
Article Figures & Data
Figures
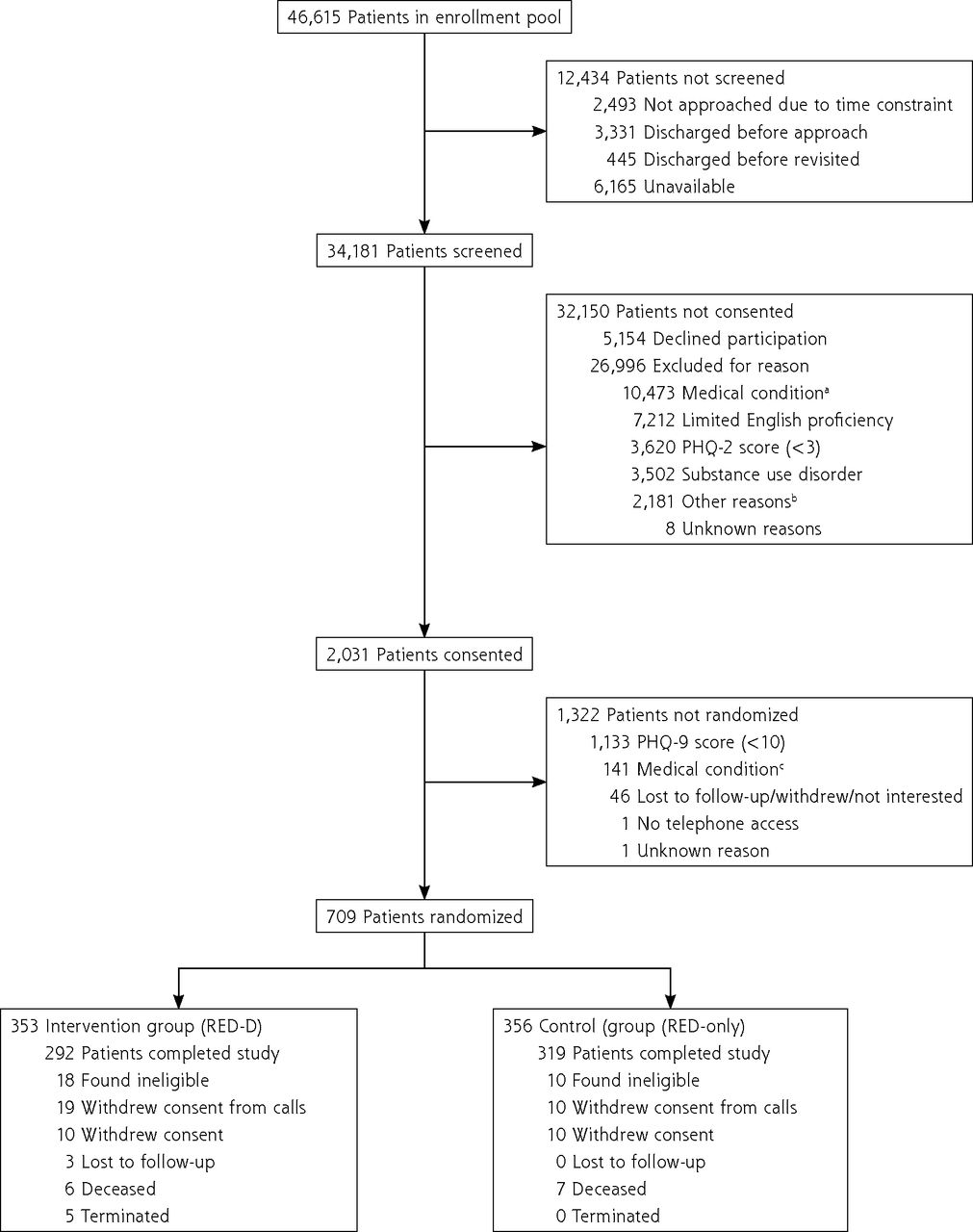
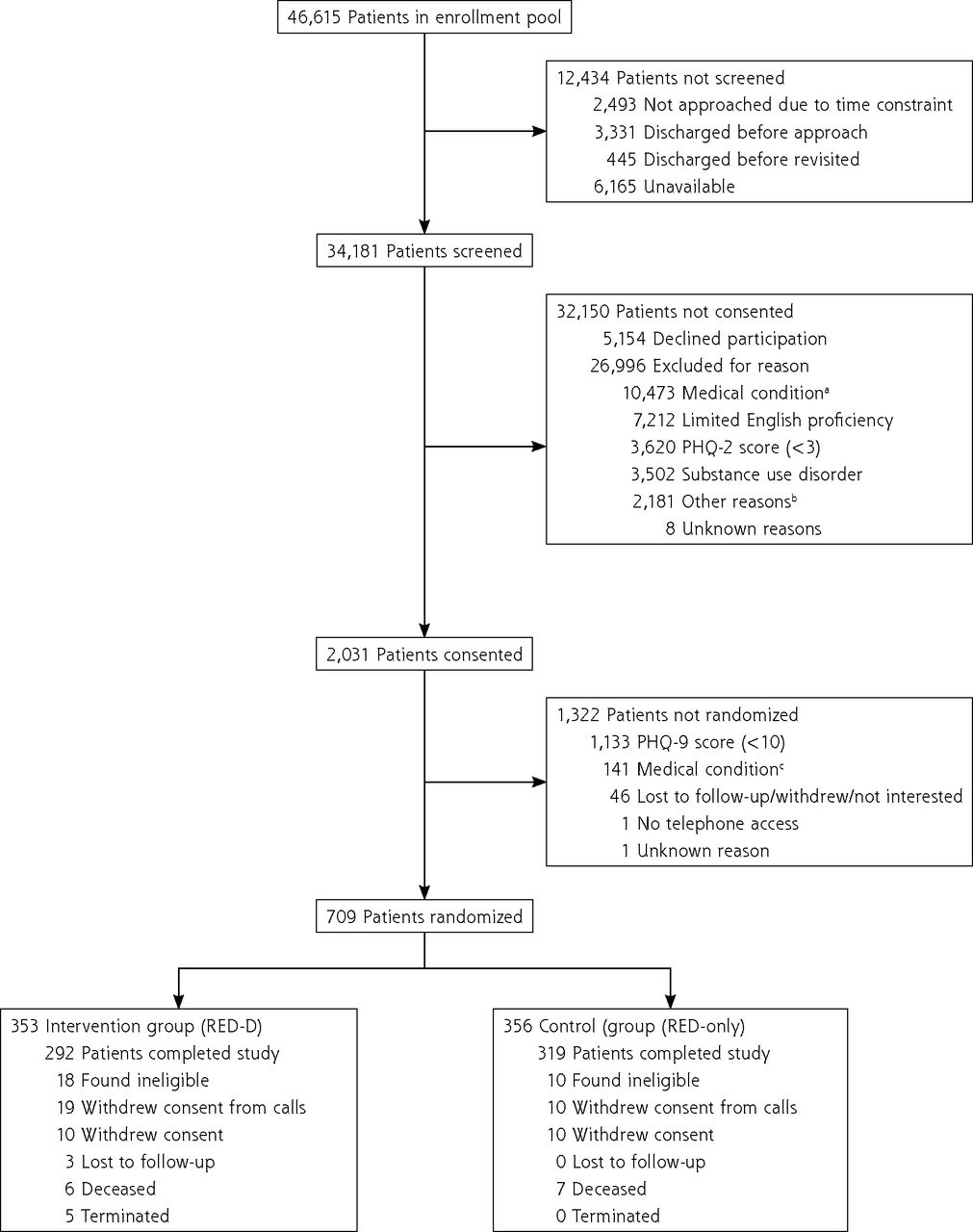
- Figure 1.
Study flowchart.
CAGE = 4-item screening for alcohol use: cutting down, annoyance by criticism, guilty feeling, and eye-openers; DAST = 10-item drug abuse screening test; PHQ-9 = patient health questionnaire-9; PHQ-2 = patient health questionnaire-2; RED = re-engineered discharge; RED-D = re-engineered discharge for depression.
a Medical exclusion occurred in phases. Patients admitted for altered mental status, end-of-life care, sickle cell crisis, or substance use were excluded from the pool immediately. Then, potentially eligible patients were excluded if they were going to be discharged to another inpatient facility, pregnant, under suicide precautions, undergoing cancer treatment; admitted to a surgical trauma unit.
b Other reasons for exclusion included: incarceration; no access to telephone; no primary care clinician; not staying in the area during the study; aged <18 years; enrolled in another discharge planning program.
c Medical exclusions after consent were for having a serious mental illness diagnosis, self-reported suicidal ideation, and self-reported alcohol or drug abuse (CAGE score >2, DAST score >5).
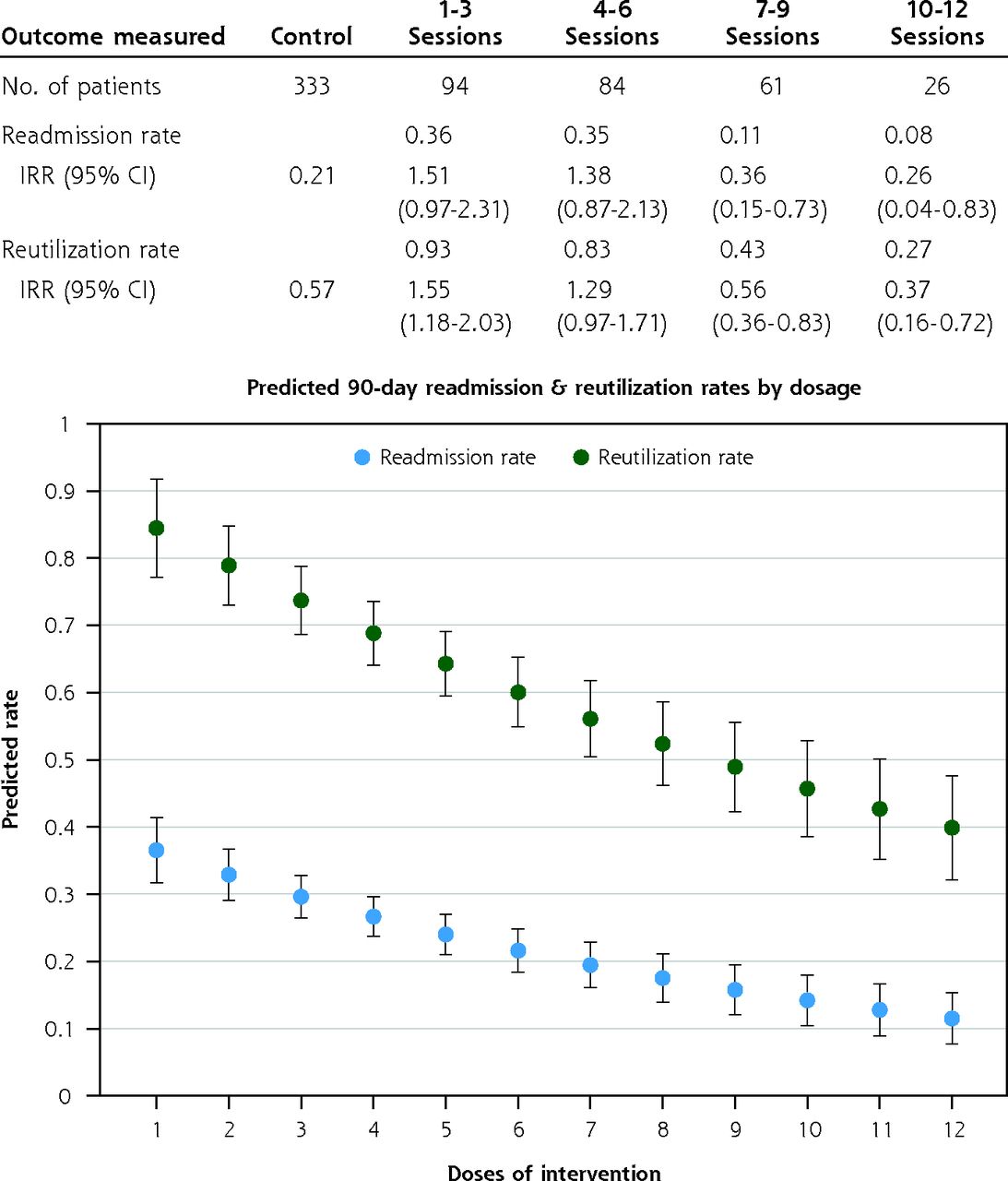
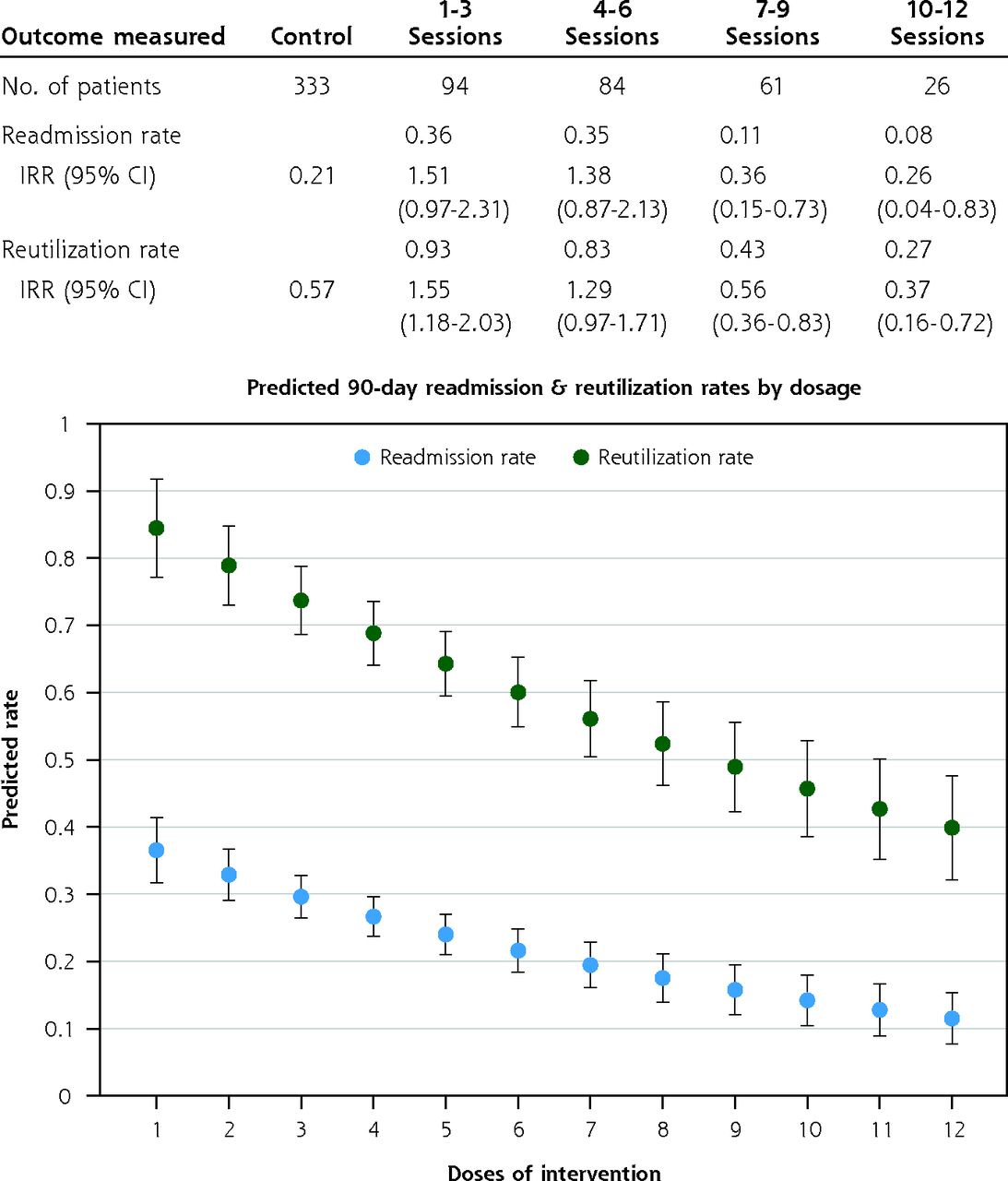
- Figure 2.
Readmission and reutilization rates for intervention patients by the number of counselling sessions completed at 90 days.
IRR = incidence rate ratio.
Note: Labeled points indicate predicted values from Poisson regression of 90-day readmission and reutilization rates on cumulative dosage of the intervention. Each value represents the readmission or reutilization rate we would expect at that associated dosage, based on regression models.
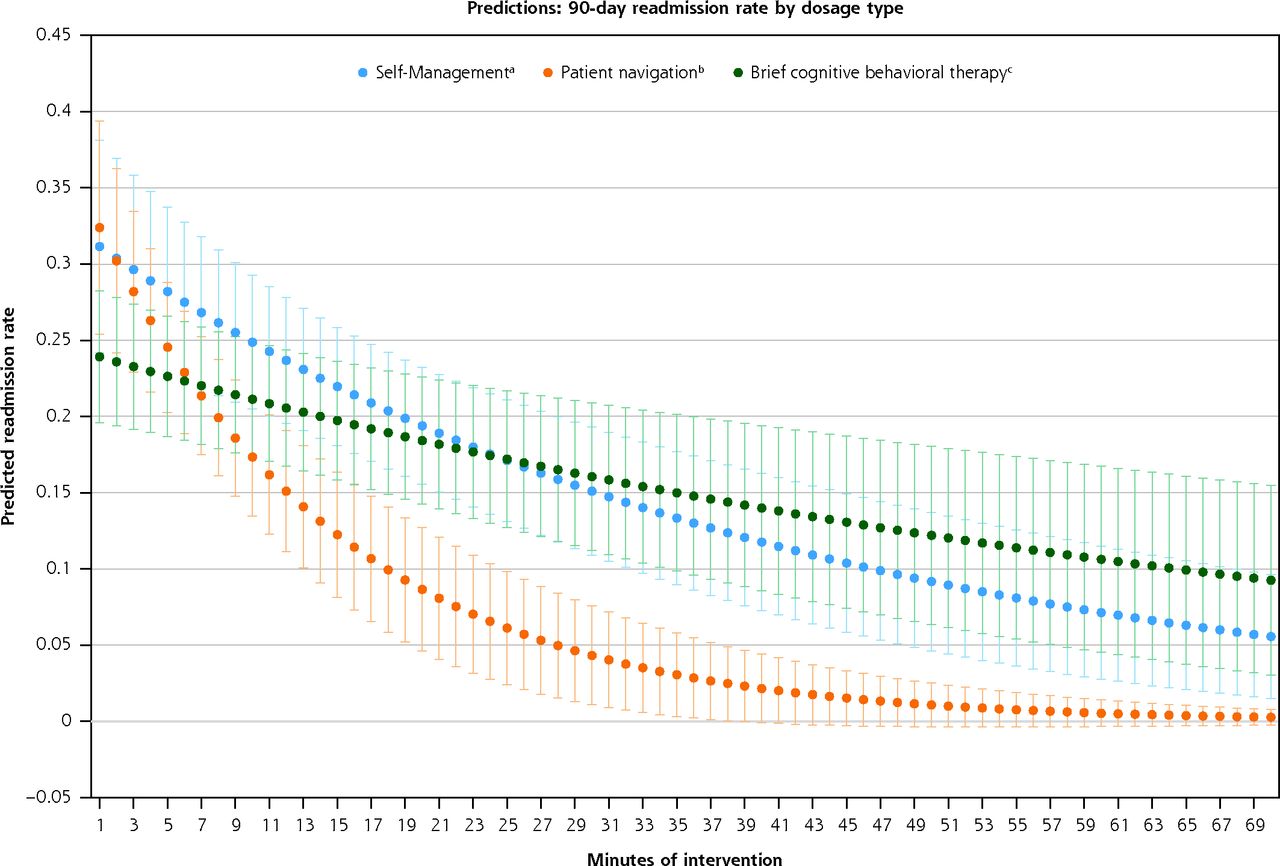
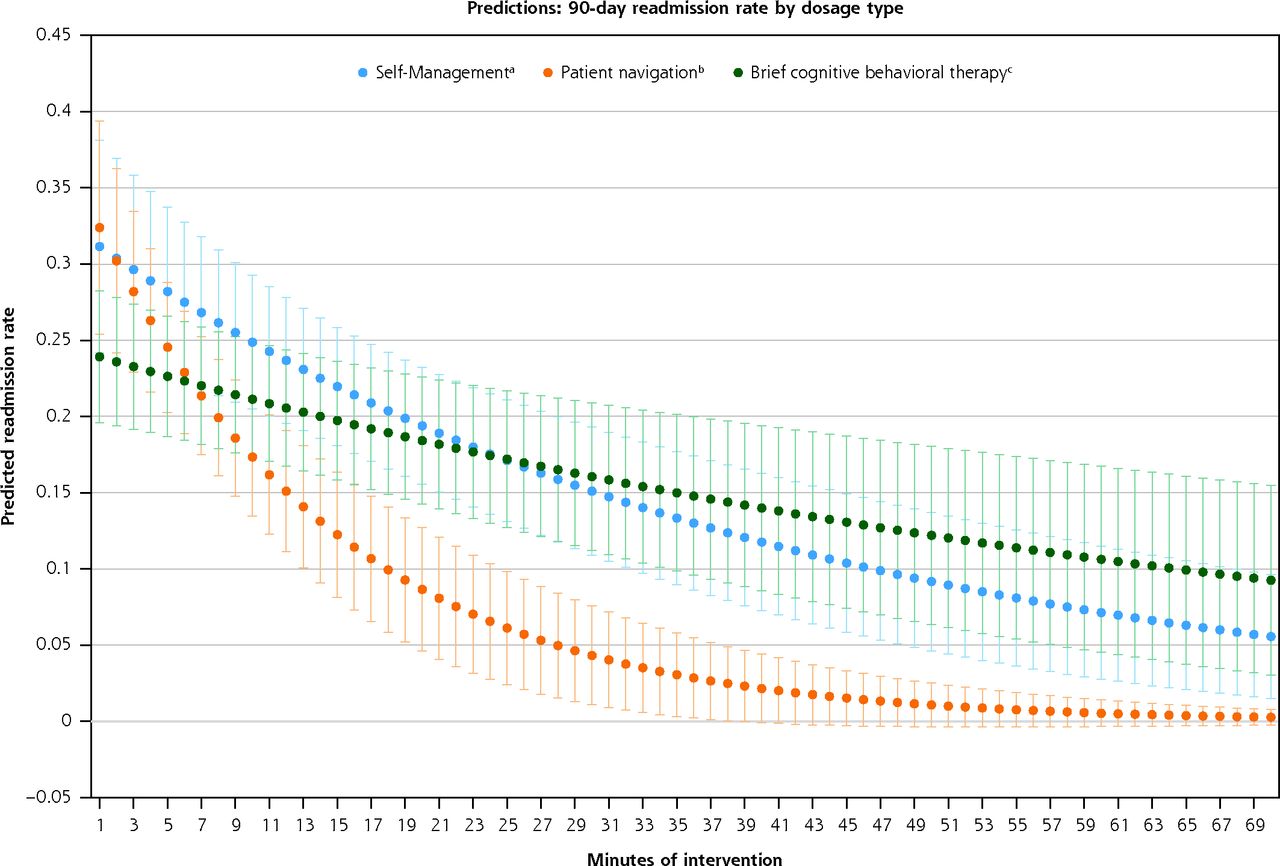
- Figure 3.
Predicted readmission rate at 90 days by type of post-discharge support for intervention participants receiving 6 or more sessions.
Note: Predicted values were generated using Poisson regression.
a Self-management was counselling focused on chronic disease self-management, including diet/nutrition, exercise, managing medications, talking to your doctor, and coping with exacerbations.
b Patient navigation includes guidance in navigating difficult aspects of the health care system, such as overcoming financial barriers, scheduling appointments, and coordinating transportation services, as well as adherence to the discharge plan and follow-up care.
c Brief cognitive behavior therapy includes orientation to the thought-feeling connection, transforming negative thoughts, behavior activation, physical symptoms, and stress management and navigating relationships, and homework.25
Tables
Characteristic Control
(n = 356)Intervention
(n = 353)Women, No. (%) 221 (62.1) 210 (59.5) Age, mean (SD) 51 (13.7) 50 (13.4) Race, No. (%) White non-Hispanic 129 (36.2) 112 (31.7) Black non-Hispanic 147 (41.3) 160 (45.3) Hispanic 59 (16.6) 67 (19.0) Other race 52 (14.6) 42 (11.9) Annual personal income, $, No. (%) <10,000 48 (13.5) 40 (11.3) 10,000-19,999 65 (18.3) 66 (18.7) 20,000-49,999 49 (13.8) 58 (16.4) ≥50,000 43 (12.1) 34 (9.6) No personal income 25 (7.0) 24 (6.8) Refused 51 (14.3) 53 (15.0) Did not know 74 (20.8) 77 (21.8) Education level, No. (%) Less than high school 14 (3.9) 16 (4.5) Some high school 47 (13.2) 40 (11.3) High school graduate or GED 134 (37.6) 124 (35.1) Some college 104 (29.2) 111 (31.4) 4-year college graduate or higher 57 (16.0) 61 (17.3) Health literacy level, grade level, No. (%)b ≤3 0 (0.0) 3 (0.8) 4-6 9 (2.5) 11 (3.1) 7-8 49 (13.8) 53 (15.0) ≥9 232 (65.2) 196 (55.5) Did not report 66 (18.5) 90 (25.6) Current employment status, No. (%) Full-time 60 (16.9) 76 (21.5) Part-time 36 (10.1) 29 (8.2) Homemaker 3 (0.8) 7 (2.0) Student 4 (1.1) 3 (0.8) Retired 63 (17.7) 51 (14.4) Disabled 120 (33.7) 119 (33.7) Unemployed 56 (15.7) 62 (17.6) Otherc 14 (3.9) 5 (1.4) Recruitment site, No. (%) Boston Medical Center 328 (92.1) 325 (92.1) Mt Auburn Hospital 28 (7.9) 28 (7.9) Homeless in past 6 months, No. (%) 28 (7.9) 24 (6.8) Major depressive disorder, No. (%)c 110 (30.9) 96 (27.2) Mean PHQ-9, (SD)d 15 (4.2) 15 (4.2) Q-LES-Q-SF, mean (SD)e 45 (15.9) 45 (16.0) GAD-7, mean (SD)f 11 (5.5) 10 (5.8) PAM-13, mean (SD)g 42 (5.6) 42 (5.5) Medication for depression, No. (%)h 140 (39.3) 123 (34.8) GAD = generalized anxiety disorder; GED = general equivalency diploma; PAM = patient activation measure; PHQ-9 = patient health questionnaire-9; Q-LES-Q-SF = quality of life enjoyment and satisfaction questionnaire – short form.
↵a Not all column percentages sum to 100% due to missing values.
↵b REALM (Rapid Estimate of Adult Literacy in Medicine). Health literacy categories correspond to scores of grade 3 or below (REALM score, 0-18), grade 4 to 6 (REALM score, 19-44), grade 7 to 8 (REALM score, 45-60), and grade 9 or above (REALM score, 61-66).20
↵c Determined by clinical interview by licensed mental health counselor after enrollment.
↵d Patient Health Questionnaire-9 is a 9-item scale. A score of ≥10 indicates moderate depressive symptoms.16
↵e Quality of Life Enjoyment and Satisfaction Questionnaire Short Form is a 16-item scale indicating the degree of enjoyment and satisfaction experienced by participants in various areas of daily functioning. The reported score is the sum of the question responses rescaled to 100. Higher scores indicate higher enjoyment and satisfaction.21
↵f Generalized Anxiety Disorder 7 is a 7-item scale. A score of 10-14 indicates possible clinically significant generalized anxiety and ≥15 indicates that treatment is probably warranted.23
↵g Patient Activation Measure 13 is a 13-item scale indicating the degree of patients’ willingness and ability to take independent actions to manage their health and care. Raw scores converted to range from 0-100 with ≤47.0 not believing activation important; 47.1-55.1 indicating a lack of knowledge and confidence to take action; 55.2-67.0 beginning to take action; and ≥67.1 taking action.22
↵h Self-reported answer to the question “Are you currently taking medication for depression?”
Intention-to-Treat Analysis
As-Treated AnalysisAs-Treated Analysis 30-Day Outcomes Type of Primary Outcome Controla
(n = 356), No. (%)Interventionb
(n = 353), No. (%)P Value, IRR (95% CI) ≥3 Sessionsc
(n = 104), No. (%)P Value, IRR (95% CI) Hospital utilizationsd 82 (0.24) 89 (0.27) .386, 1.14 (0.85-1.54) 20 (0.17) .377, 0.80 (0.48-1.28) ED visits 32 (0.09) 32 (0.10) .839, 1.05 (0.64-1.72) 9 (0.09) .653, 0.93 (0.42-1.86) Readmissionse 33 (0.10) 29 (0.09) .758, 0.92 (0.56-1.52) 3 (0.03) .012, 0.30 (0.07-0.84)f Observations 17 (0.05) 28 (0.09) .215, 1.73 (0.96-3.23) 8 (0.08) 0.343, 1.55 (0.63-3.49) 90-Day Outcomes Controla (n = 356), No. (%) Interventionb
(n = 353), No. (%)P Value, IRR (95% CI) ≥6 Sessionsg
(n = 109), No. (%)P Value, IRR (95% CI) Hospital utilizationsd 189 (0.57) 219 (0.70) .041, 1.22 (1.01-1.49) 48 (0.44) .162, 0.78 (0.56-1.06) ED visits 82 (0.25) 86 (0.27) 0.504, 1.11 (0.82-1.50) 23 (0.21) .544, 0.86 (0.53-1.34) Readmissionse 71 (0.21) 87 (0.28) .106, 1.30 (0.95-1.78) 12 (0.11) .030, 0.52 (0.27-0.92)f Observations 36 (0.11) 46 (0.15) .177, 1.35 (0.88-2.10) 13 (0.12) .797, 1.1 (0.56-2.03) ED = emergency department; IRR = incidence rate ratios; RED = re-engineered discharge; RED-D = re-engineered discharge for depression.
↵a Control group received the components of the re-engineered discharge (RED).10
↵b Intervention group received the components of the re-engineered discharge, and were offered up to 12 weekly counselling sessions that included brief cognitive behavioral therapy, patient navigation, and self-management (RED-D).
↵c ≥3 sessions includes those patients in the intervention group receiving 3 sessions of the intervention by 30 days.
↵d Hospital reutilizations are defined as the sum of hospital readmission plus emergency department visits and observations after index discharge.
↵e Readmissions are defined as 30 and 90 day all cause hospital readmissions after index discharge.
↵f Results are statistically significant.
↵g ≥6 sessions includes those patients in the intervention group receiving 6 sessions of the intervention by 90 days.
SUPPLEMENTAL TABLES & FIGURES IN PDF FILE BELOW
- MitchellSuppApps.pdf -
PDF file
- MitchellSuppApps.pdf -




{kind=link}
{kind=link}
{kind=link}