
Article Figures & Data
Figures
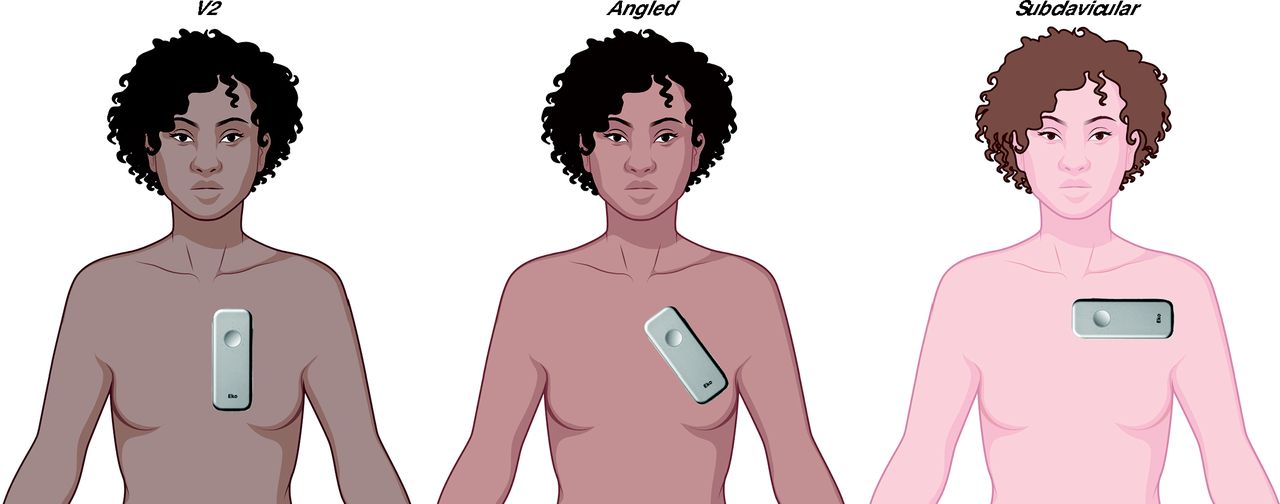
- Figure 1.
Digital Stethoscope Recording Positions
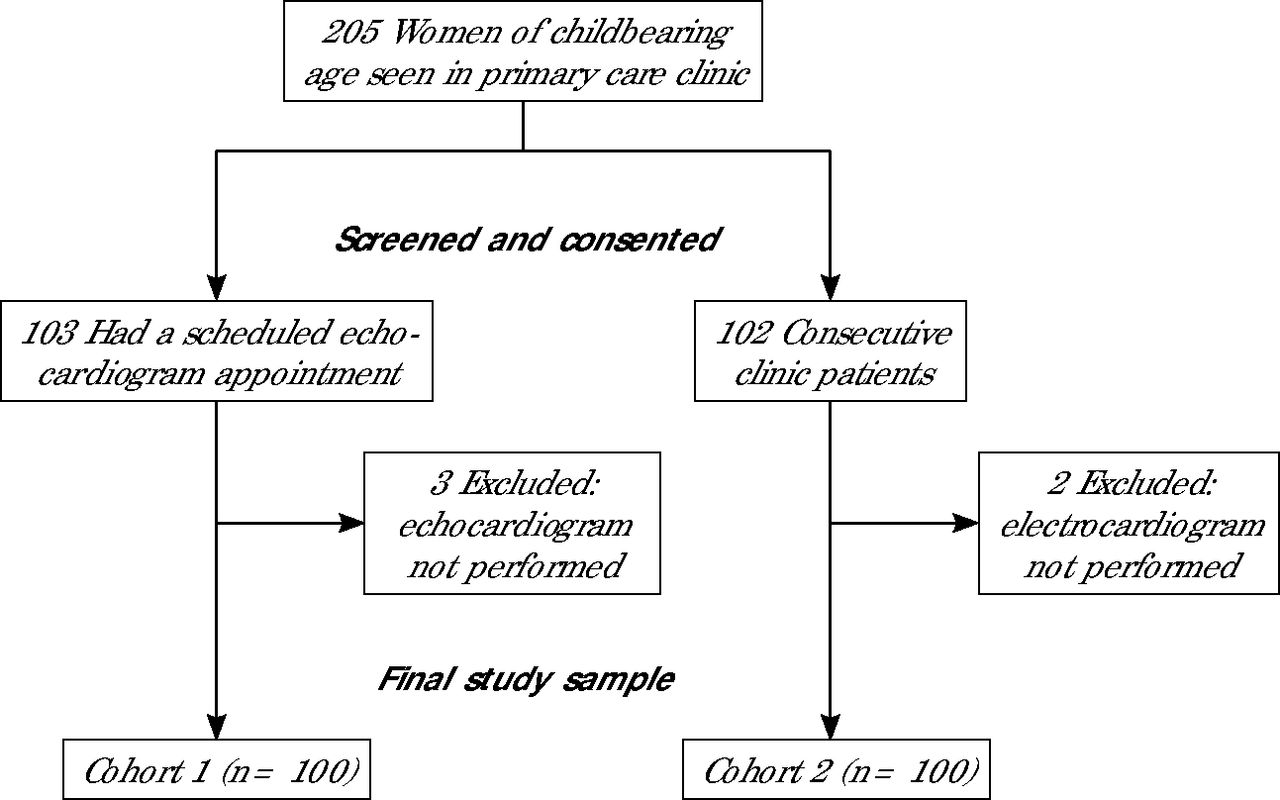
- Figure 2.
Study Flow Diagram
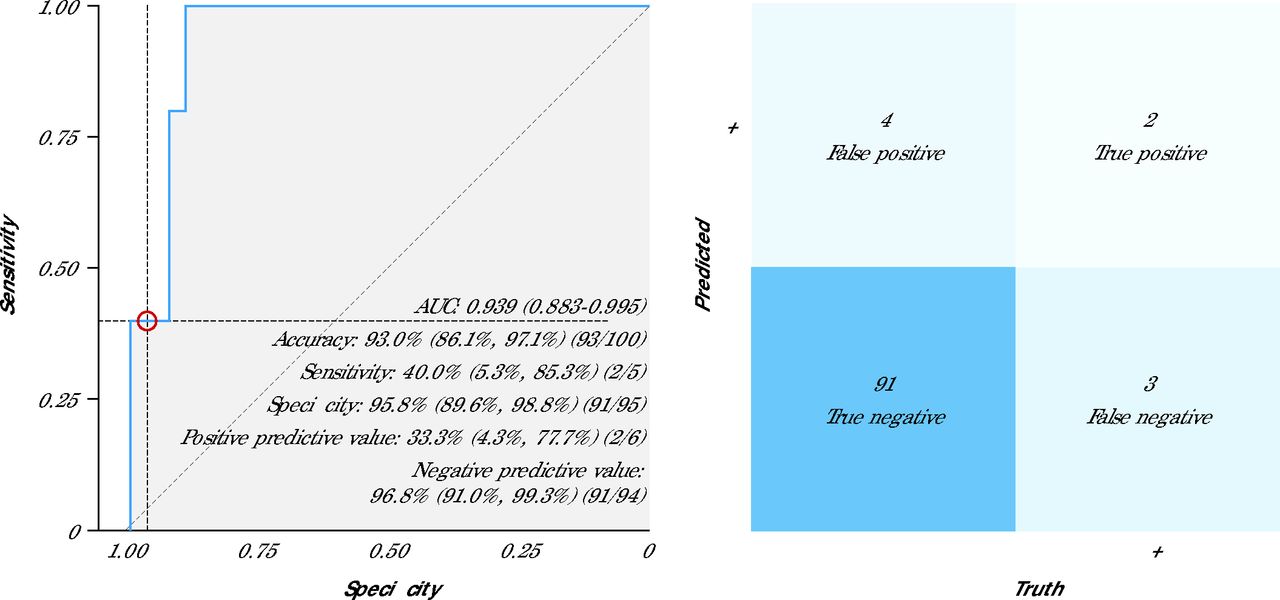
- Figure 3.
Receiver Operating Characteristic Curve and Confusion Matrix for 12-Lead ECG
AI = artificial intelligence; AUC = area under the curve; ECG = electrocardiography; ROC = receiver operating characteristic curve.
Note: The panel on the left shows the ROC curve and diagnostic performance metrics of the AI-ECG model based on 12-lead ECGs. Data are presented as % (95% CI). The panel on the right shows the associated confusion matrix comparing dichotomous AI prediction results with the ground truth (ECG results).
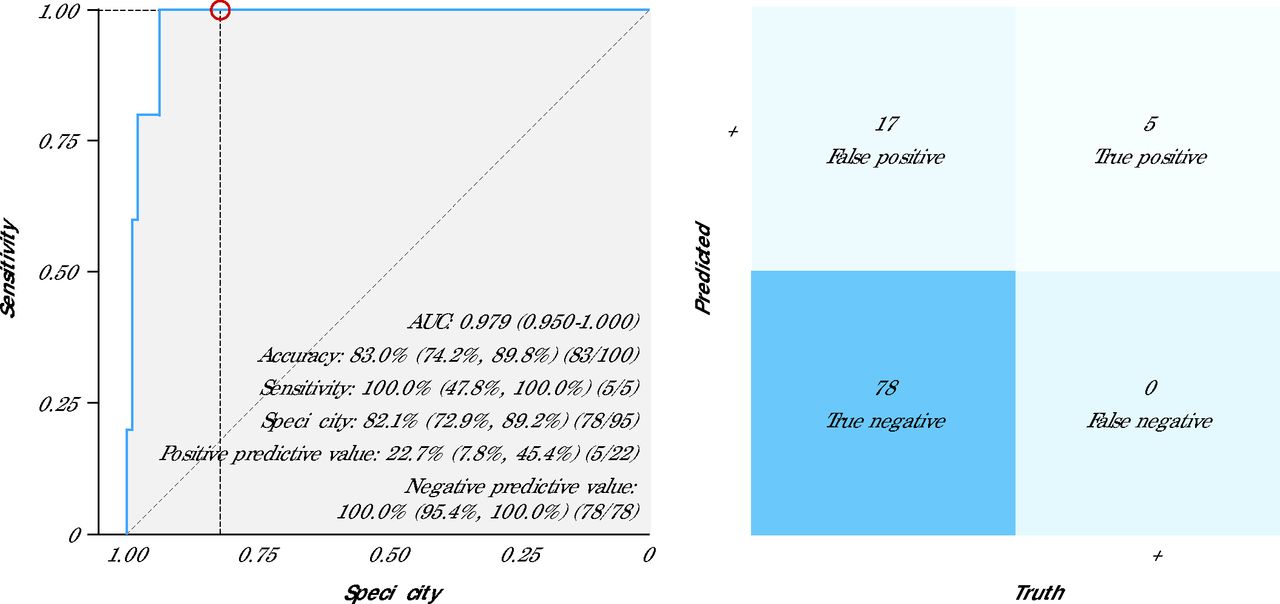
- Figure 4.
Receiver Operating Characteristic Curve and Confusion Matrix for Digital Stethoscope (Maximum Prediction)
AI = artificial intelligence; AUC = area under the curve; ECG = electrocardiography; ROC = receiver operating characteristic curve.
Note: The panel on the left shows the ROC curve and diagnostic performance metrics of the AI-stethoscope model (maximum prediction). Data are presented as % (95% CI). The panel on the right shows the associated confusion matrix comparing dichotomous AI-stethoscope prediction results with the ground truth (ECG results).




Tables
Characteristic Cohort 1 n = 100 Cohort 2 n = 100 Total N = 200 P Valuea Age at ECG, median (Q1, Q3) 40.5 35.6 38.6 .041 (32.5, 45.7) (28.5, 44.0) (30.3, 45.5) Gender, no. (%) 1.00 Female 99 (99.0) 100 (100.0) 199 (99.5) Transgender 1 (1.0) 0 (0) 1 (0.5) Race/ethnicity, no. (%) .044 Hispanic/Latino 9 (9.0) 14 (14.0) 23 (11.5) Non-Hispanic Black 17 (17.0) 9 (9.0) 26 (13.0) Non-Hispanic White 73 (73.0) 70 (70.0) 143 (71.5) Other/multiracial 1 (1.0) 7 (7.0) 8 (4.0) Pregnancy status, no. (%) .76 Not pregnant 95 (95.0) 97 (97.0) 192 (96.0) Pregnant 3 (3.0) 2 (2.0) 5 (2.5) Postpartum (≤12 mo) 2 (2.0) 1 (1.0) 3 (1.5) Clinical comorbid conditions, no. (%) Cancer 6 (6.0) 2 (2.0) 8 (4.0) .28 Cerebrovascular disease 5 (5.0) 1 (1.0) 6 (3.0) .21 Chronic pulmonary disease 17 (17.0) 15 (15.0) 32 (16.0) .85 Congestive heart failure 18 (18.0) 0 (0) 18 (9.0) <.001 Diabetes 7 (7.0) 2 (2.0) 9 (4.5) .17 Diabetes with organ damage 3 (3.0) 0 (0) 3 (1.5) .25 Hypertension 20 (20.0) 12 (12.0) 32 (16.0) .18 Moderate to severe liver disease 4 (4.0) 0 (0) 4 (2.0) .12 Moderate to severe renal disease 19 (19.0) 1 (1.0) 20 (10.0) <.001 Myocardial infarction 4 (4.0) 1 (1.0) 5 (2.5) .37 Peripheral vascular disease 4 (4.0) 2 (2.0) 6 (3.0) .68 Rheumatologic disease 5 (5.0) 3 (3.0) 8 (4.0) .72 Ulcer 2 (2.0) 3 (3.0) 5 (2.5) 1.00 ECG = electrocardiography; Q = quartile.
↵a Fisher exact test.
Note: Cohort 1 participants were consecutive primary care clinic patients already scheduled/referred for echocardiography as part of their ongoing medical care, and cohort 2 participants were recruited consecutively at an outpatient primary care clinic.
- Table 2.
Echocardiographic Parameters Stratified by Left Ventricular Ejection Fraction Among Participants in Cohort 1
Echocardiographic parameter LVEF ≥50% LVEF <50% Total P Value n Median (Q1, Q3) n Median (Q1, Q3) N Median (Q1, Q3) BMI (kg/m2) 95 27.2 (23.0, 31.8) 5 34.3 (23.4, 38.9) 100 27.2 (23.0, 32.7) .35 Heart rate 95 76.0 (67.0, 84.0) 5 82.0 (64.0, 85.0) 100 76.0 (66.8, 84.0) 1.00 LV end-diastolic diameter (mm) 95 44.0 (42.0, 48.0) 5 59.0 (58.0, 65.0) 100 45.0 (42.0, 49.0) < .001 LV end-systolic diameter (mm) 95 29.0 (26.5, 32.0) 5 52.0 (47.0, 53.0) 100 29.5 (27.0, 32.0) < .001 Mitral valve E/e` ratioa 94 8.5 (6.7, 10.0) 4 20.0 (12.3, 26.2) 98 8.6 (6.7, 10.7) .032 Cardiac output (L/min) 88 5.5 (4.7, 6.3) 5 5.2 (4.1, 5.3) 93 5.5 (4.6, 6.3) .31 Cardiac index (L/min/m2) 88 2.9 (2.6, 3.5) 5 2.6 (2.5, 2.9) 93 2.9 (2.6, 3.4) .12 LV geometry 95 No. (%) 5 No. (%) 100 No. (%) < .001 Concentric hypertrophy 10.0 (10.5) 0 (0) 10.0 (10.0) Concentric remodeling 30.0 (31.6) 0 (0) 30.0 (30.0) Eccentric hypertrophy 3.0 (3.2) 4.0 (80.0) 7.0 (7.0) Normal geometry 52.0 (54.7) 1.0 (20.0) 53.0 (53.0) BMI = body mass index; LV = left ventricular; LVEF = left ventricular ejection fraction; Q = quartile.
↵a Mitral valve E/e` ratio was calculated as mitral valve early diastolic filling velocity E (meters/second) divided by medial mitral annulus early diastolic velocity by tissue Doppler e’ (meters/second).
- Table 3.
Measures of Diagnostic Accuracy for AI Models for Cardiomyopathy Detection Based on Standard 12-Lead ECG and Digital Stethoscope Recordings
na AUC (95% CI) Sensitivity, % (95% CI) Specificity, % (95% CI) Accuracy, % (95% CI) F1 score Negative predictive value, % (95% CI) Odds ratio Positive predictive value, % (95% CI) 12-lead ECG (LVEF <50%) AI-ECG 100 0.939
(0.883-0.995)40.0
(5.3-85.3)95.8
(89.6-98.8)93.0
(86.1-97.1)36.4 96.8
(91.0-99.3)15.2
(2.0-117.9)33.3
(4.3-77.7)Digital stethoscope ECG + PCG (LVEF < 50%) Angled 99 0.983
(0.955-1.000)80.0
(28.4-99.5)93.6
(86.6-97.6)92.9
(86.0-97.1)53.3 98.9
(93.9-100.0)58.7
(5.6-610.4)40.0
(12.2-73.8)Subclavicular 96 0.857
(0.672-1.000)60.0
(14.7-94.7)90.1
(82.1-95.4)88.5
(80.4-94.1)35.3 97.6
(91.7-99.7)13.7
(2.0-92.9)25.0
(5.5-57.2)V2 100 0.949
(0.871-1.000)80.0
(28.4-99.5)91.6
(84.1-96.3)91.0
(83.6-95.8)47.1 98.9
(93.8-100.0)43.5
(4.3-437.3)33.3
(9.9-65.1)Mean prediction 100 0.971
(0.929-1.000)60.0
(14.7-94.7)93.7
(86.8-97.6)92.0
(84.8-96.5)42.9 97.8
(92.3-99.7)22.2
(3.1-159.7)33.3
(7.5-70.1)Maximum prediction 100 0.979
(0.950-1.000)100.0
(47.8-100.0)82.1
(72.9-89.2)83.0
(74.2-89.8)37.0 100.0
(95.4-100.0)49.3
(2.6-934.3)22.7
(7.8-45.4)AI = artificial intelligence; AUC = area under the curve; ECG = electrocardiography; LVEF = left ventricular ejection fraction; PCG = phonocardiogram.
↵a Results shown represent available AI prediction results based on diagnostic-quality ECG/phonocardiography. Missing or recorded ECG/phonocardiography data deemed to be of poor quality were excluded from analysis, resulting in a sample size <100 for some of the digital stethoscope recording locations.
VISUAL ABSTRACT IN PDF FILE BELOW
- Adedinsewo_VA_23_3_Final_v2.pdf -
PDF file
- Adedinsewo_VA_23_3_Final_v2.pdf -
PLAIN-LANGUAGE SUMMARY
Original Research
AI-Enabled Tools for Cardiovascular Screening Show Promise in Identifying Heart Dysfunction in Women of Reproductive Age
Background and Goal:Cardiomyopathy, a disease that weakens the heart muscle and makes it harder to pump blood, is a major health threat during pregnancy and accounts for 40% to 60% of late maternal deaths. This study evaluated the performance of an artificial intelligence–enabled electrocardiogram (AI-ECG) and an AI-powered digital stethoscope to see how well they could detect early signs of heart dysfunction in women of reproductive age.
Study Approach: In this cross-sectional pilot study, researchers examined two groups of women aged 18 to 49 who were considering pregnancy. Women who were currently pregnant or within one year postpartum were also included. The first group included 100 women who were already scheduled for an echocardiogram. The second group of women had no indication for an echocardiogram and were seen at a primary care appointment for routine care. All participants received two tests: a standard 10-second 12-lead electrocardiogram (ECG) and a digital stethoscope recording that captured a 15-second, single-lead ECG and phonocardiogram (heart sounds) from up to three locations on the chest. AI models analyzed the ECG and stethoscope recordings to estimate each participant’s risk of having left ventricular systolic dysfunction (LVSD), a type of heart dysfunction. In the second group, patients flagged with LVSD by the 12-lead ECG were then referred to an echocardiogram.
Main Results:
Group 1 (diagnostic cohort, women scheduled for echocardiograms):
-
5% of women had LVSD.
-
Negative results were highly reliable, with the AI-ECG showing a negative predictive value of 96.8% and the AI-stethoscope achieving 100%.
-
Among women who screened positive using the AI tools, 33.3% (using the AI-ECG) and 22.7% (using the AI-stethoscope) truly had LVSD.
Group 2 (screening cohort, women seen during routine primary care visits):
-
Using the AI-ECG, only 1% of women in this low-risk sample screened positive. A follow-up echocardiogram in that patient showed a normal ventricular ejection fraction. With the AI-stethoscope, 3.2% of the sample had a positive screen.
Why It Matters:Many women of reproductive age do not receive routine heart screening before pregnancy. The findings from this study highlight the potential of quick, low-cost AI tools to help detect early signs of heart dysfunction during regular primary care visits.
Demilade Adedinsewo, MD, MPH, et al
Department of Cardiovascular Diseases, Mayo Clinic, Jacksonville, FloridaVisual Abstract:
-
SUPPLEMENTAL MATERIALS IN PDF FILE BELOW
- Adedinsewo-Appendix_Tables_Figures.pdf -
PDF file
- Adedinsewo-Appendix_Tables_Figures.pdf -





{kind=link}
{kind=link}
{kind=link}
{kind=link}