
Article Figures & Data
Figures
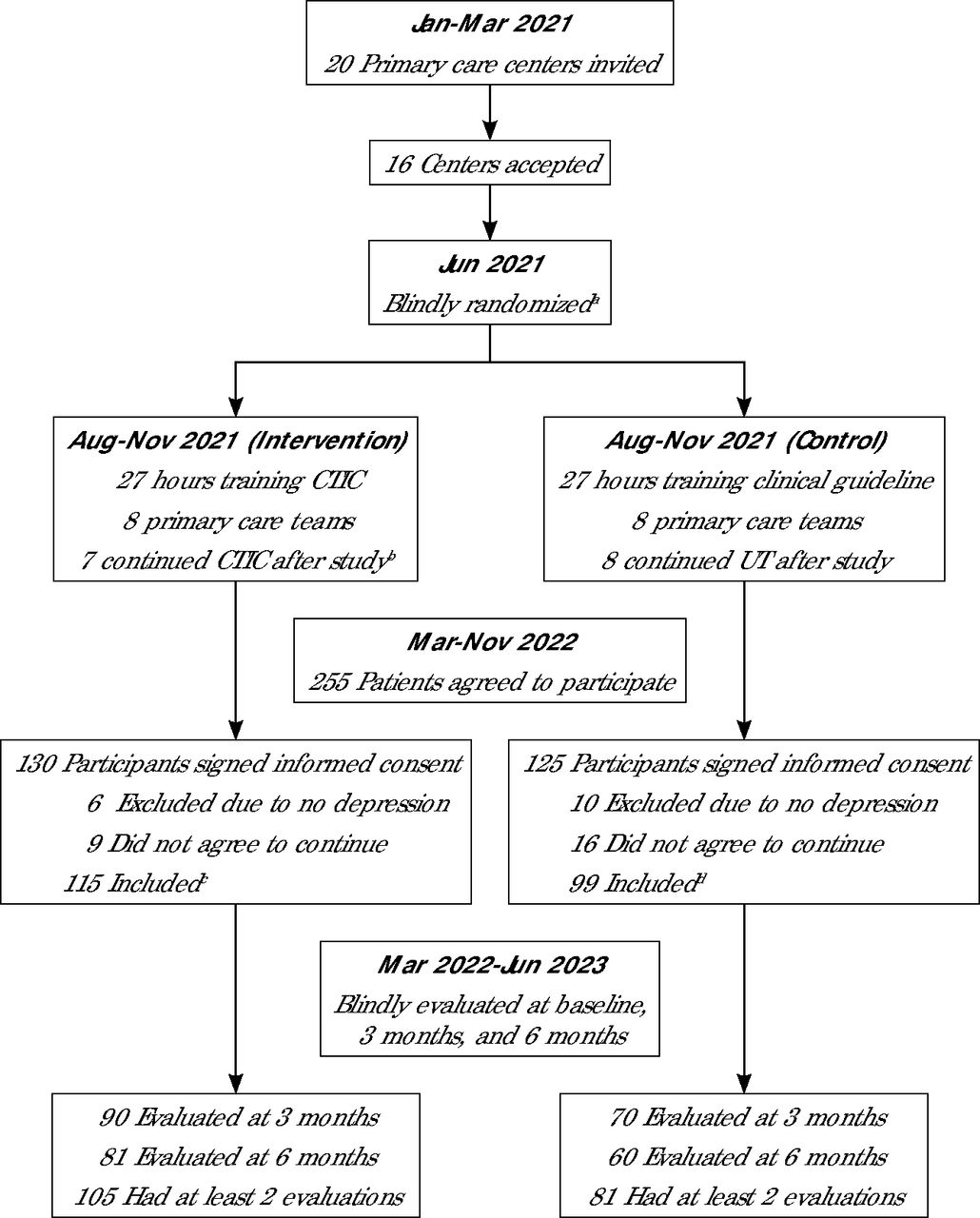
- Figure 1.
Flowchart of recruitment process.
CTIC = collaborative trauma-informed care; UT = usual treatment.
aThe 16 centers were coded with letters A-P, then randomly assigned to the intervention (A, C, G, H, I, K, M, O) and control groups (B, D, E, F, J, L, N, P).
bThe center coded C did not continue to use CTIC procedures after the study.
cNumber of intervention participants by center code was A 13, C 0, G 23, H 18, I 15, K 13, M 10, O 23.
dNumber of control participants by center code was B 14, D 26, E 19, F 9, J 14, L 8, N 9, P 3.
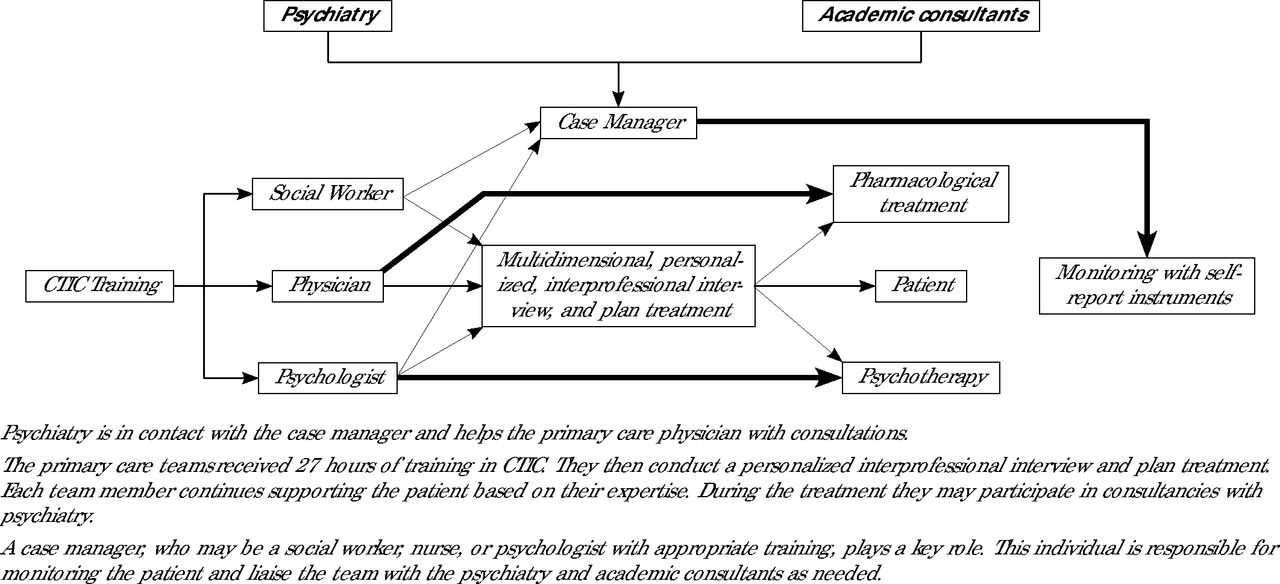
- Figure 2.
Collaborative trauma-informed care for treating depression in primary care.
CTIC = collaborative trauma-informed care.


Tables
Learning Units Main Learning Objectives Framework for CTIC in treating depression Recognize and differentiate the characteristics and treatment challenges associated with complex depression, TRD, and DTD. Trauma-informed care Understand and apply the fundamental principles of trauma-informed care, including its epidemiological foundations, neurobiological mechanisms, and clinical implications to improve diagnosis, treatment, and patient management. Attachment and mentalization in the helping relationship Integrate the concepts of bonding, mentalization, and attachment styles to understand their impact on depression and develop tailored therapeutic strategies. Resilience Understand and apply the concepts of resilience to understand their impact on depression, and develop tailored therapeutic strategies for enhancing patient resilience in treatment plans. Multi-professional comprehensive diagnostic workshop Conduct a multidimensional and interprofessional evaluation of depression cases based on complexity. This includes categorizing the type of depression, evaluating its severity, establishing differential medical and psychiatric diagnoses, and sensitively inquiring into adverse biographical history. Multi-professional comprehensive treatment workshop Develop a comprehensive and multi-professional plan of treatment for depression in primary care based on clinical complexity. Multi-professional comprehensive monitoring workshop Develop a comprehensive and multi-professional monitoring plan for depression in primary care tailored to the clinical complexity. Collaborative model workshop Integrate elements that can be implemented in primary care to support CTIC for depression including use of a case manager, follow-ups with standardized scales, and consultation with psychiatric experts. CTIC - collaborative trauma-informed care; DTD = difficult-to-treat depression; TRD = treatment resistant depression.
Characteristics CTIC Group
(n = 115)UT Group
(n = 99)P Value Female, No. (%) 98 (85.2) 84 (84.8) .49 Age, mean (SD), y 40.2 (13.5) 40.1 (15.8) .94 Educational attainment, No. (%)a .10 Primary 31 (27.4) 20 (20.2) … Secondary 56 (49.5) 30 (30.3) … Higher education 28 (24.3) 9 (9.1) … Current paid employment, No. (%) 46 (40.0) 35 (35.3) .56 Living with family, No. (%) 65 (56.5) 66 (66.7) .60 History of mental illness, No. (%) 74 (65.4) 66 (66.7) .72 History of psychiatric treatment, No. (%) 72 (62.6) 65 (65.6) .64 >3 anxiety comorbidities, No. (%) 27 (23.4) 23 (23.2) .90 History of suicide attempt, No. (%) 37 (32.1) 41 (41.5) .16 ≥4 adverse childhood experiences, No. %) 68 (59.1) 63 (63.9) .49 PHQ-9, mean (SD)b 17.1 (5.7) 17.3 (6.1) .49 GAD-7, mean (SD)c 13.1 (5.1) 13.1 (4.9) .97 DERS, mean (SD)d 78.5 (22.9) 82.5 (22.9) .21 OQ45.2 IR, mean (SD)e 23.2 (8.7) 22.0 (7.3) .30 OQ45.2 SR, mean (SD)f 13.8 (5.7) 14.0 (5.7) .81 CTIC = collaborative trauma-informed care; DERS = difficulties in emotional regulation scale; GAD = generalized anxiety disorder; IR = interpersonal relations; OQ = outcome questionnaire; PHQ= patient health questionnaire; RCT = randomized clinical trial; SR = social role; UT = usual treatment.
NOTE: This RCT was conducted in 16 primary care clinics in the Maule Region of Chile. The CTIC group was the intervention, and the UT group, the control.
↵a Primary is grades 1-8, secondary is grades 9-12, and higher education includes universities, professional institutions, and technical programs.
↵b PHQ-9 score range = 0-27; 7 or more indicates depressive symptoms.
↵c GAD-7 score range = 0-23; 10 or more indicates anxiety symptoms.
↵d DERS score range = 0-140; 73 or more indicates emotion dysregulation.
↵e OQ45.2 PI subscale score range = 0-48; 16 or more indicates interpersonal dysfunctions.
↵f OQ45.2 SR subscale score range = 0-36; 14 or more indicates social dysfunctions.
- Table 3.
Longitudinal Assessment Intervention vs Control Groups at Baseline, 3 Months, and 6 Months
Outcomes CTIC Group UT Group Time Time/Group Mean (SD) 3 Months No. Mean (SD) 6 Months No. Mean (SD) Baseline No. Mean (SD) 3 Months No. Mean (SD) 6 Months No. Mean (SD) Eta2 P Value Eta2 P Value Primary PHQ-9a 115 17.1 (5.7) 90 11.4 (7.1) 81 8.9 (6.6) 99 17.3 (6.1) 70 13.8 (8.1) 60 12.2 (8.1) 0.34 .050 0.01 .014 Secondary GAD-7b 115 13.1 (5.2) 90 10.5 (5.3) 81 9.3 (5.7) 99 13.1 (4.9) 70 11.4 (5.6) 60 10.8 (6.3) 0.14 .020 0.01 .055 DERSc 113 78.5 (22.9) 86 71.5 (25.2) 77 64.6 (24.9) 96 82.5 (22.9) 68 74.3 (28.2) 56 69.3 (25.6) 0.16 .030 0.01 .500 OQ45.2 IRd 114 23.2 (8.7) 86 20.8 (9.7) 77 19.1 (9.4) 98 22.0 (7.3) 69 20.7 (8.6) 57 19.7 (8.1) 0.07 .005 0.01 .300 OQ45.2 RSe 114 13.8 (5.7) 86 12.2 (5.9) 77 11.4 (6.2) 98 14.0 (5.7) 69 13.7 (6.7) 57 12.8 (6.5) 0.04 .012 0.01 .112 CTIC = collaborative trauma-informed care; DERS = difficulties in emotional regulation scale; Eta2 = η2 correlation coefficient; GAD = generalized anxiety disorder; IR= interpersonal relations; OQ = outcome questionnaire; PHQ= patient health questionnaire; SR = social role; UT = usual treatment.
NOTE: The CTIC group was the intervention, and the UT group, the control.
↵a PHQ-9 score range = 0-27; 7 or more indicates depressive symptoms.
↵b GAD-7 score range = 0-23; 10 or more indicates anxiety symptoms.
↵c DERS score range = 0-140; 73 or more indicates emotion dysregulation.
↵d OQ45.2 PI subscale score range = 0-48; 16 or more indicates interpersonal dysfunctions.
↵e OQ45.2 SR subscale score range = 0-36; 14 or more indicates social dysfunctions.
- Table 4.
Comparative ITT Analysis of Intervention vs Control Groups: Impact on Outcomes and Adherence at 6 Months
Outcomes CTIC Group UT Group Comparison Intracluster Coefficient No. Mean (SD) No. Mean (SD) AMD (95% CI) P Value Effect Size (95% CI) Baseline 6 months Primary PHQ-9a 115 8.9 (6.6) 99 12.2 (8.1) −3.09 (−4.94 to −1.23) .001 −0.46 (−073 to −0.18) 0.06 0.10 Secondary GAD-7b 115 9.3 (5.7) 99 10.8 (6.3) − 1.50 (− 3.03 to 0.31) .055 −0.25 (−0.52 to 0.02) 0.05 0.05 DERSc 113 64.6 (25.0) 96 69.3 (25.6) −2.40 (−8.35 to 3.54) .427 −0.19 (−0.46 to 0.09) 0.06 0.08 OQ-45.2 IRd 114 19.1 (9.4) 98 19.7 (8.1) −1.12 (−3.27 to 1.03) .307 −0.06 (−0.34 to 0.20) 0.12 0.08 OQ-45.2 SRe 114 11.4 (6.2) 98 12.8 (6.5) −1.26 (−2.81 to 0.29) .112 −0.21 (−0.48 to 0.06) 0.07 0.06 GHASf 104 31.7 (9.9) 79 29.0 (9.8) 2.59 (1.82 to 4.99) .035 −0.00 (−0.43 to 0.30) 0.10 0.11 AMD = adjusted mean difference; CTIC = collaborative trauma-informed care; DERS = difficulties in emotional regulation scale; GAD = generalized anxiety disorder; GHAS = general health adherence scale; IP = interpersonal; ITT = intention to treat; OQ = outcome questionnaire; PHQ= patient health questionnaire; SR = social role; UT = usual treatment.
NOTE: The CTIC group was the intervention, and the UT group, the control.
↵a PHQ-9 score range = 0-27; 7 or more indicates depressive symptoms.
↵b GAD-7 score range =0-23; 10 or more indicates anxiety symptoms.
↵c DERS score range = 0-140; 73 or more indicates emotion dysregulation.
↵d OQ45.2 PI subscale score range = 0-48; 16 or more indicates interpersonal dysfunctions.
↵e OQ45.2 SR subscale score range = 0-36; 14 or more indicates social dysfunctions.
↵f GHAS score range = 0-36; 24 or less is low, 25-30 is moderate, and 31 or more is high adherence.
SUPPLEMENTAL MATERIALS IN PDF FILE BELOW
Supplemental Appendix. XVII Contest for Health Research and Development Projects: Design, Implementation and Evaluation of the Effectiveness of a Multidimensional Collaborative Model to Improve the Resolution of Depression in Primary Care Teams in the Maule Region
VISUAL ABSTRACT IN PDF FILE BELOW
PLAIN-LANGUAGE ARTICLE SUMMARY AND VISUAL ABSTRACT
Original Research
Collaborative, Trauma-Informed Care Improves Depression Outcomes in Primary Care
Background and Goal: Depression is a major public health issue in Chile, affecting women at twice the rate of men. During the COVID-19 pandemic, depressive symptoms rose sharply, stressing the need for more effective care in primary care settings. Many patients experience complex forms of depression that are linked to trauma and other challenges, which standard treatments often fail to address. This study aimed to assess whether a collaborative, trauma-informed care model could improve outcomes for patients with depression compared to usual treatment in primary care clinics in Chile.
Study Approach: The study was a cluster randomized controlled trial conducted with 16 primary care teams in the Maule Region, Chile, from August 2021 to June 2023. Clinics were randomly assigned to either the collaborative, trauma-informed care model or usual treatment model. Collaborative, trauma-informed care model teams consisted of a physician, a psychologist, and a social worker, all trained in trauma-informed care and in managing difficult-to-treat depression. Usual treatment teams, consisting of primary care professionals, followed current national guidelines for depression treatment.
A total of 214 adult patients between 18 and 70 years old with diagnosed depression were recruited and monitored over a six-month period, with evaluations at three and six months.
Main Results:214 patients were recruited, 85% women, with 61.2% having 4 or more adverse childhood experiences.
-
Depression scores dropped significantly in both groups, but the collaborative trauma-informed care model group saw a greater reduction—from 17.1 to 8.9—compared to the usual treatment group, which improved from 17.3 to 12.2. (P < 0.001).
-
At six months, 62 out of 115 patients (54%) in the collaborative trauma-informed care model group showed remission, compared to 34 out of 99 patients (34%) in the usual treatment group. (p = 0.001)
-
Patients in the collaborative trauma-informed care model group had higher treatment adherence.
-
Both the collaborative trauma-informed care model and usual treatment groups showed improvements in anxiety, social functioning, and emotional regulation, but no significant differences were found between groups in these areas.
Why It Matters: This study demonstrates the effectiveness of integrating trauma-informed care into a collaborative care model for treating depression in primary care. By addressing complex forms of depression, particularly those complicated by past trauma, this approach showed significant improvements in patient outcomes. The findings suggest that this model can offer a more comprehensive and effective solution for treating difficult-to-manage depression.
Effectiveness of Collaborative, Trauma-Informed Care on Depression Outcomes in Primary Care: A Cluster Randomized Control Trial in Chile
Verónica G. Vitriol, MD, Mg, et al
University of Talca Medical School, Talca, Chile
Visual Abstract
-

In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.