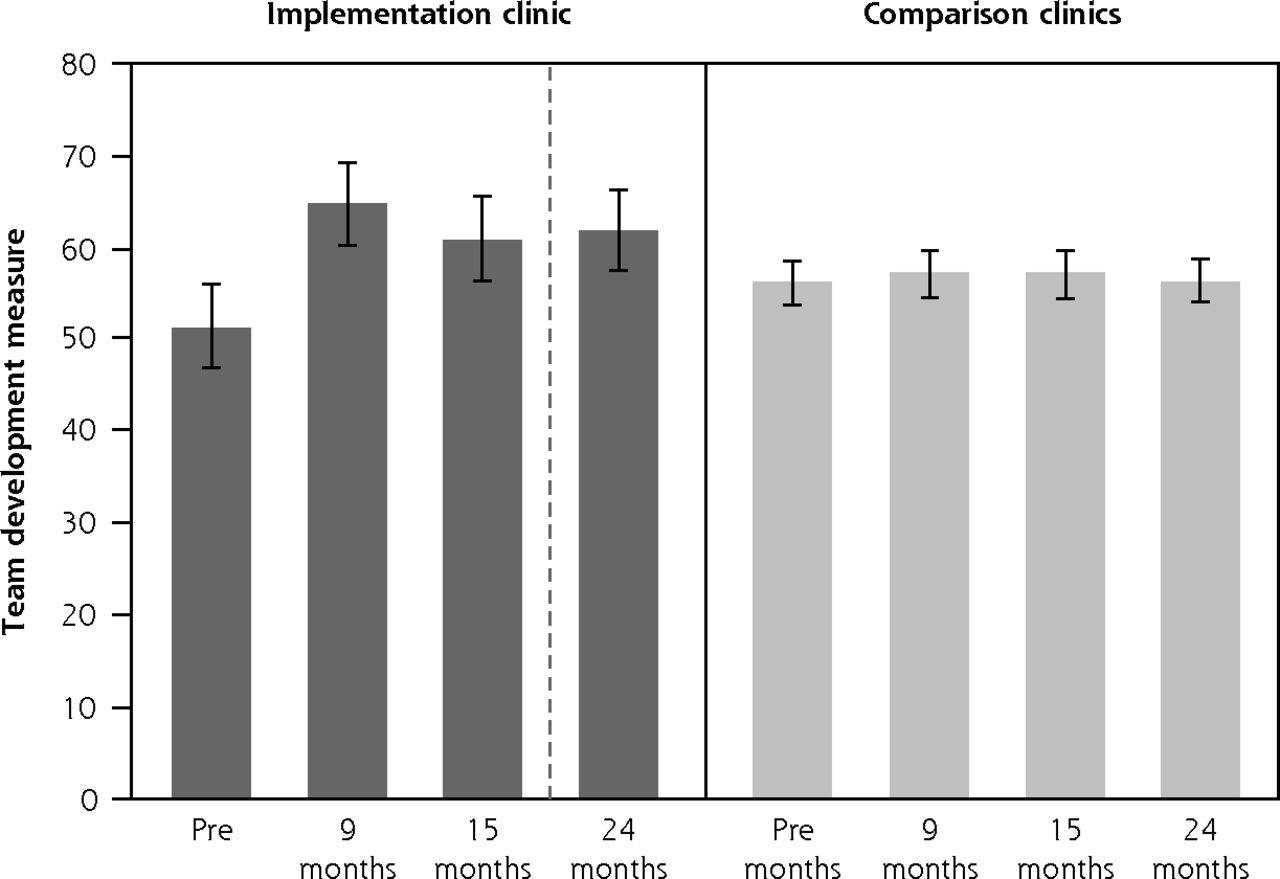
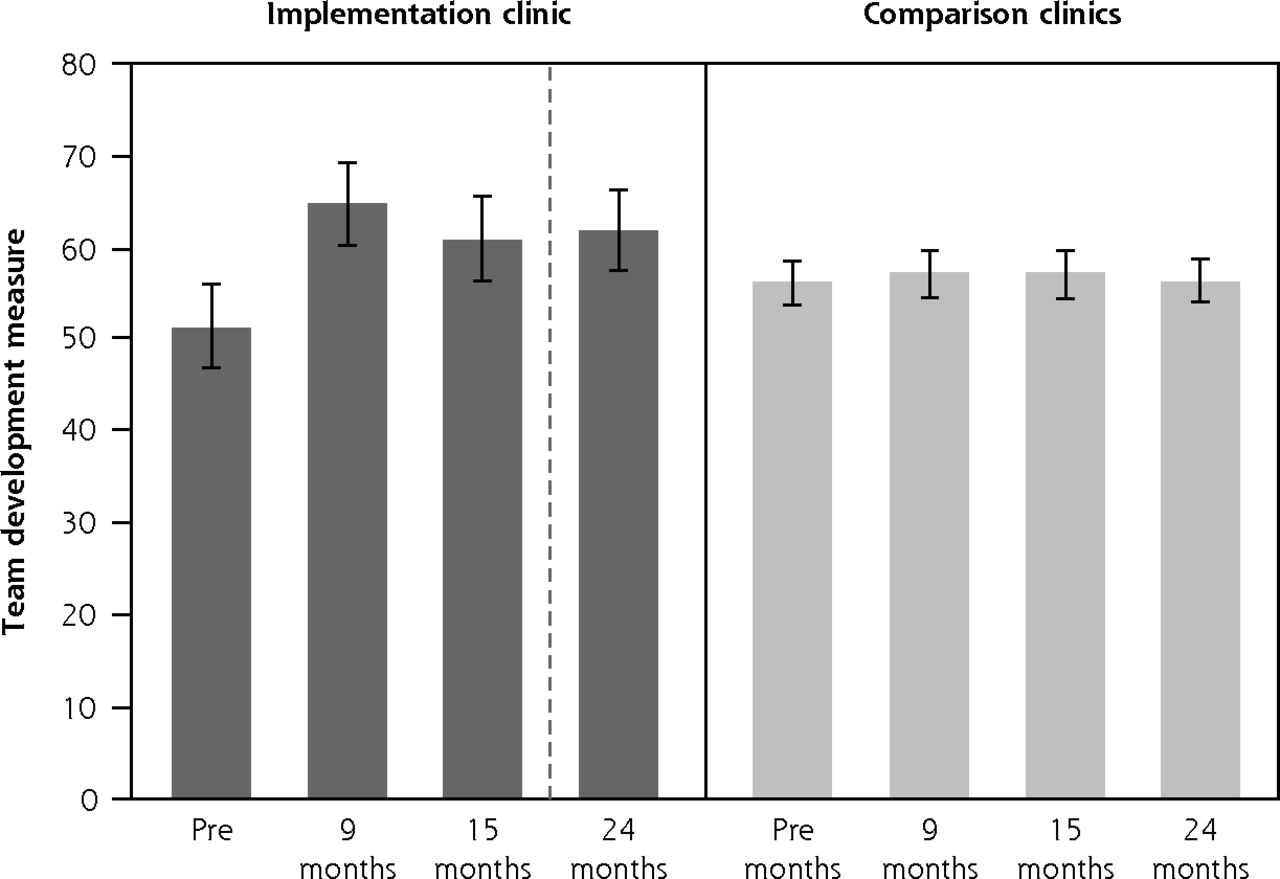
- Figure 1.
Average Team Development Measure scores at each survey time point.
MA = medical assistant; Pre = pre implementation.
Notes: Range bars indicate 95% CIs. The dashed line indicates change in MA to clinician ratio from 2:1 to 1.5:1 at 16 months post implementation.
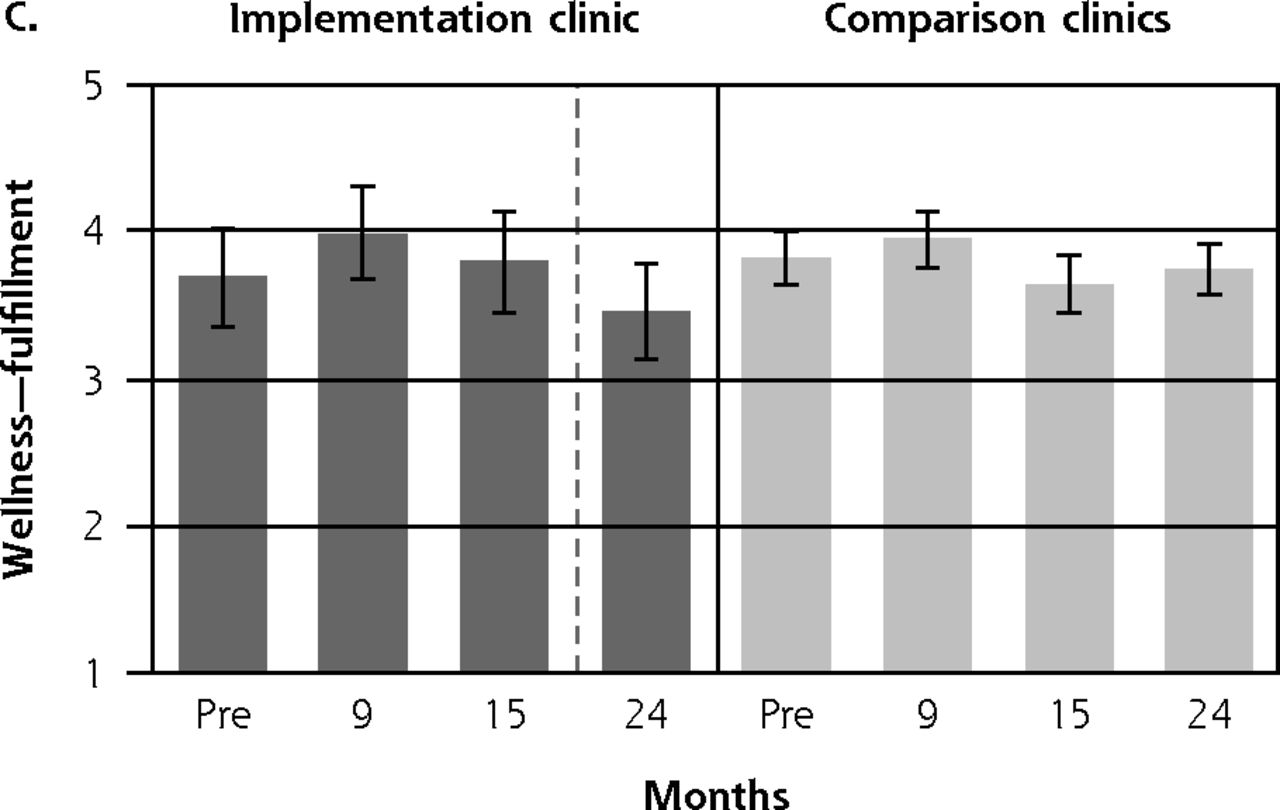
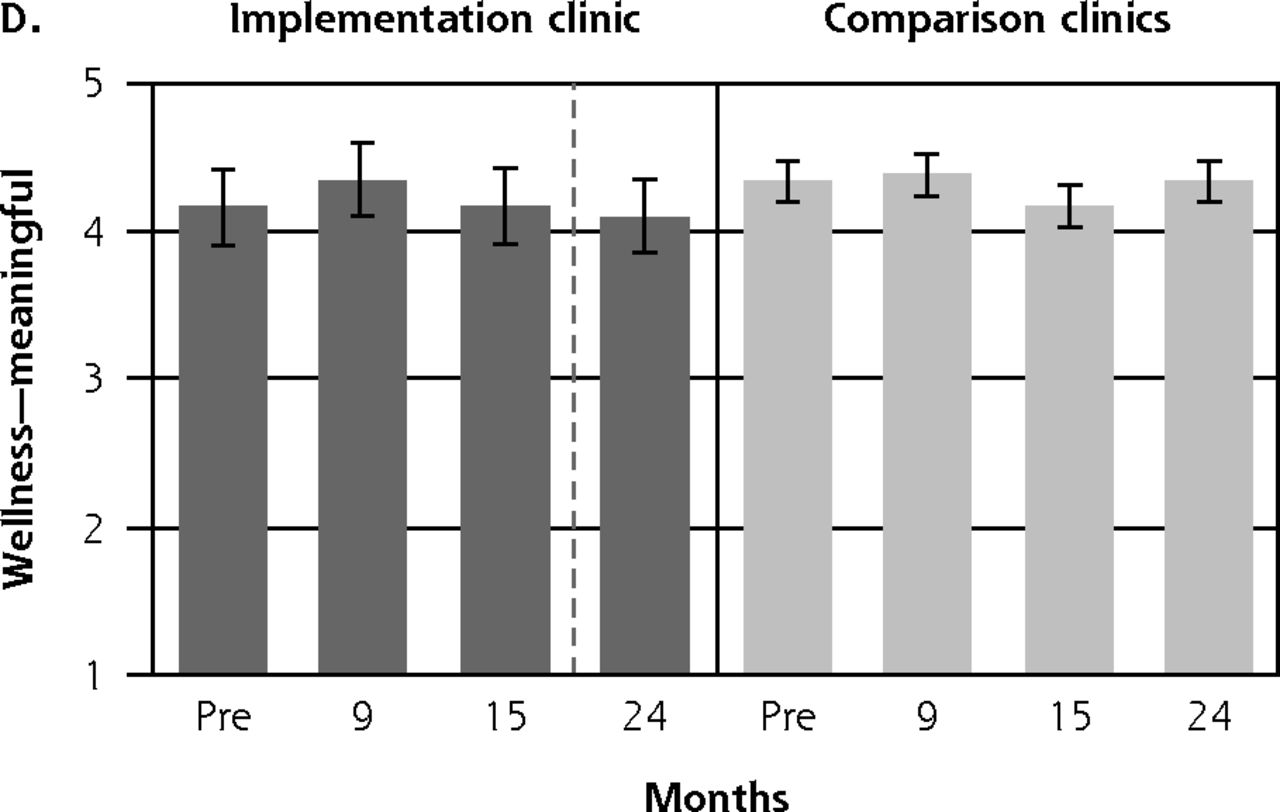
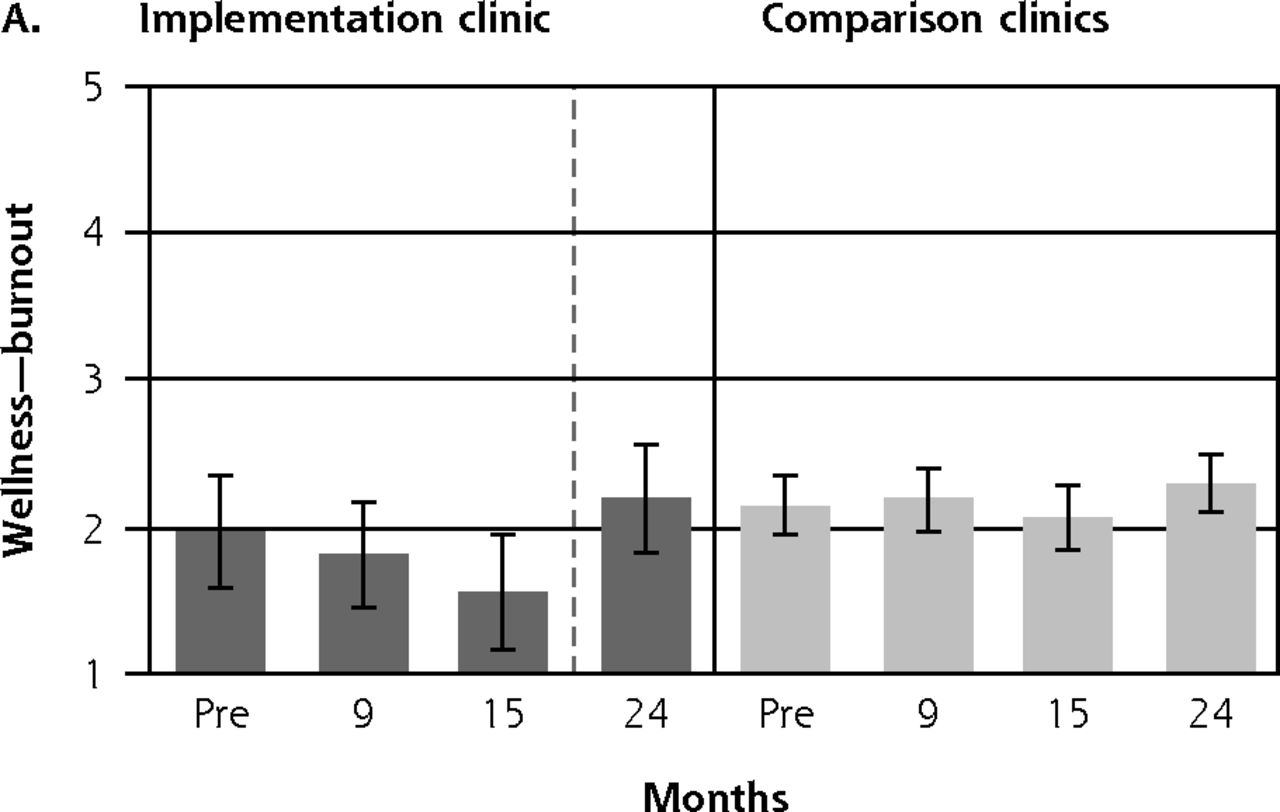
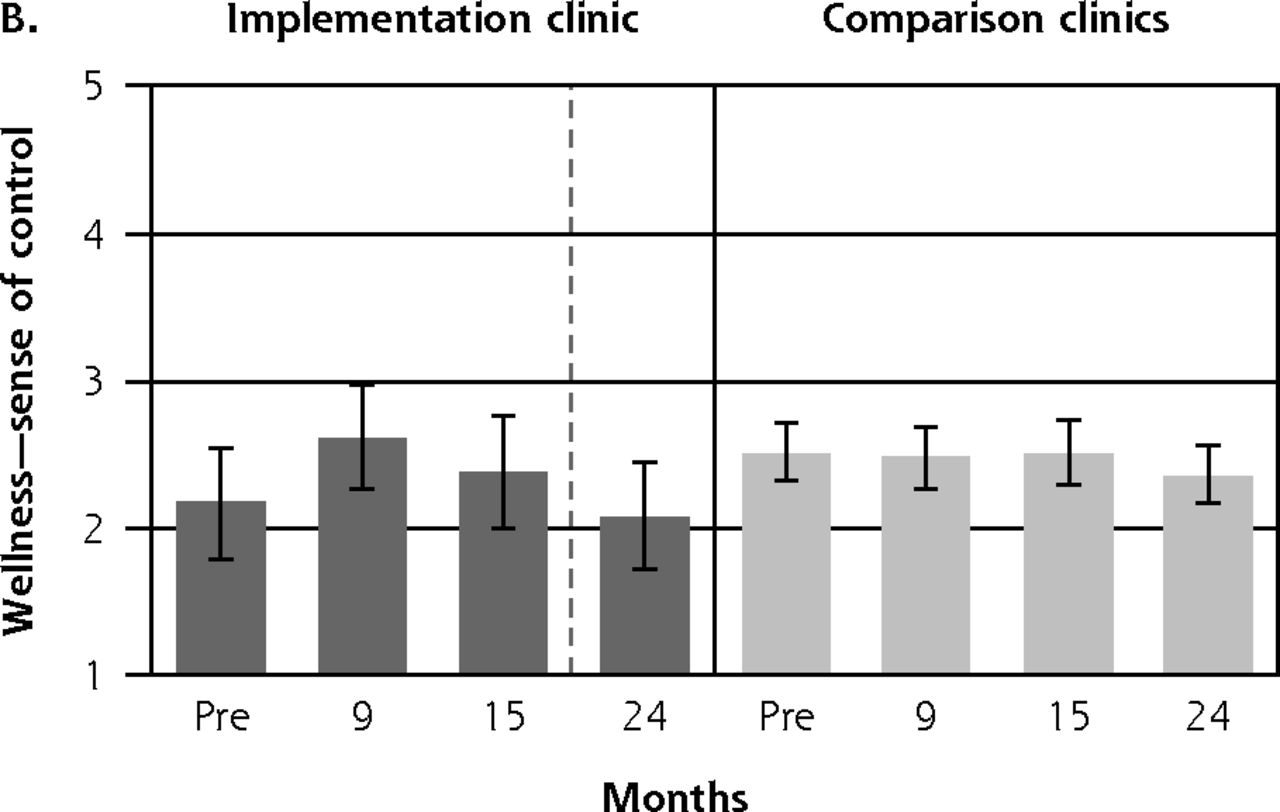
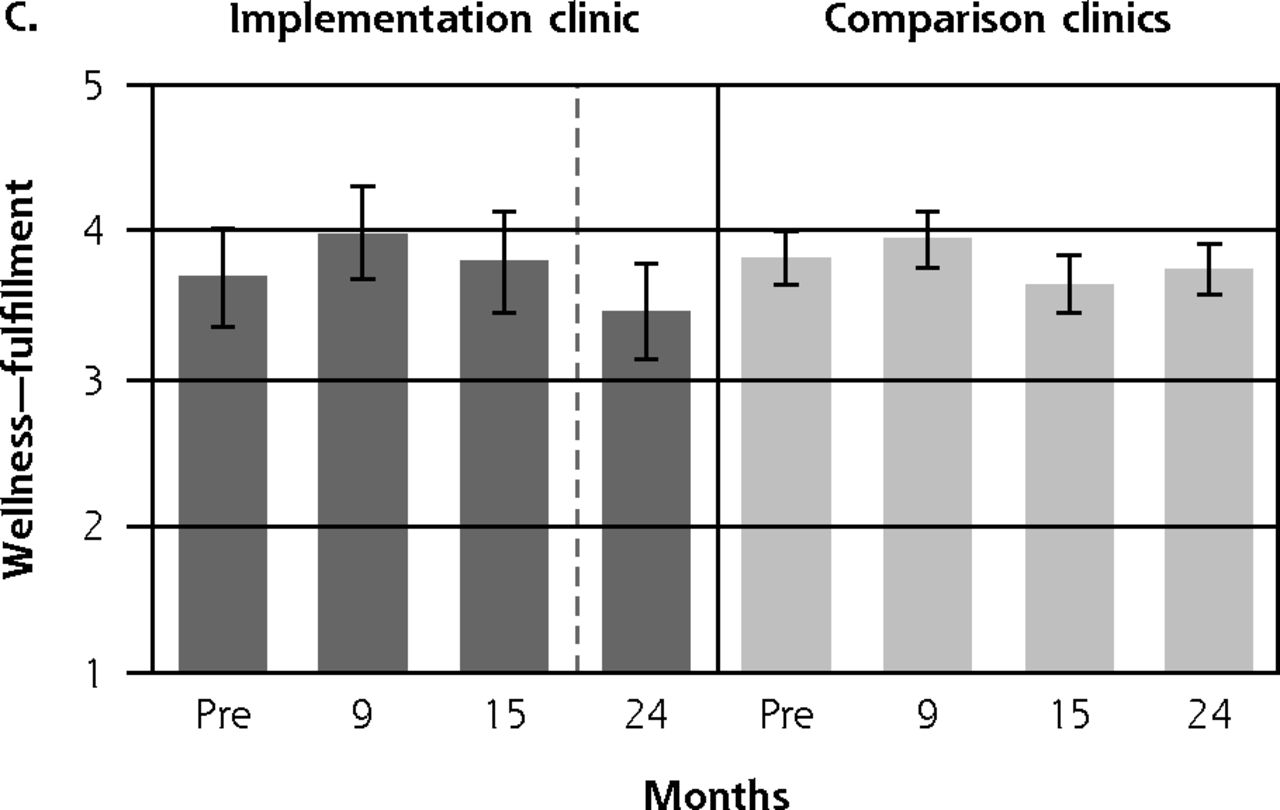
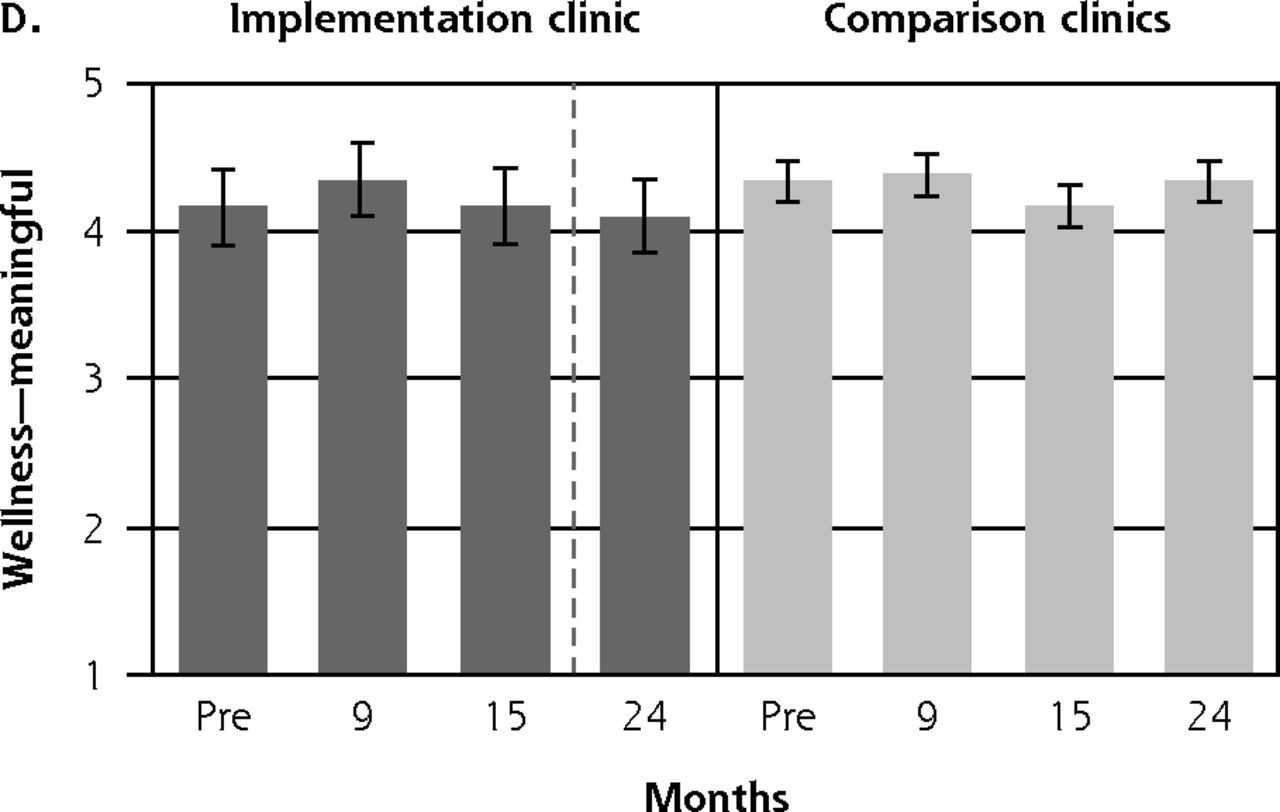
- Figure 2.
Average employee wellness scores, at each survey time point, adjusted for repeated measures.
MA = medical assistant; Pre = pre-implementation.
Notes: Range bars indicate 95% CIs. The dashed line indicates change in MA to clinician ratio from 2:1 to 1.5:1 at 16 months post implementation.


Tables
Settinga PCP Types PCP cFTEsb Annual Visitsb Implementation clinic Primary Care 2.0 site Community-based faculty practice FM, IM 6 (2.0 of which were APC) 13,500 Comparison clinics Site A Hospital-based faculty practice FM 8 17,000 Site B Hospital-based faculty practice IM 8 17,000 Site C Community-based faculty practice FM, IM 5 10,800 Site D Community-based faculty practice FM, IM 3.5 11,700 APC = advanced practice clinician (ie, nurse practitioner or physician assistant); cFTE = clinical full-time equivalent; FM = family medicine; IM = internal medicine; PCP = primary care physician.
↵a All clinics are in a single county and serve primarily private- and Medicare-insured populations.
↵b Values are approximate, based on fiscal year 2018.
Time Point Implementation Clinic (n = 44) Comparison Clinics (n = 144) Wellness, No. (%) Team Development, No. (%) Wellness, No. (%) Team Development, No. (%) Baseline 21 (84) 21 (84) 77 (71) 79 (73) 9 months 24 (63) 22 (58) 66 (49) 66 (49) 15 months 20 (80) 20 (80) 63 (60) 62 (59) 24 months 23 (92) 24 (96) 81 (79) 82 (80) ↵a Response rates (%) are based on number of eligible individuals at each time point, which varies by number of employees at each site, at each time point. The implementation clinic had approximately 25 total staff/clinicians throughout and the 4 comparison clinics ranged from 22 to 40 staff/clinicians at each.
- Table 3.
Difference-in-Difference Analysisa of Team Development and Wellness Scores by Time Point
Survey Time Point (Post Implementation) Team Development DnD, Score (P Value) [95% CI] Wellness Domain DnD, Score (P Value) [95% CI] Burnoutb Sense of Control Fulfillment Meaning 9 months 12.2 (<.001)c –0.2 (.48) 0.5 (.05)c 0.2 (.41) 0.1 (.35) [6.4 to 18.0] [–0.7 to 0.3] [<0.1 to 1.0] [–0.3 to 0.6] [–0.2 to 0.4] 15 months 8.5 (.006)c –0.3 (.26) 0.2 (.41) 0.3 (.23) 0.2 (.29) [2.5 to 14.6] [–0.9 to 0.2] [–0.3 to 0.7] [–0.2 to 0.7] [–0.1 to 0.5] 24 months 10.1 (.001)c 0.1 (.79) 0.1 (.79) –0.2 (.51) –0.1 (.71) [4.1 to 16.1] [–0.5 to 0.6] [–0.5 to 0.6] [–0.6 to 0.3] [–0.4 to 0.3] DnD = difference-in-difference; pre = pre implementation; post = post implementation.
↵a Difference-in-difference calculation = Implementation clinic (post – pre) – Comparison clinics (post – pre); results shown are from linear mixed-models, configured to account for correlation over individuals and time, with the interaction terms of “intervention × time” providing estimate of the difference-in-difference effect of the intervention at each time point (referenced to baseline).
↵b Lower score indicates less burnout.
↵c P value ≤.05
Average of 3 HEDIS Quality Indicatorsa by Clinic, During Intervention October 2016b (Early Implementation), % October 2017c (1 year Post), % October 2018d(2 years Post), % Implementation clinic 93 93 92 Comparison clinics 84 93 90 ACE = angiotensin converting enzyme inhibitors; ARB = angiotensin-receptor blockers; HEDIS = Healthcare Effectiveness Data and Information Set.
↵a Results shown are simple averages (unweighted) of 3 standard HEDIS indicators: 2 diabetes metrics (hemoglobin A1c testing, nephropathy screening rates) and 1 medication monitoring metric of ACE/ARB laboratory monitoring.
↵b Patient denominator for implementation clinic: n = 232 (diabetes metrics) and n = 364 (ACE/ARB metric); Denominator for comparison clinics: n = 1,952 (diabetes metrics) and n = 4,192 (monitoring metric).
↵c Patient denominator for implementation clinic: n = 342 (diabetes metrics) and n = 570 (ACE/ARB metric); Denominator for comparison clinics: n = 1,909 (diabetes metrics) and n = 4,297 (ACE/ARB metric).
↵d Patient denominator for implementation clinic: n = 427 (diabetes metrics) and n = 663 (ACE/ARB metric); Denominator for comparison clinics: n = 2,390 (diabetes metrics) and n = 5,149 (ACE/ARB metric).
Percentage of Patients Giving Highest Score (Top Box) for Likelihood-to-Recommend in the Press Ganey Survey, by Clinic October 2016 (Early Implementation) October 2017 (1 Year Post) October 2018 (2 Year Post) Implementation clinic Top Box Responses, % 82 77 82 Total respondents, No. 56 44 38 Comparison clinics Top Box Responses, % 84 81 85 Total respondents, No. 339 254 232




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}