
Abstract
PURPOSE To determine if hospitalized patients with depressive symptoms will benefit from post-discharge depression treatment with care transition support.
METHODS This is a randomized controlled trial of hospitalized patients with patient health questionnaire-9 score of 10 or more. We delivered the Re-Engineered Discharge (RED) and randomized participants to groups receiving RED-only or RED for Depression (RED-D), a 12-week post-discharge telehealth intervention including cognitive behavioral therapy, self-management support, and patient navigation. Primary outcomes were hospital readmission and reutilization rates at 30 and 90 days post discharge.
RESULTS We randomized 709 participants (353 RED-D, 356 RED-only). At 90 days, 265 (75%) intervention participants had received at least 1 RED-D session (median 4). At 30 days, the intention-to-treat analysis showed no differences between RED-D vs RED-only in hospital readmission (9% vs 10%, incidence rate ratio [IRR] 0.92 [95% CI, 0.56-1.52]) or reutilization (27% vs 24%, IRR 1.14 [95% CI, 0.85-1.54]). The intention-to-treat analysis also showed no differences at 90 days in readmission (28% vs 21%, IRR 1.30 [95% CI, 0.95-1.78]) or reutilization (70% vs 57%, IRR 1.22 [95% CI, 1.01-1.49]). In the as-treated analysis, each additional RED-D session was associated with a decrease in 30- and 90-day readmissions. At 30 days, among 104 participants receiving 3 or more sessions, there were fewer readmissions (3% vs 10%, IRR 0.30 [95% CI, 0.07-0.84]) compared with the control group. At 90 days, among 109 participants receiving 6 or more sessions, there were fewer readmissions (11% vs 21%, IRR 0.52 [95% CI, 0.27-0.92]). Intention-to-treat analysis showed no differences between study groups on secondary outcomes.
CONCLUSIONS Care transition support and post-discharge depression treatment can reduce unplanned hospital use with sufficient uptake of the RED-D intervention.
INTRODUCTION
Depression is an important risk factor for poor outcomes among patients with acute and chronic conditions.1-5 Among patients hospitalized for acute conditions, comorbid depressive symptoms jeopardize a safe transition from hospital to home. Among patients with chronic illness, depression is linked to increased symptom burden, functional decline, and reduced quality of life. Patients with comorbid depressive symptoms often lack essential coping skills to manage their symptoms and are at risk for medication misuse and missing post-discharge appointments.6-8 Treating comorbid depression can improve physical and psychosocial function,9 and additional care transition support is needed to avoid unplanned readmission and emergency department use.
Our team developed and studied the Re-Engineered Discharge (RED), a nationally disseminated readmission reduction program. Our research showed that a systematic approach to hospital discharge can reduce 30-day readmissions and emergency department visits.10,11 Despite the use of RED, however, 30-day readmissions and emergency department visits were 1.5 to 2.0 times higher among RED study participants with comorbid depressive symptoms.12 Other research also showed that increased risk for hospitalization persists among patients with comorbid depressive symptoms for as much as 4 years following an index hospitalization.13
To address the increased risk of readmission for hospital patients with depressive symptoms, we studied whether an adapted version of the RED protocol (RED for Depression [RED-D]) with post-discharge and mental health support reduces unplanned hospital encounters in patients with depressive symptoms compared with use of the RED protocol alone.14
METHODS
Overview
In this randomized control trial, we compared the effectiveness of RED and RED-D to reduce readmission rates and emergency department visits among patients with moderate to severe depressive symptoms. The intervention group received the RED-D protocol that included a 12-week post-discharge telehealth intervention, including brief cognitive behavioral therapy, patient navigation, and self-management education. The control group received the RED protocol alone.
The study was conducted according to the Consolidated Standards of Reporting Trials (CONSORT) and the published protocol.14,15 The Boston University Medical Campus Institutional Review Board approved study activities. Participants provided written informed consent and an external data monitoring committee reviewed unblinded safety data.
Settings
This study was initially conducted at Boston Medical Center in Boston, Massachusetts. After trial commencement, because of low accrual, a protocol amendment added Mount Auburn Hospital in Cambridge, Massachusetts as second recruitment site. Enrollment occurred from February 6, 2013 through October 25, 2016.
Consent and Eligibility
During recruitment, study staff reviewed a daily list of hospitalized patients admitted within 24 hours and assessed eligibility using medical records. Patients admitted for altered mental status, end-of-life care, sickle cell crisis, or substance use were excluded immediately. A random-number sequence determined the order to approach potentially eligible patients. Inclusion criteria were individuals aged 18 years and older that were able to provide informed consent in English, and had a telephone, a primary care clinician (PCC), and planned to stay in the local area for the study period. From this group, patients that had suicide precautions in place, were incarcerated, were pregnant, undergoing cancer treatment, had been admitted to a surgical trauma unit, or were to be discharged to other institutional settings were excluded.
Post-Consent Final Eligibility
Final eligibility was determined after consent due to the sensitivity of the information collected. The 9-item Patient Health Questionnaire (PHQ-9) was used to screen for depressive symptoms.16 Participants with PHQ-9 scores of 10 or greater were eligible. We excluded participants reporting a suicide attempt in the last 6 months or current suicidal ideation. Study staff then used the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, 4th edition Axis I Disorders17 to exclude patients with symptoms of psychosis and bipolar disorder, the 4-item Screening for Alcohol Use18 questionnaire to exclude those with problem alcohol use (scores >2), and the 10-item Drug Abuse Screening Test19 to exclude those with problem drug use (scores >5).
Baseline Data Collection
Baseline sociodemographic data, Rapid Estimate of Adult Literacy in Medicine,20 Quality of Life Enjoyment and Satisfaction Questionnaire-Short Form (Q-LES-Q-SF),21 Patient Activation Measure (PAM-13),22 and Generalized Anxiety Disorder (GAD-7)23 were collected. A licensed mental health specialist evaluated participants and determined if criteria for major depression were met at enrollment.
Randomization
Block randomization (block size = 8) randomly assigned participants (50:50) to either RED-only or RED-D groups.24 Randomization assignments were placed in sequentially numbered envelopes that were unsealed after baseline data collection.
Control Condition
A discharge educator delivered the 12-component RED protocol to all study participants. The RED protocol includes a post-discharge telephone call to support medication adherence, confirm the PCC follow-up appointment, and provide education on symptoms and care plan management. Additional details of the RED protocol are described elsewhere.11
Intervention
In addition to the RED protocol, the intervention group participants received the RED-D protocol for up to 12 weeks post discharge. This consisted of telephone sessions facilitated by a licensed Master’s-level counselor and supervised by a study psychiatrist. Session structure was tailored to participants’ needs and symptom burden, as determined by the counselor.
The components of the RED-D protocol were brief cognitive behavioral therapy, self-management education, and patient navigation. Brief cognitive behavioral therapy25 included orientation to the thought-feeling connection, transforming negative thoughts, and physical symptoms and stress management. Self-management education focused on diet, exercise, medication management, and coping with symptoms. Patient navigation included support for scheduling appointments, coordinating transportation, and adhering to the discharge plan; and sharing information back to primary care clinicians.14
Using elements of the Collaborative Care Model,26 the counselor discussed all cases with the study psychiatrist and communicated depression symptom ratings to the participant’s primary care or psychiatric clinician weekly. We used an evidence-based algorithm to determine recommendations to share with PCCs for depressive symptom management.27
Outcomes
Primary outcomes were 30- and 90-day rate of hospital readmission and reutilization (hospital readmissions, emergency department visits, and observations) after index discharge and were collected from electronic health records.
Blinded research assistants collected Q-LES-Q-SF, PHQ-9, PAM-13, and GAD-7 scores at 30 and 90 days after discharge as secondary outcomes.
Sample Size
Based on prior research,10 we expected 32% of participants to be readmitted or seen at an emergency department within 30 days, and that RED-D would reduce reutilization to 22%, requiring a sample size of 678 to attain 80% power at a significance level of 0.025. Assuming 2% missing observations, we required 692 patients for randomization.
Statistical Analysis
Intention-to-treat analyses of primary outcomes included all randomized participants and computed incidence rate ratios (IRR) and 95% CIs from Poisson models that regressed 30- and 90-day outcome counts on each study arm.
As-treated analyses for 30- and 90-day primary outcomes were performed by regressing outcome counts on the number of sessions completed by that time point, using Poisson models.
We checked for confounding due to self-selection into number of sessions by regressing the number of sessions on baseline PHQ-9, GAD-7, and PAM-13 score, major depressive disorder, education, income, sex, recruitment site, and age. Characteristics associated with number of sessions were controlled for in the as-treated regressions.
Secondary outcomes were assessed with an intention-to-treat analysis using independent t-tests and χ2 tests, as appropriate, and with an as-treated analysis by regressing 30- and 90-day PHQ-9, GAD-7, PAM-13, and Q-LES-Q-SF scores on the number of intervention sessions received, using ordinary least squares and controlling for characteristics associated with number of sessions.
Dose-response effects of the self-management, patient navigation, and brief cognitive behavioral therapy components of RED-D were assessed using Poisson models that regressed readmission rate on the time spent receiving each component by 30 and 90 days.
To check sensitivity to missingness, all analyses of primary outcomes were replicated using data imputed by chained equations and predictive mean matching, with results pooled from 50 imputations (Supplemental Table 1).
All statistical tests were run at alpha level 0.05, and parametric tests were checked at 0.025 after applying a Bonferroni correction for multiple testing. R programming language, version 3.4.3 (the R Foundation) was used for all analyses.28
RESULTS
Study Sample
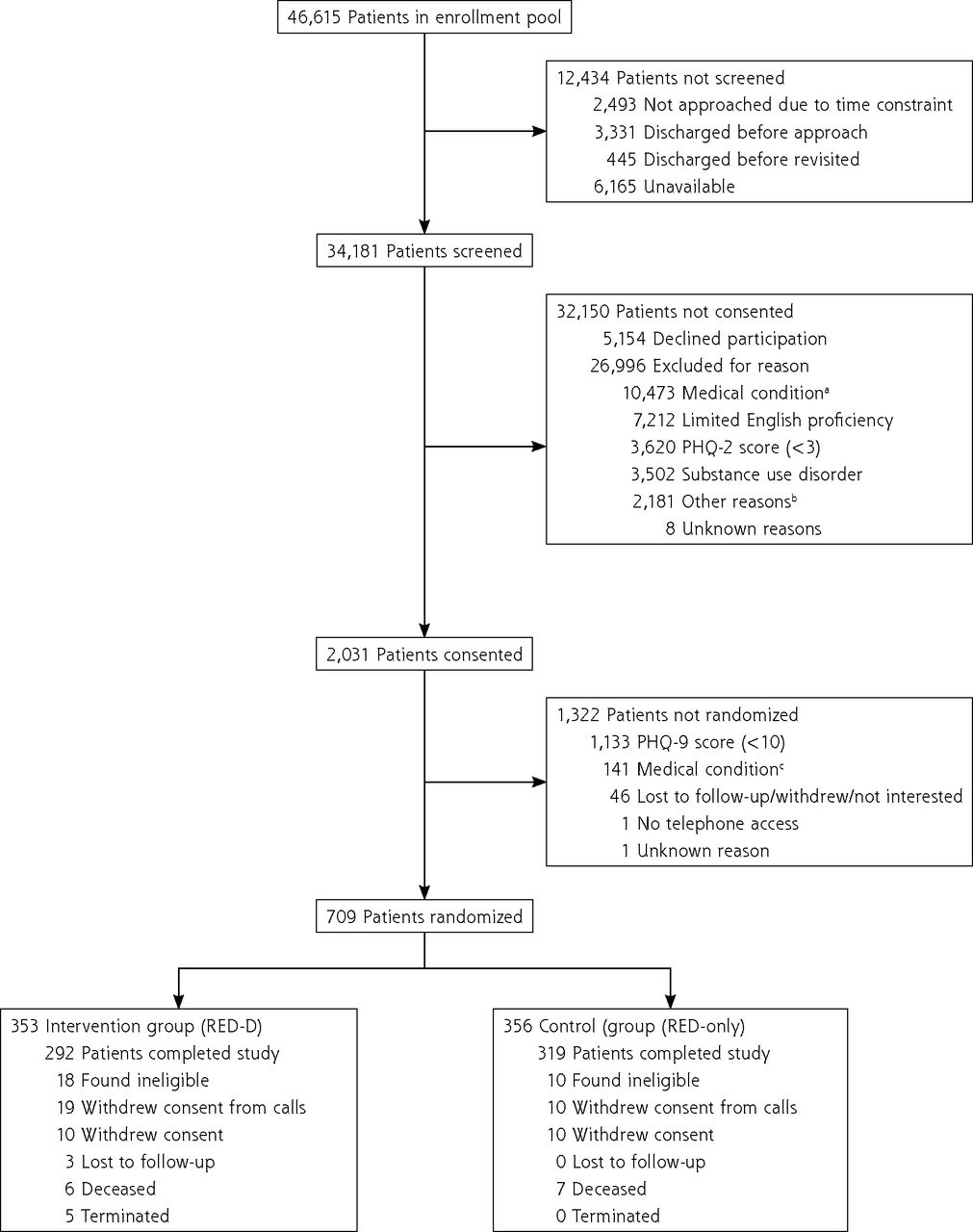
A total of 34,181 hospitalized patients were screened. Of these, 26,996 (79%) were ineligible, 5,154 (14%) declined participation, and 2,031 (6%) consented to participation. After determining final eligibility, 709 participants were randomized (353 RED-D, 356 RED-only) (Figure 1).
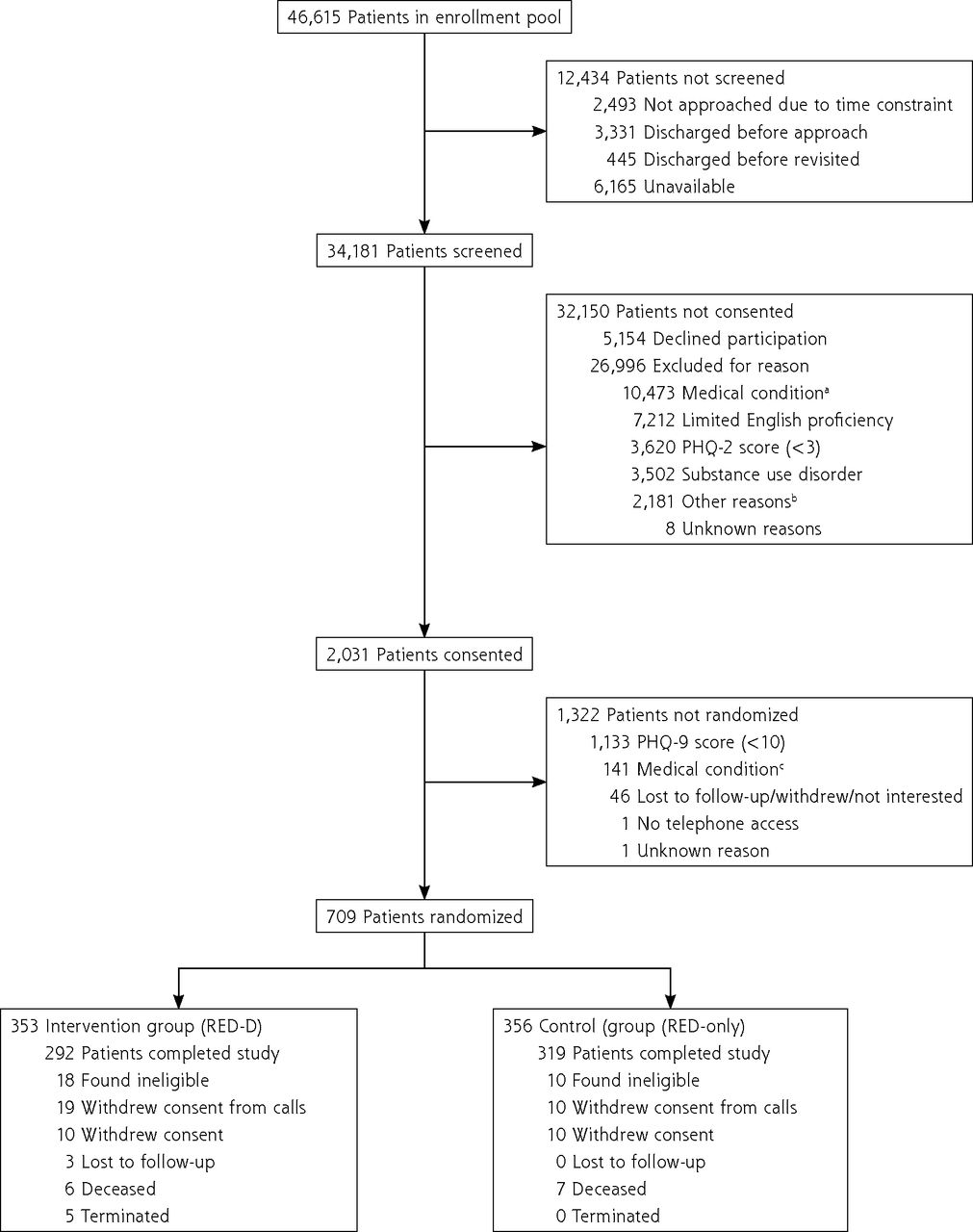
Study flowchart.
CAGE = 4-item screening for alcohol use: cutting down, annoyance by criticism, guilty feeling, and eye-openers; DAST = 10-item drug abuse screening test; PHQ-9 = patient health questionnaire-9; PHQ-2 = patient health questionnaire-2; RED = re-engineered discharge; RED-D = re-engineered discharge for depression.
a Medical exclusion occurred in phases. Patients admitted for altered mental status, end-of-life care, sickle cell crisis, or substance use were excluded from the pool immediately. Then, potentially eligible patients were excluded if they were going to be discharged to another inpatient facility, pregnant, under suicide precautions, undergoing cancer treatment; admitted to a surgical trauma unit.
b Other reasons for exclusion included: incarceration; no access to telephone; no primary care clinician; not staying in the area during the study; aged <18 years; enrolled in another discharge planning program.
c Medical exclusions after consent were for having a serious mental illness diagnosis, self-reported suicidal ideation, and self-reported alcohol or drug abuse (CAGE score >2, DAST score >5).
The mean ages of RED-D and RED-only groups, respectively, were 50.3 and 50.9 years, 60% and 62% were women, 45% and 41% were non-Hispanic Black people, and 51% and 49% were disabled or unemployed persons. The mean baseline PHQ-9 score was 15 in both groups, indicating moderately severe depressive symptoms. A total of 27% and 31% met clinical criteria for major depressive disorder (Table 1).
Demographic and Clinical Characteristics at Enrollmenta
Delivery of RED-D Protocol
By 30 days after hospital discharge, 264 (75%) patients in the RED-D group had participated in 1 or more counseling session (median = 2, interquartile range [IQR] 2). One more patient had participated by 90 days (265 [75%], median = 4, IQR 6). By 30 days, 104 (30%) participants had attended 3 or more sessions; by 90 days, 87 (25%) had attended 6 or more sessions. Mean session duration was 62.4 minutes (SD 59.8).
At 90 days, 130 participants received on average 25 minutes of self-management education (SD 27), 121 participants averaged 12 minutes of patient navigation (SD 10), and 126 participated in brief cognitive behavioral therapy sessions.
Primary Outcomes
Intention-to-treat analysis (RED-only vs RED-D) did not show reductions in readmissions at 30 days (10% vs 9%, P = .758, IRR 0.92 [95% CI, 0.56-1.52]) or 90 days (21% vs 28%, P = .106, IRR 1.30 [95% CI, 0.95-1.78]). There were similar findings for hospital reutilization at 30 days (24% vs 27%, P = .386, IRR 1.14 [95% CI, 0.85-1.54]) and 90 days (57% vs 70%, P = .041, IRR 1.22 [95% CI, 1.01-1.49]) (Table 2).
Primary Outcomes: Intention-to-Treat and As-Treated Analysis at 30 and 90 Days
At 30 days, among the 104 intervention patients who received 3 or more sessions, there were fewer readmissions compared with controls (0% vs 10%, IRR 0.30 [95% CI, 0.07-0.84], P = .012). By 90 days, among the 109 patients who received 6 or more sessions, there were fewer readmissions compared with controls (11% vs 21%, IRR 0.52 [95% CI, 0.27-0.92], P = .030). There were similar results for reutilizations (Table 2).
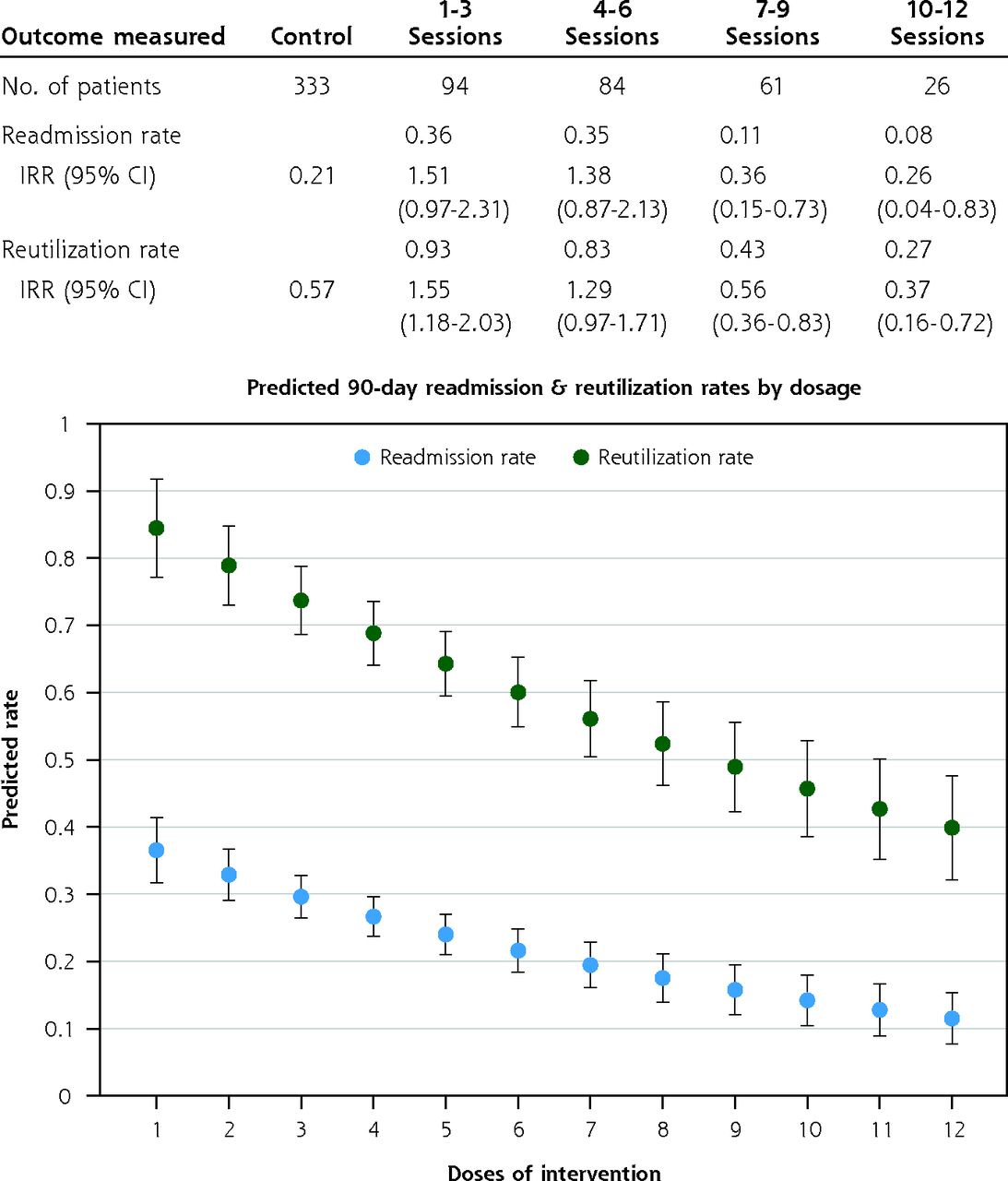
At 30 days, each additional counseling session was associated with a 23% decrease in the per-participant rate of readmissions (P = .077), and an 8% decrease in the rate of reutilizations (P = .276). At 90 days, each additional session was associated with a 10% decrease in the rate of readmissions (P = .003), and a 7% decrease in the rate of reutilizations (P = .002). At 90 days, there was a progressively decreasing readmission rate per session from 27% with 1 session to 8% with 10 sessions. Similarly, reutilization decreased from 72% with 1 session to 27% with 10 sessions (Figure 2).
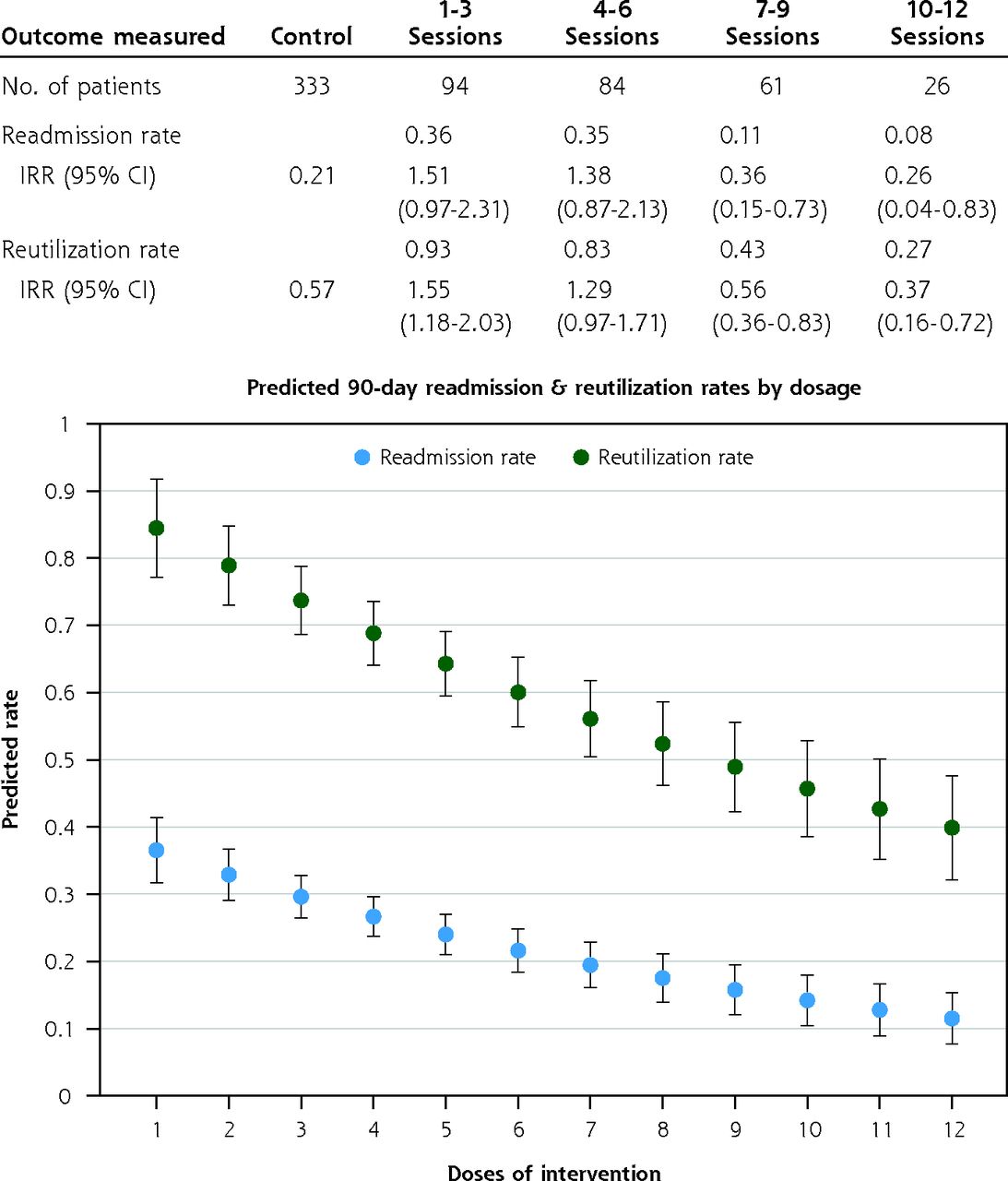
Readmission and reutilization rates for intervention patients by the number of counselling sessions completed at 90 days.
IRR = incidence rate ratio.
Note: Labeled points indicate predicted values from Poisson regression of 90-day readmission and reutilization rates on cumulative dosage of the intervention. Each value represents the readmission or reutilization rate we would expect at that associated dosage, based on regression models.
At 30 and 90 days, the number of RED-D sessions received was not correlated with baseline measurements of PHQ-9, depression diagnosis, GAD-7 score, PAM-13, education, income, and recruitment site (Supplemental Table 2). Differences were detected between participants that received fewer than 3 vs 3 or more sessions at 30 days in age (mean age 49 years vs 53 years, P = .006) and sex (62% vs 73% female, P = .047), and between participants that received fewer than 6 vs 6 or more sessions at 90 days in age (mean age 48 years vs 54 years, P <.001) (Supplemental Table 2). Results were not sensitive to controlling for these variables.
Secondary Outcomes
Intention-to-treat analysis showed no differences in 30-day PHQ-9 (10.0 vs 10.6), GAD-7 (8.7 vs 8.6), PAM-13 (37.6 vs 36.3), Q-LES-Q-SF (52.4 vs 51.9), having a PCC (97% vs 96%), seeing a PCC within 30 days (61% vs 64%), discussing depression with a PCC (44% vs 52%), or seeing other doctors (58% vs 53%) (Supplemental Table 3). There were similar findings at 90 days.
In the as-treated analyses, each additional session was associated with a PHQ-9 score that was, on average, 1 point lower at 30 days (than if that session had not occurred; 95% CI, −1.8 to 0.3; P = .009) and 0.3 points lower at 90 days (95% CI, −0.6 to 0.1; P = .111), and with a GAD-7 score that was 0.6 points lower at 30-days (95% CI, −1.5 to 0.2; P = .146), and 0.1 point lower at 90 days (95% CI, −0.5 to 0.3; P = .737). Each additional session was also associated with participants having a Q-LES-Q-SF score that was 2.1 points higher at 30 days (95% CI, −0.2 to 4.4; P = .070) and 0.9 points higher at 90 days (95% CI, −0.1 to 2.0; P = .087), and with no difference in PAM-13 score at 30 days (95% CI, −0.7 to 0.7; P = .995), but a PAM-13 score that was 0.3 points higher at 90 days (95% CI, 0.0-0.1; P = .051) (Supplemental Figure 1 and Supplemental Figure 2).
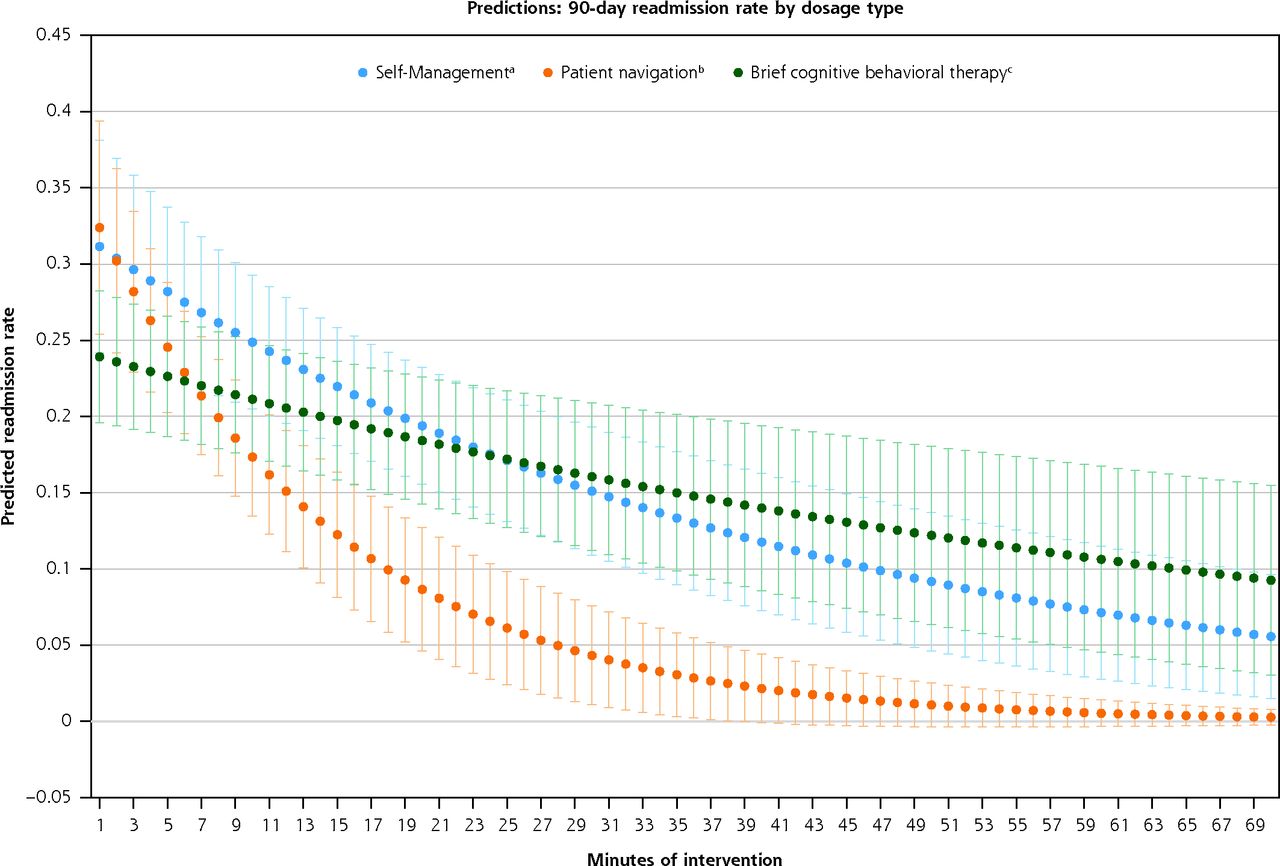
Figure 3 shows the predicted readmission rate at 90 days by the number of minutes per RED-D component. There was a decrease in readmission rates associated with time spent receiving each component. Patient navigation was associated with the largest and most rapid decline in readmissions.
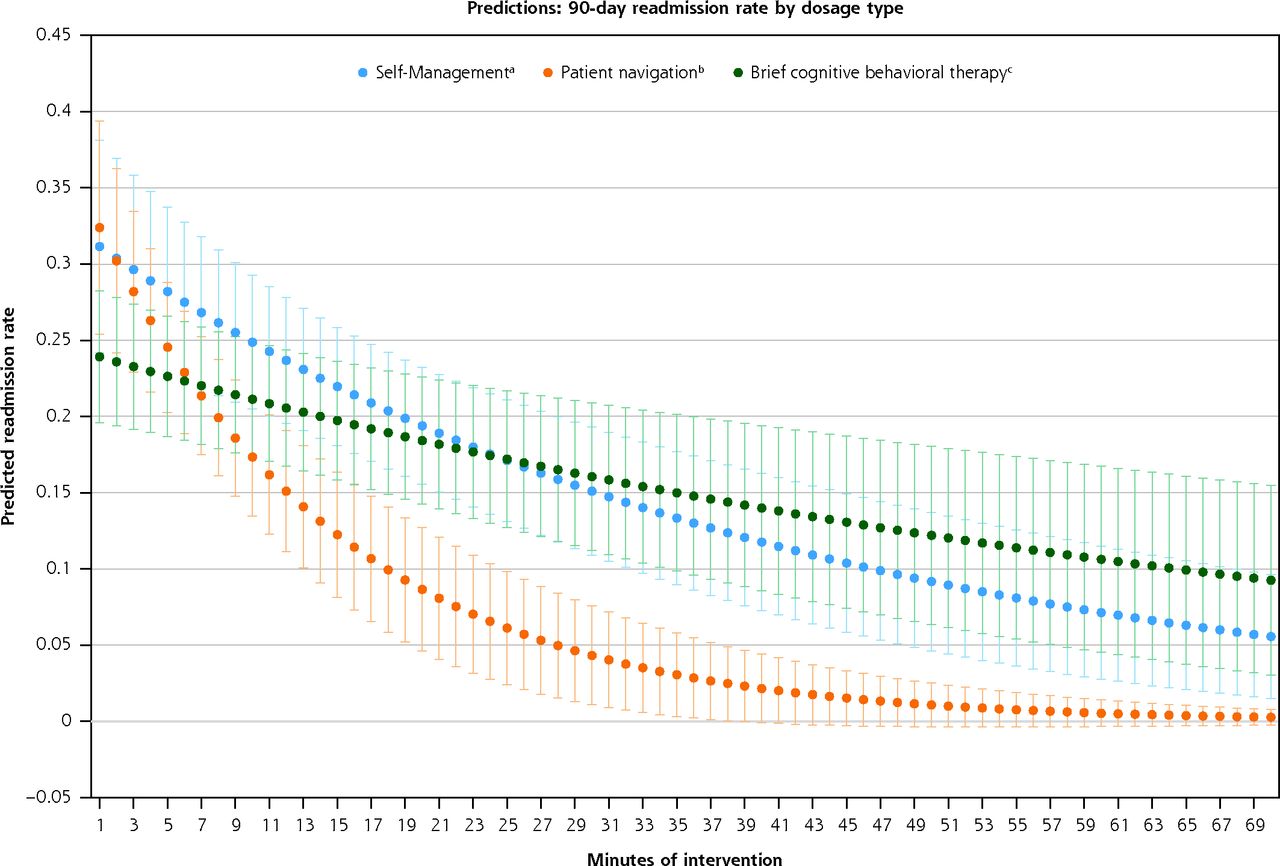
Predicted readmission rate at 90 days by type of post-discharge support for intervention participants receiving 6 or more sessions.
Note: Predicted values were generated using Poisson regression.
a Self-management was counselling focused on chronic disease self-management, including diet/nutrition, exercise, managing medications, talking to your doctor, and coping with exacerbations.
b Patient navigation includes guidance in navigating difficult aspects of the health care system, such as overcoming financial barriers, scheduling appointments, and coordinating transportation services, as well as adherence to the discharge plan and follow-up care.
c Brief cognitive behavior therapy includes orientation to the thought-feeling connection, transforming negative thoughts, behavior activation, physical symptoms, and stress management and navigating relationships, and homework.25
Adverse Events
Adverse events were reviewed by study clinicians, the Boston University Medical Campus Institutional Review Board, and the Data and Safety Monitoring Board. Adverse events (n = 26) recorded included 13 reports of suicidal ideation, 2 hospitalizations due to suicide attempt or ideation, and 11 all-cause deaths during study participation. Adverse events were not significantly different between groups and determined to be expected and unlikely related to the intervention.
DISCUSSION
This study adds to the literature showing the importance of post-discharge counseling and care transition support to reduce hospital readmissions among those with chronic illness and a high burden of cognitive and somatic symptoms of depression. An intention-to-treat analysis detected no difference in all-cause hospital readmission or reutilization at 30 or 90 days after index hospital discharge among hospitalized patients with depressive symptoms (PHQ-9 score ≥10) offered the RED-D intervention compared with RED alone. In the as-treated analysis, however, readmissions decreased 70% at 30 days and 48% at 90 days—showing that, with sufficient uptake, the intervention reduced re-hospitalizations. Furthermore, the RED-D intervention can be delivered by primary care teams after discharge to reduce readmissions among patients with depressive symptoms.29-32
Research has linked higher PHQ-9 scores in hospitalized patients with increased functional impairment, number of disability days, health care use, mortality rate, and hospital readmission.33-35 The high burden of physical symptoms during hospitalization could exacerbate depressive symptoms in chronically ill patients. Our prior work showed that hospitalized individuals with PHQ-9 scores of 10 or more have nearly 2 times the rate of readmissions compared with those who score in the non-depressive range (PHQ-9 score <5). Yet, while all RED-D participants had PHQ-9 scores of 10 or more, only one-third had confirmed depression based on clinical psychiatric interview.12,36 Interestingly, those with confirmed clinical depression were not more likely to engage with the intervention, or to benefit from it, compared with those who did not have confirmed depression. This suggests that depressive symptoms measured by the PHQ-9 identify patients with a high symptom burden and increased risk for readmission who could benefit from post-discharge support and counseling, as delivered by RED-D.
This study identifies the relative contributions of the brief cognitive behavioral therapy, self-management, and patient navigation components of RED-D. Each component contributes to the decrease in readmission rates with patient navigation being most effective in the first 30 days. These data support that early post-discharge navigational assistance, including support with appointment tracking and adherence to new medication, can benefit patients during a time where transition of care challenges emerge.10 Later, counseling focused on chronic disease self-management may become important.
Several features of the trial design should be considered. First, the 2-step application of eligibility criteria excluded participants with a high likelihood of substance abuse. This resulted in a group of participants with depressive symptoms but without alcohol and substance use co-morbidities, a group that is likely to respond differently to a post-discharge counseling intervention, allowing the results to be better generalized to patients with depressive symptoms. Second, both study groups had the evidence-based re-engineered discharge program initiated before discharge. RED was shown to reduce readmissions and emergency department use in the 30 days after discharge.10 Our data show that, while assigning RED-D by itself does not out-perform RED, fully administering the RED-D intervention for at least 3 sessions would reduce 30-day readmissions by 1 more than if those participants had received RED alone. This finding provides an example of tailoring transition of care interventions based on clinical characteristics, an approach with great potential.
This study also has several limitations. Because we observed an effect of the RED-D intervention in the as-treated analysis but not the intention-to-treat analysis, we strongly suspect that low study adherence was responsible for the null findings. Given that the uptake of counseling services is low among patients in community settings,37 it is not surprising that acceptance of a 12-week counseling intervention was low among recently discharged patients, particularly when the reason for recommending counseling services was unrelated to the admission primary diagnosis. For this reason, the as-treated findings are likely to be more predictive of implementation in clinical practice, even while this study design cannot rule out confounding from unobserved covariates.38
Other factors limiting gerneralizability include high levels of unemployment and disability, low educational attainment, and lower incomes of our study population. Also, primary outcome data were collected from electronic health records and therefore missed reutilization at other hospitals, estimated to be 10% from prior studies.10 However, a preferential impact on study groups is unlikely. Sensitivity analyses controlling for hospital site did not impact our results (Supplemental Table 4).
CONCLUSION
Assignment to the RED-D intervention by itself does not produce a detectable effect. Sufficient uptake of RED-D by hospitalized patients with depressive symptoms, however, has an important positive impact on readmission rates.
Acknowledgments
Dr Bruce Rollman and Ekaterina Sadikova
Footnotes
Conflicts of interest: authors report none.
Funding support: Supported by the Agency for Health Research and Quality (RO1HS019700) and the Blue Cross Blue Shield Foundation of Massachusetts (MHCA-2269).
Trial registration: ClinicalTrials.gov NCT01840826
- Received for publication August 11, 2021.
- Revision received November 22, 2021.
- Accepted for publication December 2, 2021.
- © 2022 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}
{kind=link}