
Abstract
Substantial shortfalls in the quality of palliative care of the elderly can be attributed to 5 fundamental flaws in the way end-of-life care is currently delivered. First, palliative care is viewed as a terminal event rather than a longitudinal process, resulting in a reactive approach and unnecessary preterminal distress in elderly patients suffering from chronic, slowly progressive illnesses. Second, palliative care is defined in terms of a false dichotomy between symptomatic and disease-focused treatment, which distracts attention from the proper focus of healing illness. Third, the decision about whether the focus of care should be palliative is not negotiated among patients, family members, and providers. Fourth, patient autonomy in making treatment choices is accorded undue prominence relative to more salient patient choices, such as coming to terms with their place in the trajectory of chronic illness. Fifth, palliative care is a parallel system rather than an integrated primary care process. A new theoretical framework—the TLC model—addresses these flaws in the provision of palliative care for elderly persons. In this model, optimal palliative care is envisioned as timely and team oriented, longitudinal, collaborative and comprehensive. The model is informed by the chronic illness care, shared decision making, and comprehensive geriatric assessment research literature, as well as previous palliative care research. Preliminary results of an intervention for elderly assisted living residents based on the TLC model support its promise as a framework for optimizing palliative care of elders.
INTRODUCTION
Despite ambitious palliative care research initiatives,1 process improvement efforts,2 and education programs,3 the quality of palliative care provided to the elderly remains poor. Myriad studies have shown that many older persons nearing the end of life experience unnecessary suffering caused by uncontrolled symptoms,4– 8 depression,9 such existential struggles as making sense of the meaning of one’s life,10, 11 and other issues. These shortfalls exist across a variety of care settings,12 including the community,8, 9 nursing homes,6, 7 and hospitals.4
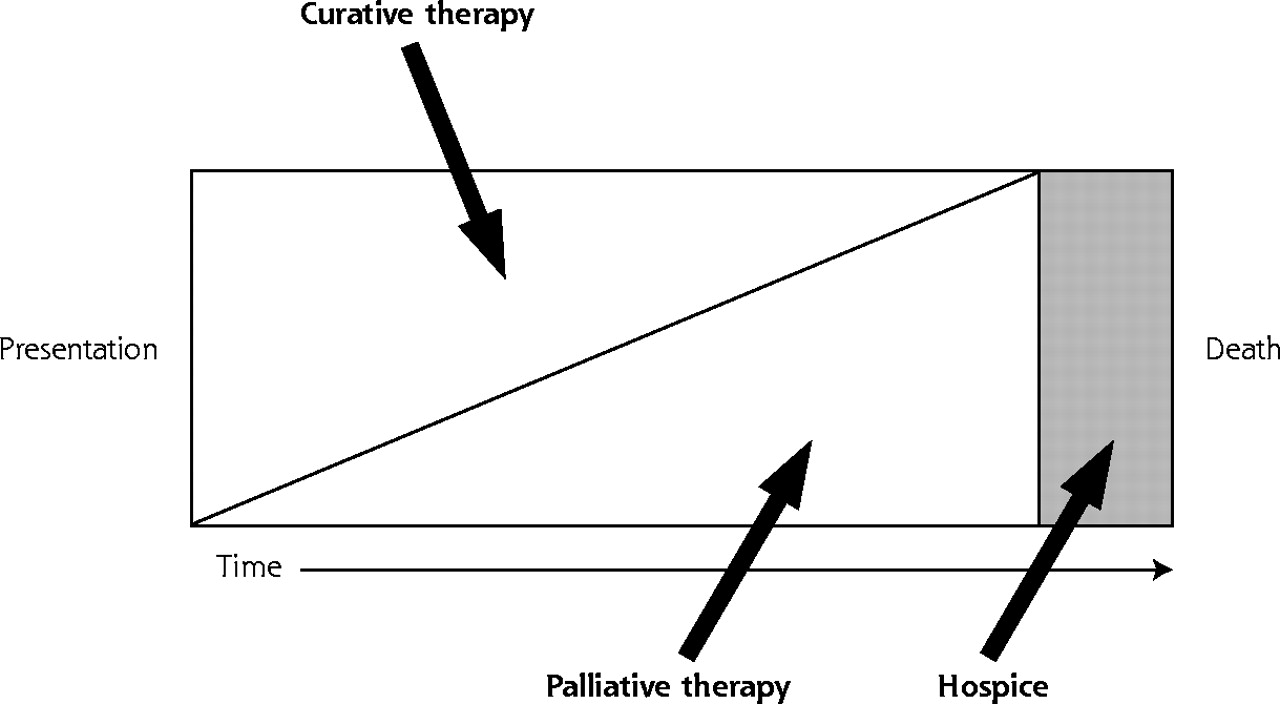
There is a growing recognition3, 13, 14 that previous efforts have largely failed because the underlying conceptual framework for palliative care currently applied to the elderly is fundamentally flawed. We submit that palliative care in older patients should not be viewed as synonymous with hospice or end-of life-care. Rather, palliative care should be viewed as any care primarily intended to relieve the burden of physical and emotional suffering that often accompanies the illnesses associated with aging. Palliative care should thus be a major focus of care throughout the aging process, regardless of whether death is immediately proximate. With this approach, end-of-life care, regardless of whether provided within a hospice framework, represents only part of the continuum of longitudinal palliative care (Figure 1⇓).
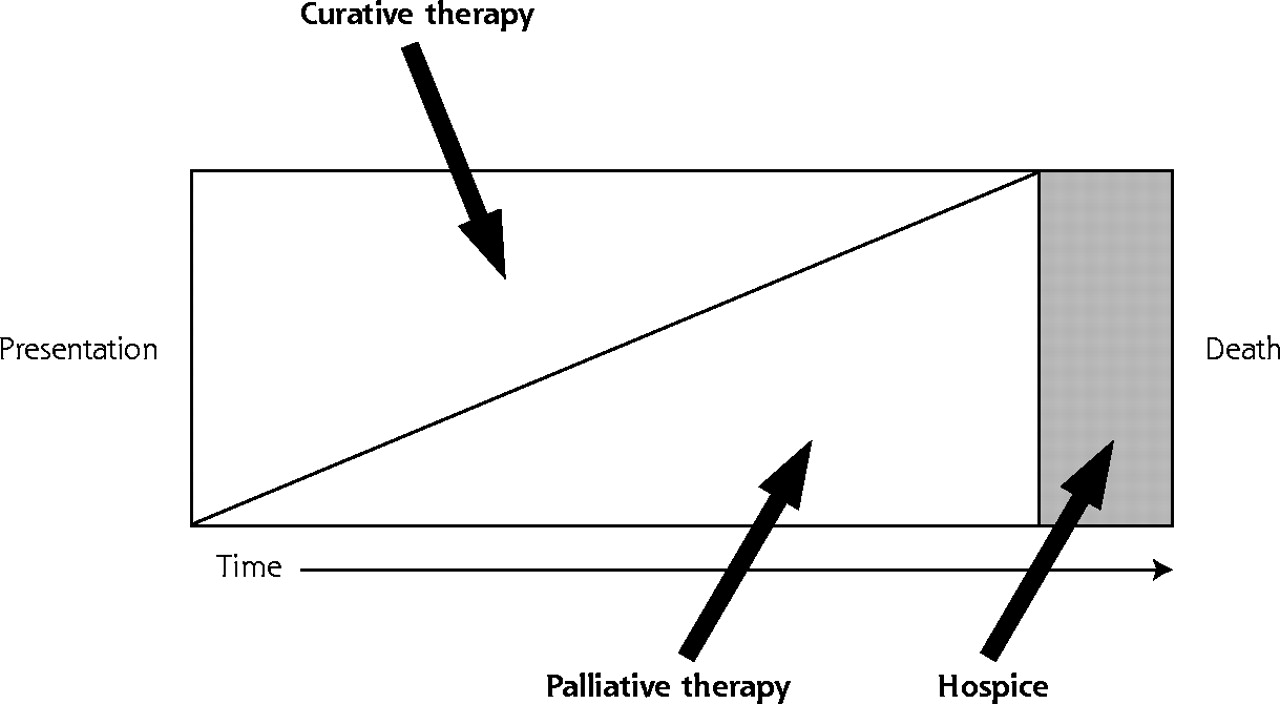
The palliative care continuum.
Adapted with permission from Emanuel LL, von Gunten CF, Ferris FF, eds. “Plenary 3: Elements and Models of End of Life Care,” The Education for Physicians on End-of-Life Care (EPEC) Curriculum:© The EPEC Project, 1999, 2003.
The purposes of this article are (1) to review the problems with the prevailing model of palliative care for older persons, (2) to describe a new model—the TLC model—that provides a useful framework for addressing these problems, and (3) to describe an ongoing palliative care improvement intervention study based on the TLC model and how early results of the study support and inform the model.
FUNDAMENTAL PROBLEMS WITH CURRENT PALLIATIVE CARE FOR THE ELDERLY
Palliative Care as a Terminal Event Rather Than a Longitudinal Process
An unintended consequence of the hospice movement is the tendency to defer palliative care until patients are unequivocally dying. The 6-months-or-less life expectancy requirement for hospice eligibility15 compounds the problem. Whereas the hospice-based palliative care model is often applicable to younger patients dying of cancer, for whom the disease course is relatively predictable, it is ill suited to older persons. Older patients typically die of chronic, slowly progressive illnesses characterized by multiple acute episodes, often followed by full or partial recovery. Current prognostic models fail to accurately predict the timing of death from such illnesses.1, 16, 17 This fundamental mismatch between care paradigm and clinical reality has resulted in an approach to palliative care in the elderly characterized by reacting to acute exacerbation of chronic illness. The result is missed opportunities for palliation at all points along the chronic disease trajectory (Figure 1⇑). Such missed opportunities are evidenced by the palliative care shortfalls mentioned previously,4– 11 as well as the phenomenon of late hospice referrals resulting in very short lengths of stay in many programs.18
Palliative Care Defined Within a False Dichotomy of Symptomatic and Disease-Focused Treatment
Because a disease is “a disorder with a specific cause and recognizable signs and symptoms,”19 the widely promulgated symptom-disease dichotomy is nonsensical. Furthermore, treating underlying disease processes also often ameliorates symptoms. Most importantly, this false dichotomy diverts attention from the proper focus of end-of-life care: the healing of illness, “the patient’s personal experience of a physical or psychological disturbance.”20 Symptoms often have no clear basis in objective disease, and one cannot generally palliate symptoms related to existential suffering (eg, coming to closure with loved ones) with disease-focused treatment.
We submit that only treatment intent helps to distinguish palliative care from other forms of medical care. Most current medical care seeks to prevent death. By contrast, in palliative care, illness is treated to maintain or slow the rate of decline in quality of life.21 The practical importance of the distinction is that treatment intent strongly influences the actual interventions chosen, as well as their extent, dose, and scheduling. For example, chemotherapy regimens for advanced cancer might or might not extend life, but essentially all such regimens cause side effects that can reduce quality of life. By contrast, palliative care might have less chance of extending life but is associated with far less toxicity and may actually lead to improved quality of life.
Decision to Focus Care as Palliative Not Explicitly Negotiated
In clinical practice, neither patients nor family members nor health care providers unilaterally determine treatment intent. Rather, a negotiated agreement among physicians, patients, and family members determines the balance between palliative and curative treatment in the present and future (Figure 1⇑).22– 24 In current care processes, such negotiation is generally tacit rather than explicit. In one study,25 family members of dying patients noted problems communicating with health care clinicians as a critical issue. In a second study,26 families noted that having adequate information and professional caregivers facilitate care transitions enhanced their chances of reaching a turning point at which death was viewed as imminent and helped them make informed decisions.
The current lack of explicit negotiation between patients and physicians regarding optimal balancing of palliative and curative treatment contributes to the neglect of existential patient suffering.10, 22 Such issues as maintenance of dignity are often as important or more important to patients than symptoms such as pain.27 Lack of explicit negotiation also results in failure to support patients in coping with difficult issues early in the dying process, such as deciding where to live, learning to manage decreased finances,28 and struggling “to remain engaged in the everydayness that gives life meaning.”29 Given the often long trajectory of decline in older patients with chronic illnesses, a palliative care approach that includes both managing remaining life and dealing with approaching death seems especially germane.
Autonomous Patient Treatment Decisions Accorded Undue Prominence
The current approach to palliative care is predicated on the false assumption that autonomy forms the basis of human dignity.30 In reality, palliative care choices are heavily dependent upon the presentation of choice by the physician. As noted previously, the difference between the ideal shared decision-making approach and the current one is that physician biases and preferences could be made explicit in the former, whereas in the latter they are generally hidden or implicit. Many treatment choices offered to patients in the name of honoring autonomy are in fact nonchoices.28 For example, dying patients are routinely asked whether they want invasive therapies to keep them alive even when there is no chance of survival, no matter what course is taken. The more salient or controlling choice noted by family caregivers of dying patients in one study was about “the perception of the person’s stage in the illness trajectory” and resulting goals for quality of remaining life—factors that help to determine treatment intent—and not primarily about which specific treatments were to be received.28
Palliative Care as a Parallel System Rather Than an Integrated Process
Palliative care presently occurs outside the usual care processes, often delivered by specialists and other personnel within the hospice framework, with little involvement from primary care physicians. Shoehorning prolonged palliative care discussions into already overloaded periodic office visits is unlikely to remedy this situation. Rather, for palliative care delivery to become an integral part of daily clinical practice, and to facilitate deeper, less hurried, longitudinal palliative care dialogues, creative new ways of maintaining continuous healing relationships31 among patients, families, and primary providers must be sought. Such relationships allow patients to receive care whenever and wherever they need it in a variety of forms, including face-to-face office visits, Internet and electronic mail communication, telephone calls, and other means.
THE TLC MODEL OF PALLIATIVE CARE FOR THE ELDERLY
To begin to remedy these problems, we propose the TLC model of palliative care for older patients (Table 1⇓). In this model, palliative care is defined as care aimed at improving the quality of life of persons nearing (but not necessarily at) the end of life and facilitating the transitions before death.32 This increasingly endorsed definition,3, 12, 33, 34 which contrasts with common usage of the term palliative care as a synonym for terminal care, does not simply arbitrarily extend the period before anticipated death. Rather, it acknowledges the prolonged process of nearing death faced by many older patients who have chronic illnesses and accounts for the wide variation in the point in time at which patients, families, and physicians perceive that death is approaching.
TLC Model of Palliative Care for Elderly Patients
T – Timely and Team Oriented
Palliative care must be timely, not delayed in a misguided attempt to wait for a clearly terminal event, to avoid prolonged, unnecessary suffering. Furthermore, to achieve continuous healing relationships, palliative care must be team-oriented. Given the problem of competing demands during physician office visits,35 health care team members, such as nurses and trained lay persons, must play a major role in supporting family self-care efforts and implementing palliative care.
L – Longitudinal
The ideal trajectory of palliative care for the elderly is longitudinal, with an evolving balance of palliative and curative measures (Figure 1⇑).3 Such an approach could overcome the current tendency to use a reactive approach to end-of-life care that is focused on acute illness exacerbation. Emerging concepts from the literature regarding interventions to optimize longitudinal chronic illness care31, 36 can help to inform such a longitudinal approach.
C – Collaborative and Comprehensive
Palliative care must be a collaborative enterprise among physicians, patients, and their loved ones. Information should flow freely in all directions to facilitate shared decision making. The rich and growing body of literature concerning shared decision-making programs37, 38 to help patients make health care decisions serves as a useful reference point. The content of palliative care efforts must also be comprehensive, informed by empirically supported domains of palliative care.3, 39– 42 Maintaining social roles and relieving existential suffering should be a particularly strong focus of palliative care for older patients to help maintain dignity throughout the dying process.23, 43, 44 The rich and comprehensive geriatric assessment45 research literature can help to inform the content of palliative care for older patients, even though the target population for the TLC approach is located close to (but not necessarily at) the hospice bar in Figure 1⇑, whereas the target population for traditional comprehensive geriatric assessment is closer to the extreme left.
PRELIMINARY EVALUATION OF THE TLC MODEL
There is currently no empirical research to support the effectiveness of palliative care interventions based on the TLC model. Given its high face validity and grounding in descriptive research, however, we are conducting an evaluation of an intervention based on the TLC model. We describe the intervention and preliminary study findings in the following sections.
Assisted Living: An Ideal Setting for TLC Model Application
Assisted living facilities are congregate residential settings that provide or coordinate personal services, supervision, activities, and health-related services.46 There are about 1.5 million assisted living beds in the United States, and demand is expected to grow considerably during the next 20 years as the population ages.47 Three issues make the assisted living facility an ideal setting in which to evaluate the TLC model of palliative care for the elderly.
First, the elderly resident population is increasingly functionally impaired and frail.48, 49 The typical resident is an 80-year-old woman who needs assistance with two activities of daily living.46 The estimated life expectancy for persons of this age and degree of frailty is generally less than 2 years.50 Thus, most elderly residents in assisted living facilities are nearing but not necessarily at the end of life. Second, because most residents suffer from multiple chronic illnesses for which an accurate prognosis is impossible,18, 51 the current approach of delaying palliative care until death is clearly imminent is likely resulting in unnecessary, prolonged resident suffering. Third, recent reviews have disclosed no reports concerning palliative care needs or quality in this population.52, 53
The Palliative Care in Assisted Living (PCAL) Study
To begin to fill this important knowledge gap and compare the effectiveness of 2 interventions for improving palliative care in older persons based on the TLC model, we are conducting the Palliative Care in Assisted Living (PCAL) study. From November 2000 through June 2004, English-speaking residents of 2 assisted living facilities in the Sacramento, Calif, area, operated by a single not-for-profit corporation, are being invited to volunteer for the PCAL study. Facility 1 houses 100 residents and facility 2 houses 35 residents. Care processes at the facilities are essentially identical. The average resident age is 85 years, two thirds are female, and nearly all are white and English speaking. Most residents pay facility fees out of pocket. Residents who cannot understand the consent form because of cognitive impairment or who are unable to consent because of serious acute illness are excluded.
Methods
The study is a nonblinded, prospective comparison trial. Intervention assignment is by facility to avoid cross-contamination among subjects. The study assessment (Table 2⇓) combines a series of validated instruments to address content domains drawn from the palliative care3, 39– 42 and geriatric assessment45 literature. The assessment is conducted by one of the authors (AFJ) at the facilities in 2 parts spaced 2 to 3 weeks apart, each lasting 1 to 1.5 hours. Nearly all the residents have at least 1 family member or friend who assists with making medical decisions, and whenever possible, we arrange for these persons to accompany the resident.
Palliative Care in Assisted Living (PCAL) Study Assessment Elements and Measures
Within 24 hours of completing the assessment, a letter containing palliative care recommendations based on the findings (the study intervention), as well as resident and family input and preferences, is mailed to the resident, primary provider, and appropriate family member(s). Facility 1 (more intensive intervention) residents receive identical assessments with new recommendation letters every 3 months. For facility 2 (less intensive intervention) residents, outcomes are assessed at appointments every 3 months, but no further recommendations are provided. Residents receive their assigned intervention until they leave their facility, die, or drop out.
Data regarding the impact of the ongoing study interventions on patient outcomes, such as health-related quality of life, are not yet available. We present, however, a brief summary of preliminary findings concerning the palliative care needs of enrollees. SPSS 10.0.5 for Windows (SPSS, Inc, Chicago, Ill) was used for all analyses.
Preliminary Study Findings
Sixty-one patients had enrolled by June 30, 2002: 44 at facility 1 (27% of the facility population since enrollment began) and 17 at facility 2 (28% of the facility population). Data presented are for the 50 residents (facility 1, n = 37, facility 2, n = 13) who had received a baseline assessment before the interim analysis. Residents were very old (mean age 85.4 years, ± 7.2 SD), 36 (72%) were female, 48 (96%) were white (96%) and highly educated, with a mean of 15.2 (± 2.7 SD) years of formal education. Lack of energy (27, 54%), feeling drowsy (27, 54%), pain (26, 51%), feeling sad (25, 50%), difficulty concentrating (25, 50%), worrying (22, 44%), and feeling nervous (16, 32%) were the most prevalent symptoms in the week before assessment. Twelve of 50 residents (24%) scored at or above the possibly depressed cut point on the Geriatric Depression Scale.
Thirty-four of 50 residents (68%) possessed adequate cognition to complete the values history; 1 refused to complete the medical interventions subsection. Responses to 2 basic life values questions (5-point Likert scale, 5 = extremely important, 1 = not at all important) indicated a strong tendency to value maintaining the quality of remaining life (3.9, ± 0.8 SD) rather than prolonging life at less than current quality (1.9, ± 0.9 SD, P <.001 for difference in response distributions, Wilcoxon test). Most residents (20 of 33, 61%) wished to avoid cardiopulmonary resuscitation. Only a small percentage of residents expressed an unqualified wish to receive mechanical ventilation (3%), total parenteral nutrition (12%), or an enteral feeding tube (21%). A greater percentage (58%, 51%, and 42%, respectively), however, expressed willingness to receive these treatments for a brief (10 days or less) trial period. Thirty-six of 50 residents (72%) had a durable power of attorney for health care, but only 4 residents (8%) had a do-not-resuscitate order. No resident met National Hospice Organization hospice eligibility criteria.
A mean of 5.3 (± 2.0 SD) palliative care improvement recommendations per resident were generated from the baseline assessment at facility 1 and 4.8 (± 2.2 SD) at facility 2. Table 3⇓ summarizes the frequency of the various subcategories of recommendations.
Palliative Care Improvement Recommendations for Elderly Residents of 2 Assisted Living Facilities (N = 50)
DISCUSSION
Preliminary Support for the TLC Model
Our preliminary findings and those of others4, 6, 52 illustrate glaring deficits in the quality of palliative care for older persons. No subject in our study was terminally ill, and none was a candidate for hospice, yet all were approaching the end of life and had multiple unmet palliative care needs. These findings show a pressing need for a major paradigm shift in the way palliative care of elders is conceptualized and delivered.13 They also provide initial support for the TLC model as a promising framework for better meeting the palliative care needs of older patients. Until intervention evaluations like the PCAL study are completed, however, the impact of using the TLC framework on patient outcomes remains unclear. If the study results are favorable, future researchers might build upon the interventions we have outlined by including even greater emphasis on such important issues as bolstering patients’ sense of dignity43, 44 and self-efficacy67, 68 and supporting family caregivers throughout the trajectory of chronic illness.26
CONCLUSION
It is clear that the prevailing model of palliative care is ill suited for application to older patients suffering from slowly progressive chronic illnesses. The TLC model provides a promising potential framework for designing interventions to address current palliative care shortfalls and improve both the quality of remaining life and process of dying for older persons and their loved ones. Given the high amount of conceptual overlap with already familiar tasks, such as chronic illness care coordination, primary care physicians appear well suited to assume the role of team leader for palliative care delivered within the TLC framework.
Footnotes
Conflict of interest: none reported
Funding support: Funded in part by a Robert Wood Johnson Foundation Generalist Physician Faculty Scholar Program (RWJF GPFSP) career development grant, No. 039176 (Dr. Jerant) and a RWJF Promoting Excellence in End of Life Care Program grant, No. 035490 (Dr. Meyers).
Versions of this paper were presented in part at the RWJF GPFSP Annual Meeting, Ponte Vedra, Calif, December 4–6, 2002?
- Received for publication September 16, 2002.
- Revision received January 17, 2003.
- Accepted for publication February 10, 2003.
- © 2004 Annals of Family Medicine, Inc.




{kind=link}