
Article Figures & Data
Figures
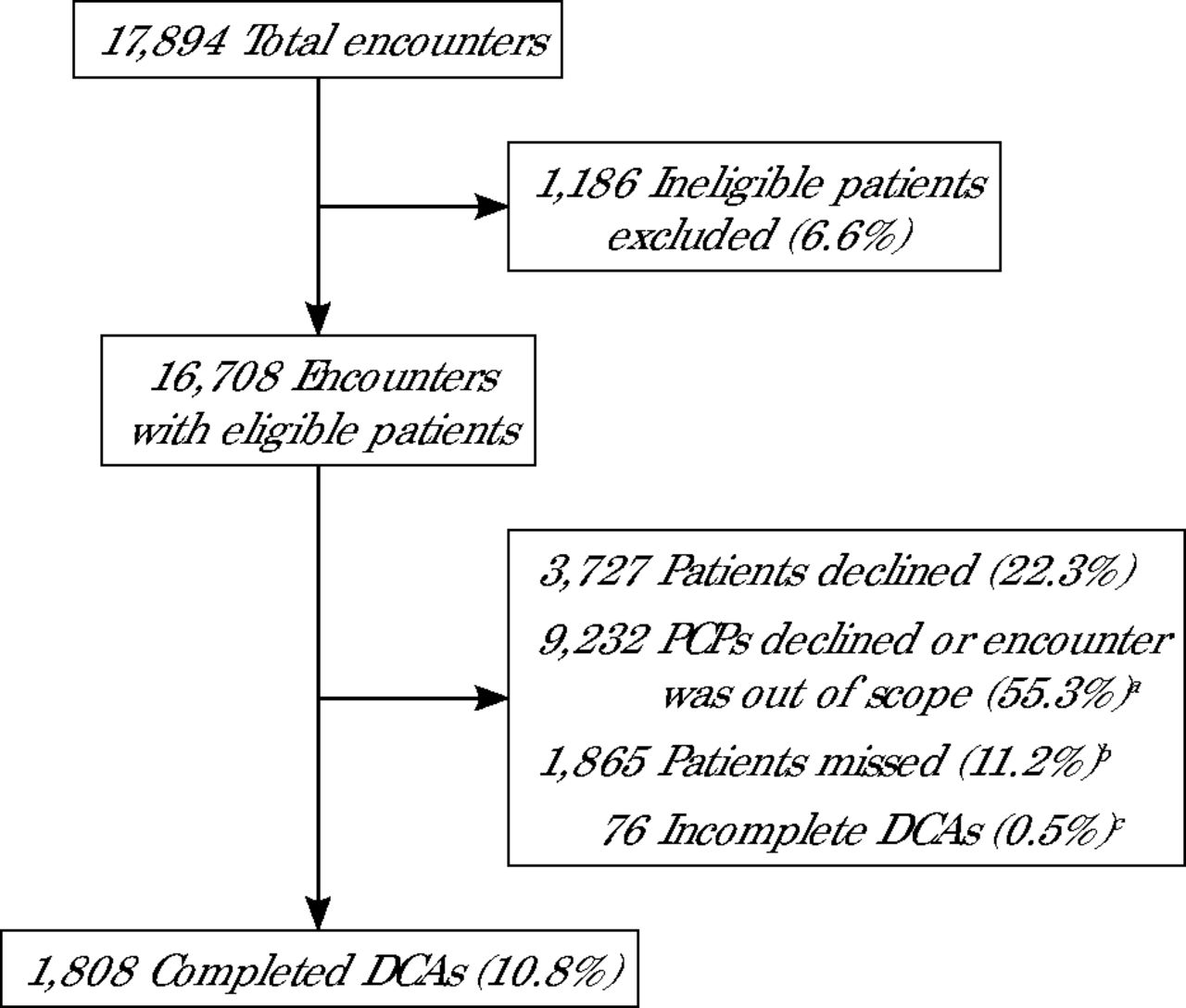
- Figure 1.
Feasibility and Acceptability of Digital Cognitive Assessment Implementation
DCA = digital cognitive assessment; PCP = primary care physician.
a For each encounter, the PCP could decline to have the patient complete the DCA, and as different clinics rolled out the DCA screening, some encounters were defined as out of scope on the basis of clinic-specific workflows and perceived system constraints.
b Missed: patient was eligible to complete the DCA but was not approached.
c Incomplete: patient started the DCA but did not complete enough of the test to produce a score.

Tables
- Table 1.
Examples of Implementation Differences by Clinics, Which Defined Out-of-Scope Encounters
Sprint topic Example Timing of DCA administration during encounter/visit DCA administered before clinician entered examination room vs after clinician finished in examination room Types of encounters/visits for which DCA would be administered DCA administered for specific encounter types (eg, annual wellness visit, preventive visit) vs for all encounter types Specific appointment times when DCA would be administered DCA administered for appointments at specific times in the schedule each day vs at any appointment time Clinic personnel who would administrator DCA during encounter/visit DCA administered by medical assistant vs primary care clinician DCA = digital cognitive assessment.
- Table 2.
Demographic Characteristics of Unique Patients Approached to Complete a Digital Cognitive Assessment
Did not complete DCAa n = 8,675 Completed DCA n = 1,722 P value Age, y, mean (SD) 74.7 (7.4) 73.5 (6.0) <.001 Sex, No. (%) Female 5,156 (59.4) 995 (57.8) .21 Male 3,518 (40.6) 727 (42.2) Race, No. (%) <.001 Asian 219 (2.5) 23 (1.3) Black or African American 1,553 (17.9) 336 (19.5) White 6,801 (78.4) 1,355 (78.7) Other reported 82 (0.9) 5 (0.3) Ethnicity, No. (%) .07 Hispanic 194 (2.2) 51 (3.0) Non-Hispanic 8,414 (97.0) 1,663 (96.6) Area Deprivation Index median, (25%, 75%) 54 (35, 74) 51 (29, 76) .027 Clinic, No. (%) <.001 1 1,146 (13.2) 282 (16.4) 2 1,737 (20.0) 36 (2.1) 3 306 (3.5) 41 (2.4) 4 1,198 (13.8) 459 (26.7) 5 641 (7.4) 410 (23.8) 6 1,049 (12.1) 475 (27.6) 7 2,598 (29.9) 19 (1.1) DCA = digital cognitive assessment.
↵a Patients who did not complete a DCA included those who had a status of ineligible, patient declined, physician declined or out of scope, missed or not performed reason unknown, or incomplete.
- Table 3.
Logistic Regression Comparing Patients Who Completed a Digital Cognitive Assessment vs Patients Who Did Not
OR (95% CI) P value Age 0.98 (0.97, 0.99) <.001 Sex Female 1.12 (1.00, 1.26) .053 Race Asian vs White 0.46 (0.29, 0.73) .001 Black or African American vs White 0.91 (0.75, 1.09) .294 Other race vs White 0.28 (0.11, 0.72) .008 Ethnicity Hispanic vs Non-Hispanic 0.96 (0.67, 1.38) .821 Area Deprivation Index 1.00 (1.00, 1.00) .551 Clinic 1 vs 3 1.84 (1.28, 2.63) .001 2 vs 3 0.15 (0.09, 0.24) <.001 4 vs 3 2.90 (2.03, 4.14) <.001 5 vs 3 4.82 (3.36, 6.92) <.001 6 vs 3 3.28 (2.29, 4.69) <.001 7 vs 3 0.05 (0.03, 0.10) <.001 OR = odds ratio.
Unimpaired (n = 762) Borderline (n = 628) Impaired (n = 236) Inconclusivea (n = 96) P value Age, y, mean (SD) 72.1 (5.0) 74.2 (6.2) 76.2 (7.2) 73.2 (6.3) <.001 Sex, No. (%) .064 Female 456 (59.8) 367 (58.4) 121 (51.3) 51 (53.1) Male 306 (40.2) 261 (41.6) 115 (48.7) 45 (46.9) Race, No. (%) <.001 Asian 2 (0.3) 10 (1.6) 8 (3.4) 3 (3.1) Black or African American 79 (10.4) 142 (22.6) 88 (37.3) 27 (28.1) White 678 (89.0) 473 (75.3) 139 (58.9) 65 (67.7) Other reported 0 (0) 3 (0.5) 1 (0.4) 1 (1.0) Ethnicity, No. (%) .001 Hispanic 11 (1.4) 25 (4.0) 14 (5.9) 1 (1.0) Non-Hispanic 746 (97.9) 601 (95.7) 222 (94.1) 94 (97.9) Years of education, mean (SD) 15.1 (2.4) 14.1 (2.7) 12.8 (3.1) 13.5 (2.5) <.001 Area Deprivation Index, median (25%, 75%) 43 (28, 63) 55 (33, 81) 63 (43, 87) 52 (28, 88) <.001 Charlson Comorbidity Index, median (25%, 75%) 1 (0, 1) 1 (0, 2) 1 (0, 3) 1 (0, 2) <.001 Comorbidities, No. (%) Hypertension 544 (71.4) 520 (82.8) 197 (83.5) 84 (87.5) <.001 Hyperlipidemia 434 (57.0) 356 (56.7) 127 (53.8) 52 (54.2) .685 Chronic kidney disease 107 (14.0) 128 (20.4) 59 (25.0) 20 (20.8) <.001 Diabetes 220 (28.9) 221 (35.2) 94 (39.8) 36 (37.5) .002 Congestive heart failure 47 (6.2) 75 (11.9) 30 (12.7) 11 (11.5) <.001 COPD 119 (15.6) 120 (19.1) 42 (17.8) 20 (20.8) .225 Obstructive sleep apnea 110 (14.4) 74 (11.8) 26 (11.0) 14 (14.6) .219 Obesity 186 (24.4) 113 (18.0) 54 (22.9) 21 (21.9) .014 Cancer 63 (8.3) 61 (9.7) 23 (9.7) 11 (11.5) .594 Tobacco use, No. (%) (some with missing values) .004 Current 38 (6.7) 52 (11.3) 19 (10.9) 4 (6.4) Former 124 (22.0) 127 (27.7) 49 (28.2) 12 (19.0) Never 402 (71.3) 280 (61.0) 106 (60.9) 47 (74.6) COPD = chronic obstructive pulmonary disease; DCA = digital cognitive assessment.
↵a Patients categorized as inconclusive if they completed a DCA that could not be scored and determined by Linus Health as an inconclusive result, and were not included in the statistical analysis.
Borderline (n = 628) Impaired (n = 236) P value New diagnosis of ADRD, No. (%) 4 (0.6) 5 (2.1) .068 New diagnosis of MCI, No. (%) 9 (1.4) 12 (5.1) .005 New antidementia drug ordered, No. (%)a 3 (0.5) 6 (2.5) .015 Order for laboratory test, No. (%) Vitamin B12 139 (22.1) 85 (36.0) <.001 TSH 188 (29.9) 84 (35.6) .119 Order for imaging of head/neck, No. (%) Any type of imaging 48 (7.6) 40 (16.9) <.001 CT 24 (3.8) 22 (9.3) .003 MRA 2 (0.3) 0 (0) 1.000 MRI 29 (4.6) 22 (9.3) .014 Referral to neurology, No. (%) 25 (4.0) 28 (11.9) <.001 Referral to geriatrics, No. (%) 4 (0.6) 8 (3.4) .005 Referral to neuropsychology, No. (%) 3 (0.5) 5 (2.1) .039 Referral to psychiatry, No. (%) 1 (0.2) 0 (0) 1.000 Referral to brain health navigator RN, No. (%) 299 (47.6) 148 (62.7) <.001 Died, No. (%) 4 (0.6) 2 (0.8) .667 ADRD = Alzheimer disease or a related dementia; CT = computed tomography; MCI = mild cognitive impairment; MRA = magnetic resonance angiogram; MRI = magnetic resonance imaging; RN = registered nurse; TSH = thyroid-stimulating hormone.
↵a Donepezil, galantamine, rivastigmine, tacrine, memantine, memantine/donepezil.
PLAIN-LANGUAGE SUMMARY
Original Research
Digital Cognitive Assessment in Primary Care May Enable Early Dementia Detection and Next Step Care
Background and Goal: Many adults aged 65 and older never receive a cognitive check during regular primary care visits. This study assessed the feasibility and acceptability of implementing a digital cognitive assessment for Alzheimer disease and related dementias (ADRD) screening into primary care. They also assessed the prevalence of positive screens and measured diagnostic and care outcomes after a positive digital cognitive assessment result.
Study Approach: From June 2022 to May 2023, seven Indiana University Health clinics offered the five-minute Digital Clock & Recall test on an iPad to every patient 65 and older. Each site, after a series of pre-launch “sprint” meetings, set its own rules on which visit types and which staffers would run the screen, then uploaded results to the electronic record for the physician to review. In month three, researchers introduced a registered-nurse role to support patients for completing care pathways if they were flagged for cognitive impairment. Physicians retained discretion over follow-up, and investigators recorded every lab, imaging study, referral and new diagnosis ordered within 90 days of the screen.
Main Results
-
Of the 16,708 patients who were identified as eligible for screening, a total of 1,808 digital cognitive assessments (10.8%) were completed by 1,722 unique patients.
-
More than one-half (55.3%) of eligible visits never offered the digital cognitive assessment because PCPs declined or the encounter was deemed out of scope during sprint meetings.
-
Screening outcomes: Among 1,808 tests, 44.3% were categorized as unimpaired, 36.5% as borderline, and 13.7% as impaired.
-
Follow-up within 90 days for the impaired group: 2.1% received a new Alzheimer or related-dementia diagnosis; 5.1% received a new mild cognitive impairment diagnosis; 16.9% had brain imaging ordered; 62.7% were referred to the brain health navigator.
Why It Matters: Many cases of cognitive impairment go undetected in primary care. Digital cognitive assessments may offer a feasible way to screen older adults during routine visits, helping identify those who may benefit from early diagnosis, treatment, and care planning. However, without supportive workflows and follow-up systems in place, these tools alone aren’t enough to close the gap in dementia care.
Feasibility and Acceptability of Implementing a Digital Cognitive Assessment for Alzheimer Disease and Related Dementias in Primary Care
Nicole R. Fowler, PhD, MHSA, et al
Department of Medicine, Indiana University School of Medicine, Indianapolis, Indiana
-




{kind=link}