
Article Figures & Data
Figures
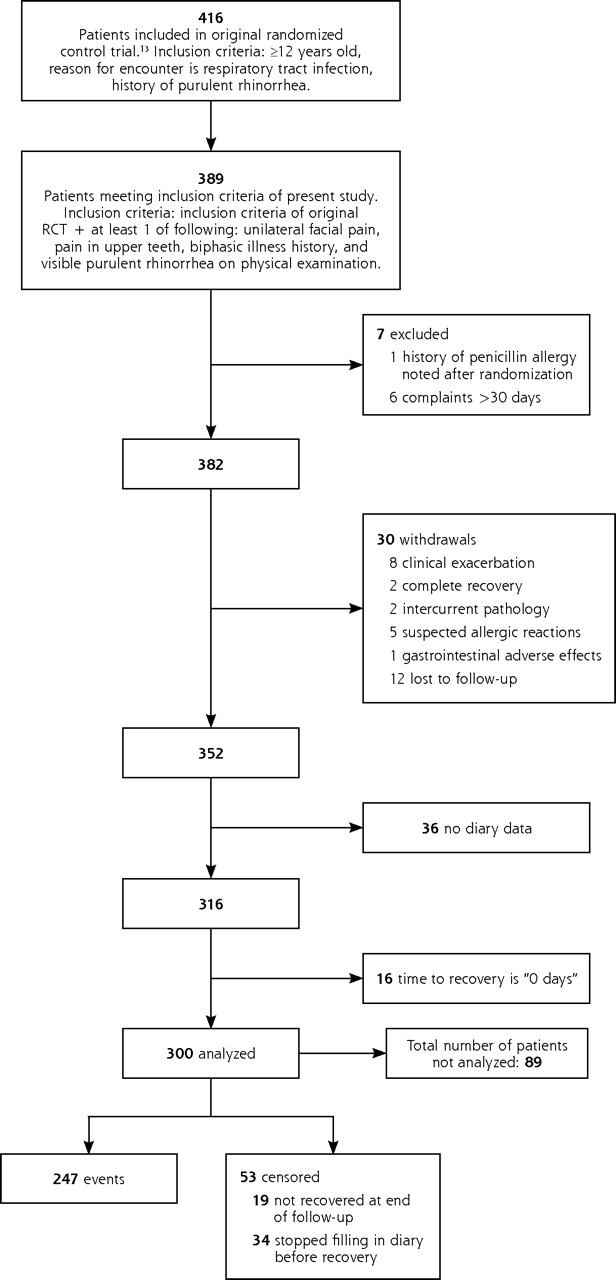
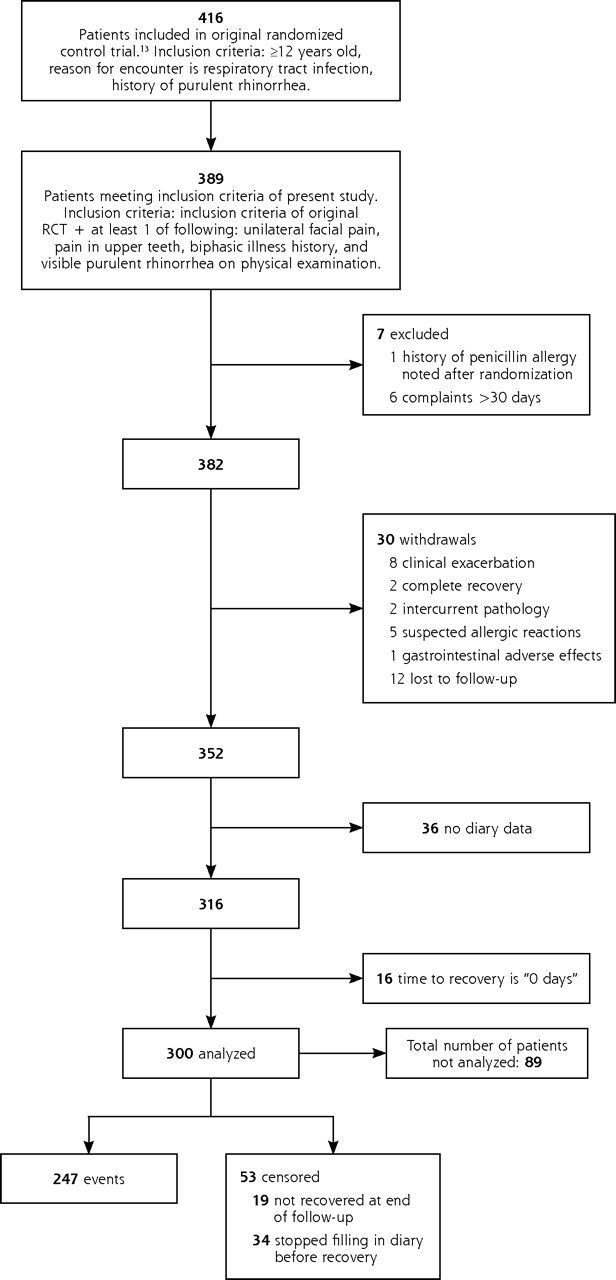
- Figure 1.
Flow chart of patients studied.
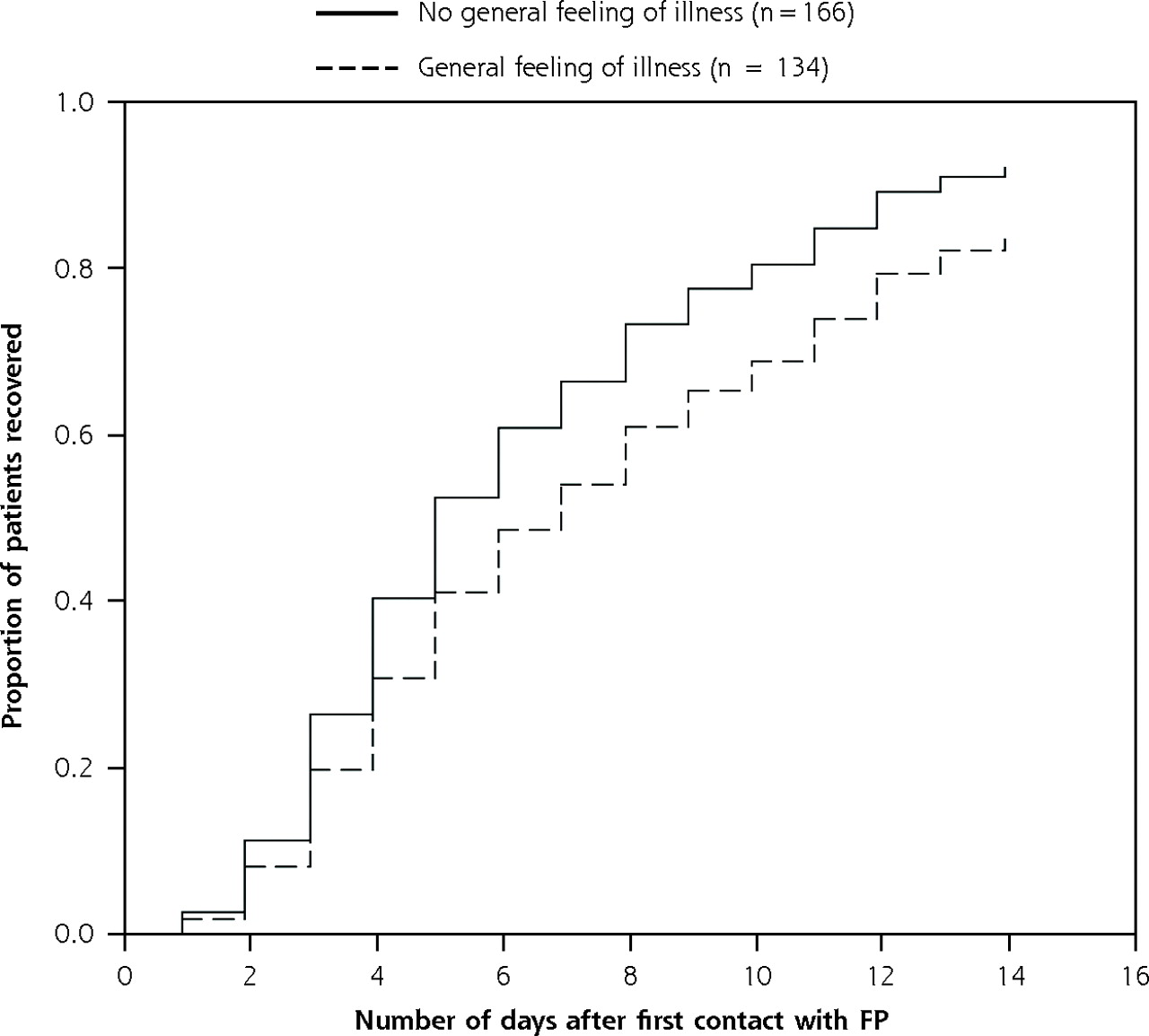
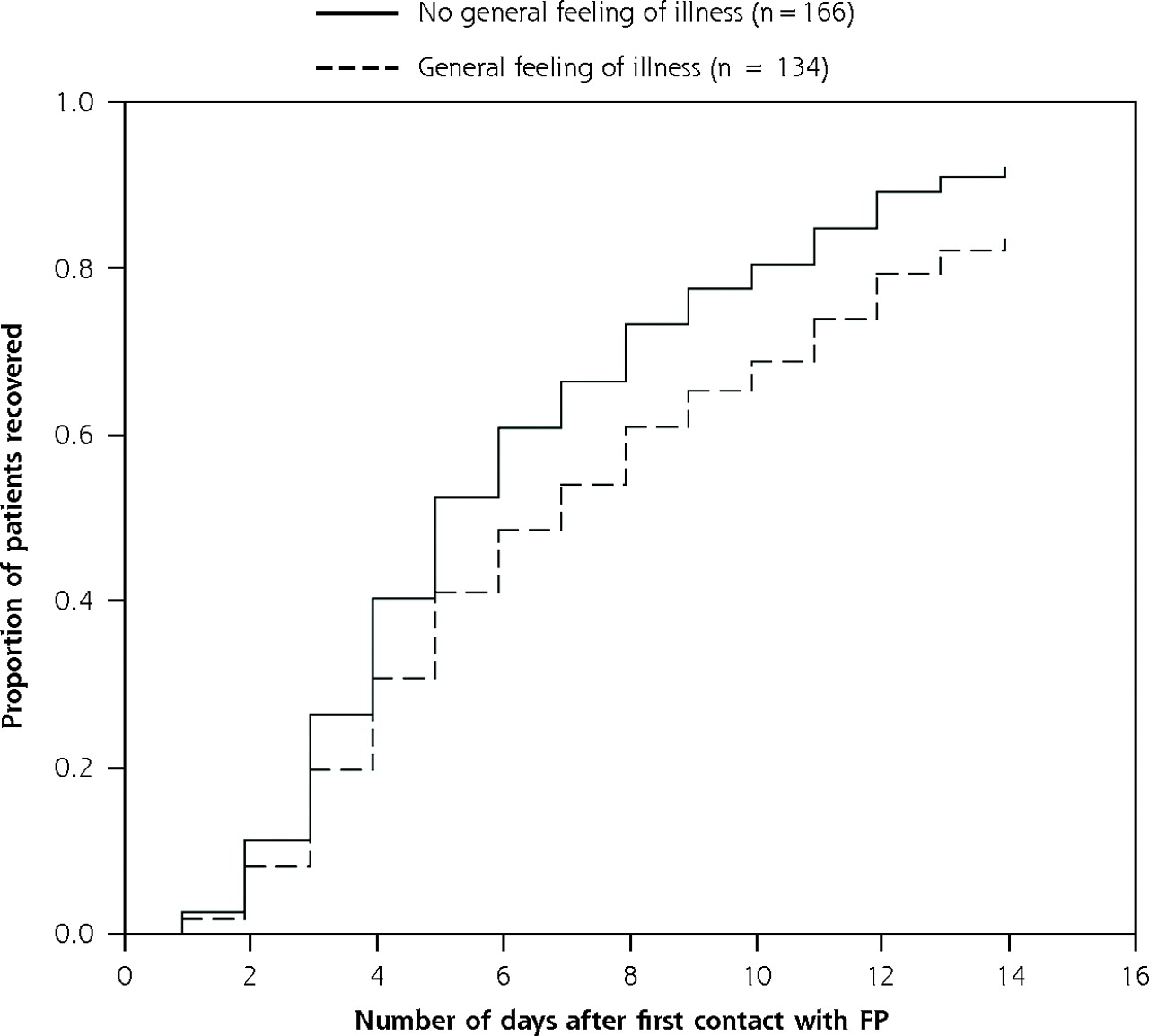
- Figure 2.
Recovery of patients according to their general feeling of illness at baseline adjusted for covariates.
FP = family physician.
Hazard ratio = 0.68 (95% confidence interval, 0.53–0.88); P = .003.
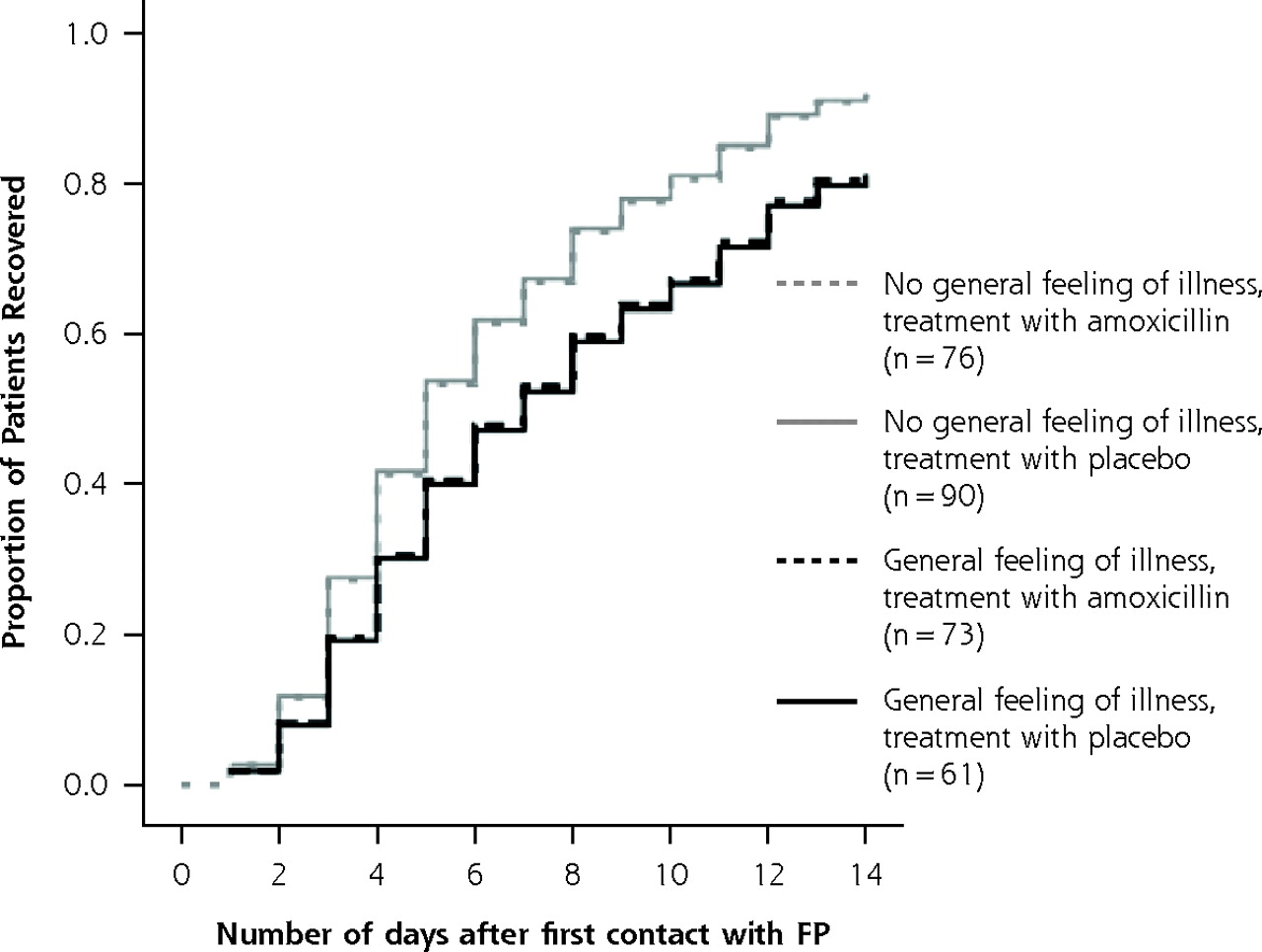
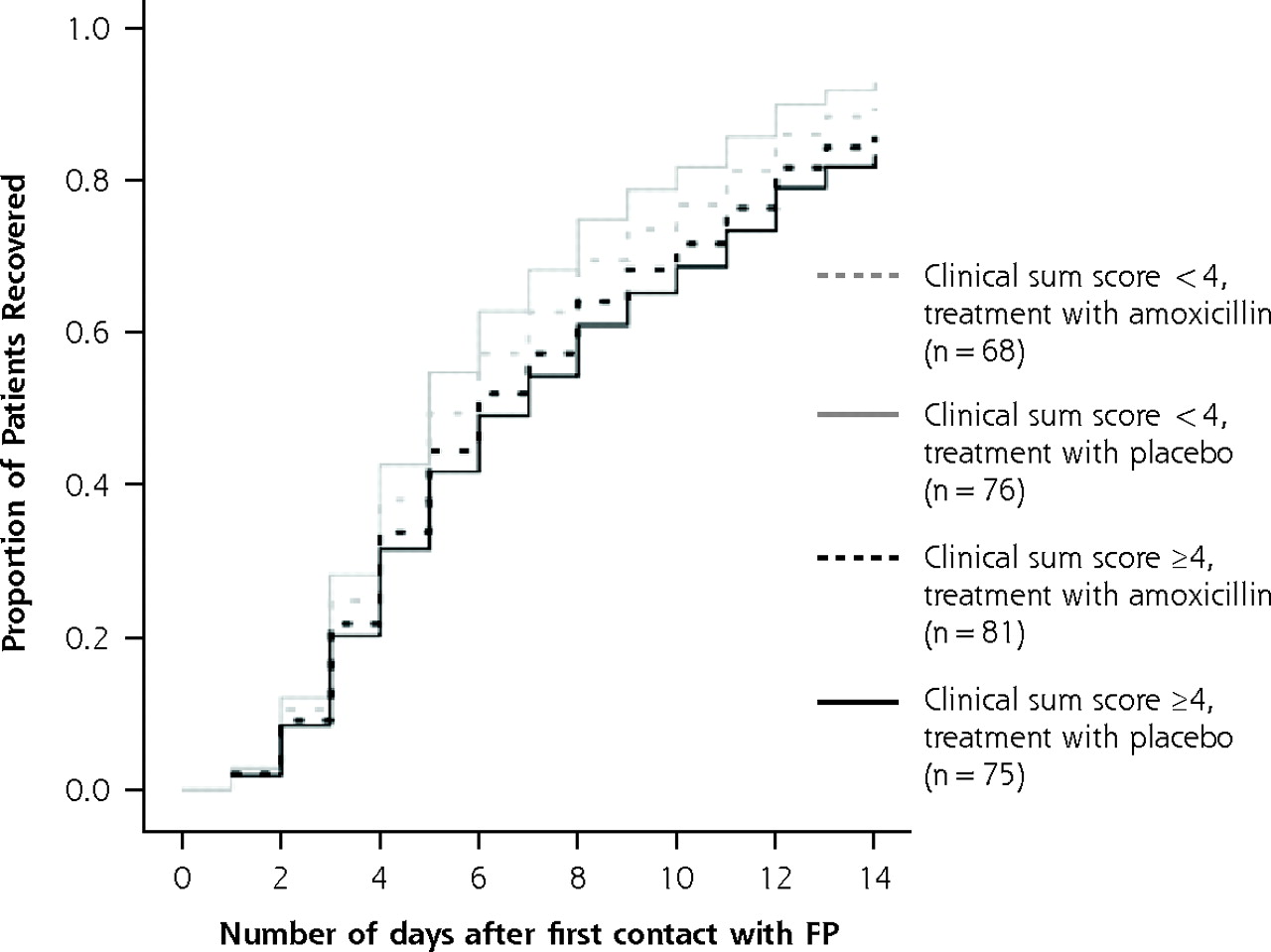
- Figure 3.
Illness course in patients according to treatment and clinical sum score.
FP = family physician.
Note: For the sum score, 1 point was given for each of the following: purulent rhinorrhea, postnasal drip, temperature ≤37.5°C, complaints present for ≤7 days, biphasic illness history, pain on bending, unilateral facial pain, and pain in upper teeth. Possible range of scores: 0 to 8 points.
* Cox regression analysis for interaction between clinical sum score and treatment group (see also Table 3⇑). Model: clinical sum score (<4 /≤4) + treatment group (amoxicillin/placebo) + clinical sum score × treatment group. P value for interaction = .36.
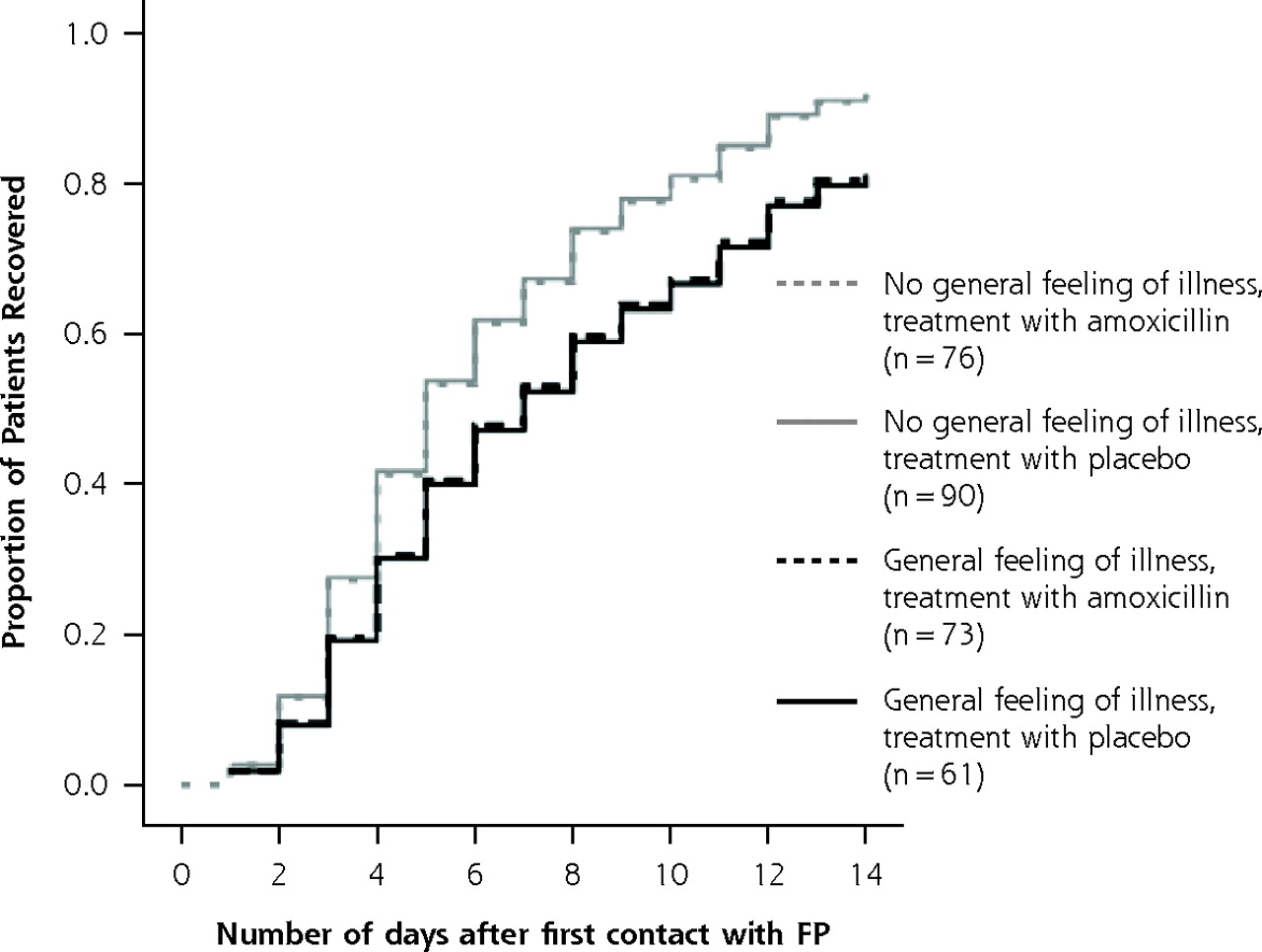
- Figure 4.
Illness course in patients according to treatment and general feeling of illness.
FP = family physician.
* Cox regression analysis for interaction between general feeling and treatment group (see also Table 3⇑). Model: general feeling of illness (present vs absent) + treatment group (amoxicillin vs placebo) + general feeling of illness × treatment group. P value for interaction = .91.

Tables
- Table 1.
Comparison of the Patients Meeting Inclusion Criteria Who Were and Were Not Analyzed in the Study
Patients Analyzed (n = 300) Patients Not Analyzed (n = 89) P Characteristic No. (%) n* No. (%) Value† * A total of 89 patients were not analyzed, but most of the n values in this column are less than 89 because of missing data. †χ2 test. ‡ Radiographic data were available for only 218 analyzed patients. Placebo treatment 151 (50.3) 89 47 (52.8) .68 Age older than mean (37 years) 129 (43.0) 63 31 (49.2) .27 Female sex 170 (56.7) 70 38 (54.3) .41 Purulent rhinorrhea 170 (56.7) 82 46 (56.1) .51 Postnasal drip 132 (44.0) 82 46 (56.1) .55 Temperature ≥37.5°C 46 (15.3) 82 15 (18.3) .31 Complaints ≥7 days 138 (46.0) 82 41 (50.0) .30 Biphasic illness 173 (57.7) 82 46 (56.1) .45 Pain when bending 193 (64.3) 82 55 (67.1) .37 Unilateral facial pain 175 (58.3) 82 44 (53.7) .26 Pain in upper teeth 54 (18.0) 82 14 (17.1) .50 Fatigue 186 (62.0) 82 41 (50.0) .03 Reduced productivity 155 (51.7) 82 36 (43.9) .13 General feeling of illness 134 (44.7) 82 16 (19.5) <.001 Abnormal radiograph 103 (47.2)‡ 51 23 (45.1) .45 Clinical sum score ≥4 156 (52.0) 82 39 (47.6) .28 Antibiotics in previous month 2 (0.6) 81 0 (0) 1.00 - Table 2.
Prognostic Variables and Patient Recovery: Results of Cox Proportional Hazard Regression Analyses (N = 300)
Bivariate Analysis Multivariate Analysis Prognostic Variable HR 95% CI P Value HR 95% CI P Value * HR = hazard ratio (ratio of the instantaneous recovery rate with and without the prognostic variable; HR <1 means slower recovery when that variable is present at first examination); CI = confidence interval. † Results of the stepwise (backward and forward) Cox multiple regression analysis. The variables included in the analysis were sex, unilateral facial pain, reduced productivity, and a general feeling of illness. ‡ n = 218. Placebo treatment 0.97 0.76–1.24 .80 – – Age older than mean (37 years) 0.86 0.66–1.11 .23 – – Female sex 1.20 0.93–1.54 .16 Not selected† Purulent rhinorrhea 1.09 0.84–1.40 .52 – – Postnasal drip 0.90 0.70–1.16 .42 – – Temperature ≥37.5°C 0.86 0.60–1.23 .40 – – Complaints ≥7 days 0.94 0.73–1.21 .65 – – Biphasic illness 0.92 0.71–1.18 .49 – – Pain on bending 0.97 0.75–1.27 .85 – – Unilateral facial pain 0.76 0.59–0.98 .03 Not selected† Pain in upper teeth 0.82 0.59–1.14 .24 – – Fatigue 0.83 0.64–1.07 .15 – – Reduced productivity 0.75 0.59–0.97 .03 0.77 0.60–0.99 .04† General feeling of illness 0.67 0.52–0.87 .002 0.68 0.53–0.88 .003† Abnormal radiograph‡ 1.02 0.76–1.37 .90 – – Clinical sum score ≥4 0.76 0.60–0.98 .04 Not selected† - Table 3.
Results of Cox Regression Analysis for Interactions Between Prognostic Variables and Treatment Group*
Interaction Term† Hazard Ratio 95% CI P Value CI = confidence interval. * The original trial13 had 2 treatment groups: antibiotics and placebo. A significant interaction would mean that the influence of the prognostic variable on the course of illness depends on whether the patient is treated with antibiotics or placebo. † Variables included in the multivariate model: prognostic variable + treatment group + prognostic variable × treatment group. ‡ Graphically illustrated in Figures 3 and 4. § n = 218. Age (>37 years) × treatment 1.04 0.62–1.73 .79 Sex × treatment 1.06 0.64–1.76 .69 Purulent rhinorrhea × treatment 1.11 0.67–1.84 .68 Postnasal drip × treatment 1.01 0.61–1.67 .98 Temperature ≥37.5°C × treatment 1.12 0.55–2.29 .75 Complaints ≥7 days × treatment 1.10 0.66–1.83 .71 Biphasic illness × treatment 1.00 0.60–1.67 .97 Pain on bending × treatment 1.10 0.65–1.85 .73 Unilateral facial pain × treatment 1.05 0.63–1.74 .85 Pain in upper teeth × treatment 1.31 0.68–2.52 .43 Fatigue × treatment 0.91 0.54–1.51 .71 Reduced productivity × treatment 1.22 0.74–2.01 .44 General feeling of illness × treatment‡ 0.97 0.58–1.61 .91 Abnormal radiograph§ × treatment 1.25 0.69–2.25 .47 Clinical sum score × treatment‡ 1.27 0.77–2.09 .36
The Article in Brief
Predicting Prognosis and Effect of Antibiotic Treatment in Rhinosinusitis
By An De Sutter, MD PhD, and colleagues
Background Rhinosinusitis (or sinusitis) is an infection or inflammation of membranes inside the nose and face. Although antibiotics are not generally effective in treating this condition, they are effective in treating a bacterial type of sinusitis that affects a minority of patients. The goal of this study is to search for clues to help identify sinusitis patients who might benefit from antibiotics.
What This Study Found Signs and symptoms of sinusitis and abnormal sinus x-ray findings do not help predict the course of the illness or whether the patient will benefit from antibiotics.
Implications
- This study contributes to a better understanding of the natural course of the "cold."
- There is no evidence that signs or symptoms of rhinosinusitis indicate a need for antibiotic treatment. Sinus x-rays have no added value in treating rhinosinusitis patients.
- The authors suggest that the best policy for patients who might have rhinosinusitis (and who do not have signs of complications or severe infection, such as high fever and serious pain) is to wait for natural recovery.
Annals Journal Club Selection:
Nov/Dec 2006
The Annals Journal Club is designed to encourage a learning community of those seeking to improve health care and health through enhanced primary care. Additional information is available on the Journal Club home page.
The Annals of Family Medicine encourages readers to develop the learning community of those seeking to improve health care and health through enhanced primary care. You can participate by conducting a RADICAL journal club, and sharing the results of your discussions in the Annals online discussion for the featured articles. RADICAL is an acronym for: Read, Ask, Discuss, Inquire, Collaborate, Act, and Learn. The word radical also indicates the need to engage diverse participants in thinking critically about important issues affecting primary care, and then acting on those discussions.1Articles for Discussion
- van Driel M, De Sutter A, Deveugele M, et al. Are sore throat patients who hope for antibiotics actually asking for pain relief? Ann Fam Med. 2006;4:494-499.
- De Sutter A, Lemiengre MB, Van Maele G, et al. Predicting prognosis and effect of antibiotic treatment in rhinosinusitis. Ann Fam Med. 2006;4:486-493.
- Hickner J. A new look at an old problem: inappropriate antibiotics for acute respiratory infections. Ann Fam Med. 2006;4:484-485.
Discussion Tips
These articles use different methods to address different aspects of the problem of antibiotic overuse for respiratory illness.2 van Driel et al solicit the patient�s perspective on the reason for consulting for acute sore throat. De Sutter et al use clinical data to try to predict illness duration and response to antibiotics in patients with rhinosinusitis. You may wish to discuss only one study, or to consider each separately and then try to draw larger insights across both articles.Discussion Questions
- What is the research question in these studies? Why do the questions matter?
- Are the study designs appropriate for the research questions? How could the designs be improved?
- Study methods�to what degree can the findings be accounted for by:
- How participants were selected?
- How key variables were defined and measured?
- Confounding (false attribution of causality because 2 variables discovered to be associated actually are associated with a third factor)?
- How information was interpreted?
- Chance (as indicated by inferential statistics)?
- Main findings�how do these studies advance current knowledge?
- Generalizability�how transportable are the findings to other settings, particularly to my patients, practice and community? For the DeSutter et al study, how does the nesting of this observational study within an RCT affect its external validity?
- Implications�how can these findings be used to change practice or advance new hypotheses and research? Do you think that searching (in patient care and in research) for subgroups of patients who might benefit from antibiotics is justified? How can patient needs/desires be met without antibiotics?
References
- Stange KC, Miller WL, McLellan LA, et al. Annals journal club: It�s time to get RADICAL. Ann Fam Med. 2006;4:196-197. Available at: http://annfammed.org/cgi/content/full/4/3/196.
- Centers for Disease Control. Antibiotic/Antimicrobial Resistance Clinical Guidelines. March 30, 2006. Available at: http://www.cdc.gov/drugresistance/clinical.htm.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The role of antibiotics in the treatment of acute rhinosinusitis in children: a systematic review
- Acute sinusitis
- Point-of-Care C-Reactive Protein Testing and Antibiotic Prescribing for Respiratory Tract Infections: A Randomized Controlled Trial
- On TRACK: The Search for the Holy Grail
- A New Look at an Old Problem: Inappropriate Antibiotics for Acute Respiratory Infections
- In This Issue: Prescribing Drugs: What Do Patients and Pharmaceutical Companies Really Want?
- Annals Journal Club: Antibiotics for Common Respiratory Infections