
Article Figures & Data
Figures
- Figure 1.
Numbers of facilitators and practices.
ABS = aspirin use for high-risk patients; CPCQ = Change Process Capability Questionnaire.
Notes: Numbers of practices that improved on the CPCQ score and on the aspirin, blood pressure, and smoking measures are not mutually exclusive and add up to more than the total number of practices with high change capacity or low change capacity.
a More effective: ≥75% of facilitator’s practices had improved CPCQ scores and/or ABS performance; less effective: <50% of facilitator’s practices had improved CPCQ scores and/or ABS performance. A total of 53 facilitators with 740 practices were neither more nor less effective, and were excluded from effectiveness analyses.
b Assessed from baseline CPCQ score, dichotomized at the median value as high (score ≥11) or low (score <11).
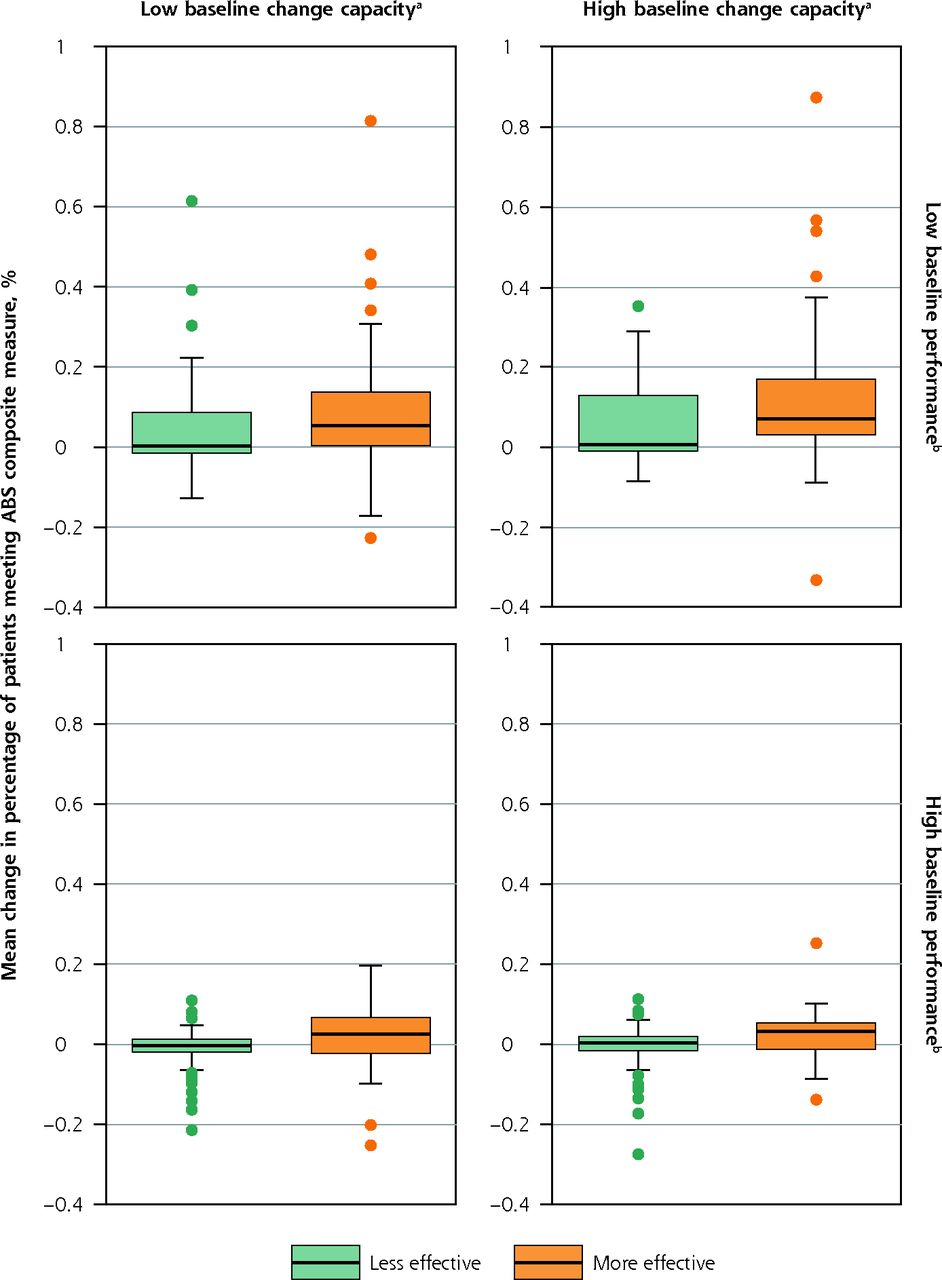
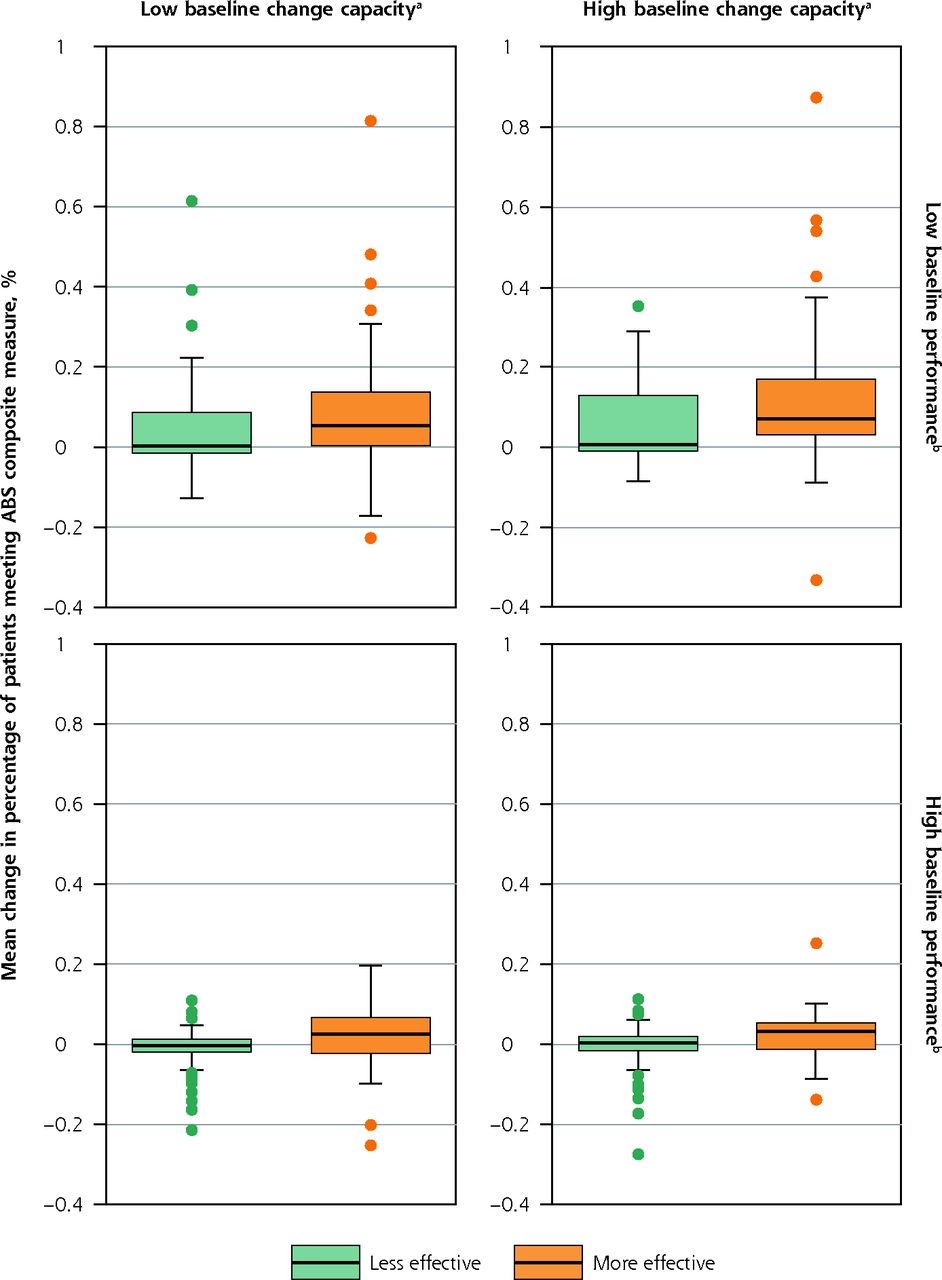
- Figure 2.
Distribution of mean change in ABS composite measure between more and less effective facilitators, stratified by practice baseline change capacity and baseline performance.
ABS = aspirin use, blood pressure control, smoking cessation counseling. CPCQ = Change Process Capability Questionnaire.
Notes: Plots show absolute changes in percentages, so the magnitude of the difference is small, but across the baseline characteristics, practices with more effective facilitators tended to have higher changes in the ABS composite measure.
a Assessed from baseline CPCQ score, dichotomized at the median value as high (score ≥11) or low (score <11).
b Assessed from percentage of patients meeting composite ABS outcome at baseline, dichotomized at the median value as high (≥65%) or low (<65%).
c More effective: ≥75% of facilitator’s practices had improved CPCQ scores and/or ABS performance; less effective: <50% of facilitator’s practices had improved CPCQ scores and/or ABS performance.

Tables
Group and Measure Coop 1 Coop 2 Coop 3 Coop 4 Coop 5 Coop 6 Coop 7 Total Practices Number participating 245 225 274 205 216 211 254 1,630 Number having external facilitator 245 225 274 205 166 211 254 1,580 Facilitators Number 31 17 17 16 15 39 23 158 Number having ≥4 practices 18 16 17 15 12 19 19 116 Effectiveness of facilitators having ≥4 practicesa Number more effective 12 5 6 2 0 6 2 33 Number less effective 2 3 2 2 11 3 7 30 ABS = aspirin use for high-risk patients, blood pressure control, smoking cessation counseling; Coop = cooperative; CPCQ = Change Process Capability Questionnaire.
↵a More effective: ≥75% of facilitator’s practices had improved CPCQ scores and/or ABS performance; less effective: <50% of facilitator’s practices had improved CPCQ scores and/or ABS performance. A total of 53 facilitators who were neither more effective nor less effective were excluded from effectiveness analyses.
Phase and Components Specific Activities Preintervention phase: Sep 2015-Mar 2017 Quantitative data collection Baseline surveys (practice survey, practice member survey) Intervention phase: Dec 2015-Nov 2017 Quantitative data collection: Dec 2015-Nov 2017a Quarterly ABS reports Qualitative data collection: Jul 2016-Apr 2017 Interviews with 80 study participants: 41 Facilitators
39 Leaders of facilitator organizations and cooperatives
Postintervention phase: Nov 2016-Apr 2018 Quantitative data collection: Nov 2016-Dec 2017 Postintervention surveys (practice survey, practice member survey) Qualitative data collection: Sep 2017-Aug 2018 Interviews with 74 facilitators: 28 Previously interviewed during intervention phase
46 Newly interviewed
Analysis phase: Mar 2020-Dec 2021 Quantitative data analyses Analyses of descriptive data from 162 facilitators (158 external, 4 internal) Qualitative data analyses Analyses based on interviews with 36 of 87 facilitators interviewed: 23 More effective facilitators
13 Less effective facilitators
ABS = aspirin use for high-risk patients, blood pressure control, smoking cessation counseling.
↵a The active interventions ranged in duration from 3 to 18 months.
Outcome More Effective Facilitator Less Effective Facilitator All High Capacity Low Capacity High Capacity Low Capacity Change in percentage of patients meeting ABS measurea Aspirin, mean (SD) % 10 (22) 6 (16) 0 (10) 1 (10) 4 (16) Blood pressure, mean (SD) % 4 (14) 2 (14) 2 (9) 2 (13) 2 (13) Smoking, mean (SD) % 11 (17) 9 (22) 1 (14) 0 (11) 6 (18) Change in CPCQ score, mean (SD) pointsb −2.7 (9.8) 17.8 (13.9) −3.1 (9.5) 11.7 (10.6) 5.9 (14.5) ABS = aspirin use for high-risk patients, blood pressure control, smoking cessation counseling; CMS = Centers for Medicare and Medicaid Services; CPCQ = Change Process Capability Questionnaire.
Notes: See Table 1 footnotes for definitions of more and less effective facilitators. See Figure 1 footnotes for definitions of practice baseline change capacity.
↵a Absolute difference between percentage of patients meeting metric at follow-up and at baseline. Theoretical range: −100% (practice went from all eligible patients meeting CMS performance measure at baseline to none at follow-up) to 100% (practice went from no eligible patients meeting CMS performance measure at baseline to all at follow-up).
↵b Difference between score at follow-up and at baseline. Theoretical range following above logic: −56 (practice went from highest to lowest change capacity) to 56 (practice went from lowest to highest change capacity).
- Table 4.
Summary of Strategies Used and Articulation of Strategies by More and Less Effective Facilitators
Facilitator Effectiveness Cultivating Motivation, Tailoring, and Addressing Resistance Guiding Practices Though the Change Process Articulating Strategies to Help Practices More effective Aligned EvidenceNOW work with other payer initiatives or practice goals.
Used formal assessment tools or casual conversations to assess practice readiness to change and QI capacity.
Addressed resistance directly and worked with practice to overcome barriers (eg, suggesting smaller tests of change, working with EHR vendors, helping reallocate tasks among team members).Identified pain points through conversation with the practice and discussed next steps.
Shared ideas from other practices (cross-pollination) such as on workflows and patient education and helped tailor to the local context to make changes appropriate across diverse practice settings.
Provided project management support (eg, agenda setting, note-taking, summarizing action items, assigning tasks to team members, providing reminders).Yes—were able to speak in detail about the work they did in specific practices, how this work was tailored, and which changes likely led to improvements. Less effective Showed less evidence of motivating and tailoring.
Cited practice resistance as preventing work from being done. Described not wanting to push the practice too hard.Held didactic meetings with education alone.
Did the work for the practice.
Presented options for the change process, but did not push the practice to identify their next steps.
Some did not have structured meetings; emphasis was on just being present in the practice.No—when asked about work done in specific practices, answers were limited to the facilitator’s overall approach and to description of presentations and materials used. EHR = electronic health record; QI = quality improvement.
SUPPLEMENTAL DATA IN PDF BELOW
Supplemental Table 1. EvidenceNOW Clinical Quality Outcome Measures
Supplemental Appendix 1. Practice Facilitator In-Person Interview
Supplemental Appendix 2. Practice Facilitator Phone Interview
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Enhancing capability for continuous organisational improvement and learning in healthcare organisations: a systematic review of the literature 2013-2022
- What AHRQ Learned While Working to Transform Primary Care
- Estimating the Cardiovascular Disease Risk Reduction of a Quality Improvement Initiative in Primary Care: Findings from EvidenceNOW
- Estimating the Cardiovascular Disease Risk Reduction of a Quality Improvement Initiative in Primary Care: Findings from EvidenceNOW