
Abstract
PURPOSE The purpose of this study is to evaluate recent trends in primary care physician (PCP) electronic health record (EHR) workload.
METHODS This longitudinal study observed the EHR use of 141 academic PCPs over 4 years (May 2019 to March 2023). Ambulatory full-time equivalency (aFTE), visit volume, and panel size were evaluated. Electronic health record time and inbox message volume were measured per 8 hours of scheduled clinic appointments.
RESULTS From the pre-COVID-19 pandemic year (May 2019 to February 2020) to the most recent study year (April 2022 to March 2023), the average time PCPs spent in the EHR per 8 hours of scheduled clinic appointments increased (+28.4 minutes, 7.8%), as did time in orders (+23.1 minutes, 58.9%), inbox (+14.0 minutes, 24.4%), chart review (+7.2 minutes, 13.0%), notes (+2.9 minutes, 2.3%), outside scheduled hours on days with scheduled appointments (+6.4 minutes, 8.2%), and on unscheduled days (+13.6 minutes, 19.9%). Primary care physicians received more patient medical advice requests (+5.4 messages, 55.5%) and prescription messages (+2.3, 19.5%) per 8 hours of scheduled clinic appointments, but fewer patient calls (−2.8, −10.5%) and results messages (−0.3, −2.7%). While total time in the EHR continued to increase in the final study year (+7.7 minutes, 2.0%), inbox time decreased slightly from the year prior (−2.2 minutes, −3.0%). Primary care physicians’ average aFTE decreased 5.2% from 0.66 to 0.63 over 4 years.
CONCLUSIONS Primary care physicians’ time in the EHR continues to grow. While PCPs’ inbox time may be stabilizing, it is still substantially higher than pre-pandemic levels. It is imperative health systems develop strategies to change the EHR workload trajectory to minimize PCPs’ occupational stress and mitigate unnecessary reductions in effective physician workforce resulting from the increased EHR burden.
INTRODUCTION
There are not enough hours in the day for primary care physicians (PCPs) to do all that is expected of them. It would take nearly 27 hours per day to follow national guidelines for acute, chronic, and preventive care.1 In addition to seeing patients in face-to-face and telemedicine appointments, PCPs are experiencing growing demands to manage electronic health record (EHR) inbox messages2,3 and may feel increasingly tethered to the EHR.4 Many inbox messages require substantial time to address including responding to telephone calls, patient medical advice requests, prescription refill requests, results review, and electronic consults (PCP communications with other physicians for formal input on clinical care without seeing the patient). At the same time, many PCPs have reduced their clinical time or expressed an intent to leave practice in the near future, potentially due to the burnout associated with work on weekends, holidays, early mornings, and late nights to catch up from the overflowing demands of the week.5-8
Following the COVID-19 pandemic onset, clinicians spent more total and after-hours time in the EHR in the second half of 2020 compared to the pre-pandemic period of December 2019-March 2020.2 This increase in EHR time was partially driven by an increase in messages from patients—which rose 57% compared to the pre-pandemic average—as each additional patient message was associated with a 2.32-minute increase in EHR time per day. Looking at primary care specifically, Nath and colleagues found PCPs had a 15.6% increase in inbox time from 21.7 minutes per day pre-pandemic (March 2018-February 2020) to 25.1 minutes per day the following year (March 2020–June 2021).3 Patient medical advice requests represented the largest surge in message volume over this period, rising 104.9% from 1.8 to 3.9 messages per day. Both studies showed that after the initial pandemic-associated increases, message volume plateaued at levels above the pre-pandemic baseline despite a return to near normal volumes of in-person visits. Even if message volumes remained stable, these trends are concerning as higher message volumes are associated with greater rates of burnout.7,8 Primary care physicians spend more time in the EHR and receive more inbox messages than physicians in other specialties,9 so it is critical to understand how PCPs’ EHR workload has continued to change since prior to the onset of the COVID-19 pandemic. Using data from May 2019 through March 2023, this study aimed to assess trends in PCPs’ EHR workload from 1 year prior to 3 years following the onset of the pandemic.
METHODS
This longitudinal study of primary care EHR workload included PCPs who practiced family medicine, internal medicine, and general pediatrics for the duration of May 2019 to March 2023 at UW Health, the integrated health system of the University of Wisconsin-Madison which cares for nearly 300,000 primary care patients each year. Physician demographics including specialty, sex, years at UW Health, ambulatory full-time equivalency (aFTE), panel size, clinic hours, and visit volume were evaluated. Monthly EHR usage and scheduling data were collected for each PCP from the EHR (Epic Systems). Seven measures of EHR time were calculated on a monthly basis for each PCP and normalized per 8 hours of scheduled clinic appointments: total EHR time (EHR8), time in notes (Notes8), time in InBasket (Inbox8), time in orders (Orders8), time in clinical review (Review8), time outside scheduled hours on days with scheduled appointments (TOSH8), and time on unscheduled days (TUSD8).10 The volume of 5 inbox message types PCPs received was also calculated per 8 hours of scheduled clinic appointments: telephone calls (PatientCall8), prescriptions (Rx8), results (Result8), patient medical advice requests (MyChart8), and electronic consults (eConsult8).
The methods employed in this study have certain limitations. The Inbox8 measure only captures time spent on dedicated inbox screens, so it does not include all time needed to address messages and thus likely underestimates the total time required to manage the inbox. The TOSH8 measure excludes all time from one-half-hour before to one-half-hour after the first to the last scheduled clinic appointment of each day, respectively, so it may underestimate EHR use outside scheduled clinic appointments.11 Additionally, Epic’s vendor-defined method of measuring active EHR use times out after 5 seconds of inactivity and thus likely underestimates total EHR time especially when engaged in tasks such as reading notes.
Unadjusted comparisons of PCP demographics and workload across primary care specialties were performed with χ2 tests for count data and Kruskal-Wallis H tests for continuous variables. Multivariable linear regression was used to compare EHR time and message volume across 4 years: May 2019 to February 2020 (pre–COVID-19 pandemic); June 2020 to March 2021; May 2021 to March 2022; and April 2022 to March 2023. Each model included data across all 4 years and treated study year as a categorical variable and controlled for correlation between monthly measures of EHR use by PCP (using random effects), specialty, and month of the year to account for seasonality. The Benjamini-Hochberg procedure was used to adjust P values for multiple comparisons across all models, using a false-discovery rate (FDR) of 5% (FDR = 0.05). Because many PCPs reduced their aFTE during the study period, we conducted a sensitivity analysis with EHR time and message volume normalized per aFTE-week. We collected 48 months of data covering April 2019 to March 2023, but excluded 6 months of data from the analysis including March 2020 to May 2020 due to the dramatic and transitory changes in EHR use early in the COVID-19 pandemic,2 and April 2019, April 2021, and May 2022 due to incomplete EHR use data. This study was approved by University of Wisconsin’s Health Sciences Institutional Review Board.
RESULTS
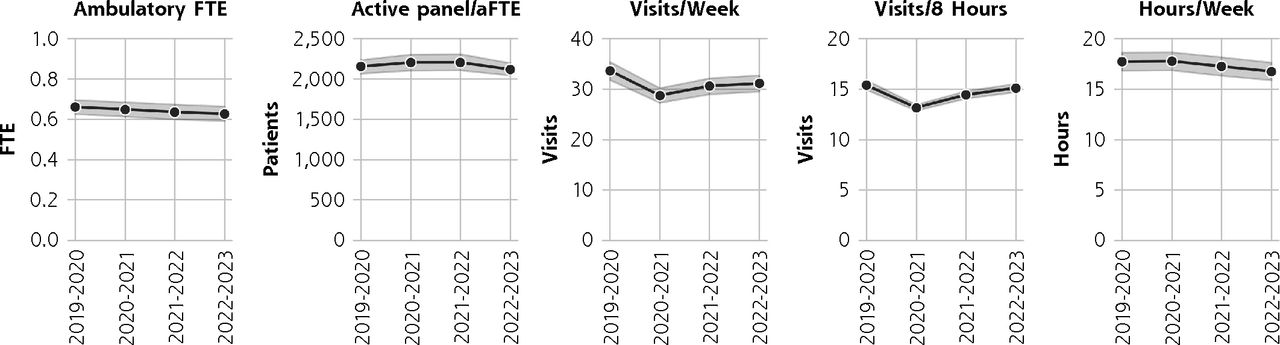
Of the 141 PCPs included in this study, nearly one-half (49.6%) practiced family medicine and two-thirds (66.7%) were female (Table 1). Primary care physicians’ average aFTE decreased significantly throughout the study (Figure 1), dropping 5.2% from 0.66 in the pre-pandemic year of May 2019 to February 2020 to 0.63 in the final study year of April 2022 to March 2023. Average active panel size per aFTE, visits per 8 hours of clinic, visits per week, and hours of clinic per week were all also significantly lower in April 2022 to March 2023 than they were in May 2019 to February 2020, though visit volumes had rebounded from their low in June 2020 to March 2021 (Table 2).
Physician Demographics and Workload by Specialty

Primary care physicians’ average workload by year.
aFTE = ambulatory FTE; FTE = full-time equivalency.
Note: Grey band represents 95% confidence interval.
EHR Time and Inbox Message Volume by Study Year
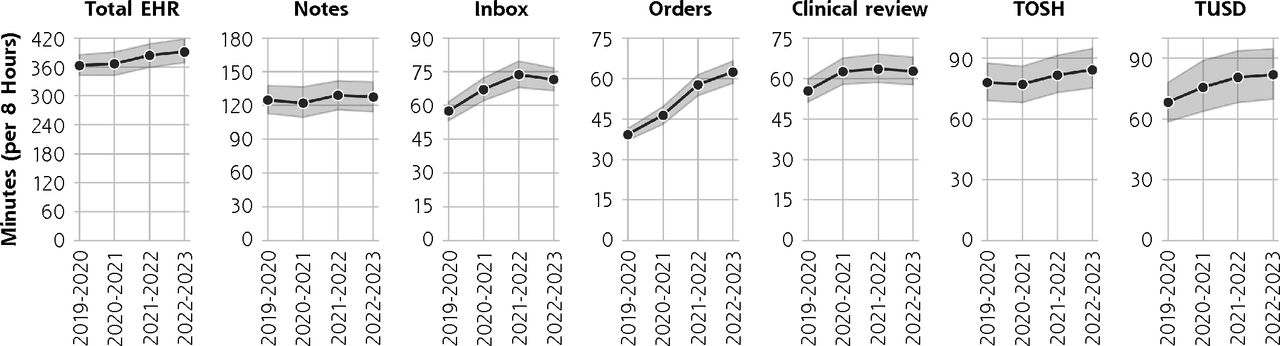
All 7 measures of EHR time per 8 hours of scheduled clinic appointments increased significantly between May 2019 to February 2020 and April 2022 to March 2023 (Figure 2) including EHR8 (+28.4 minutes, 7.8%), Orders8 (+23.1 minutes, 58.9%), Inbox8 (+14.0 minutes, 24.4%), Review8 (+7.2 minutes, 13.0%), Notes8 (+2.9 minutes, 2.3%), TOSH8 (+6.4 minutes, 8.2%), and TUSD8 (+13.6 minutes, 19.9%). The direction and significance of changes in EHR time between these years was the same when normalized per aFTE-week, except that the increase in time in notes was no longer significant (Supplemental Table). Among the year-on-year changes, Inbox8 and Review8 decreased marginally but significantly between the final 2 years of the study after significantly increasing each of the prior years (Table 2).

Primary care physicians’ average time in the EHR by year.
EHR = electronic health record; TOSH = time outside scheduled hours on days with scheduled appointments; TUSD = time on unscheduled days.
Note: Time in notes, inbox, orders, clinical review, outside scheduled hours on days with appointments, and on unscheduled days are included in total EHR time. Grey band represents 95% confidence interval.
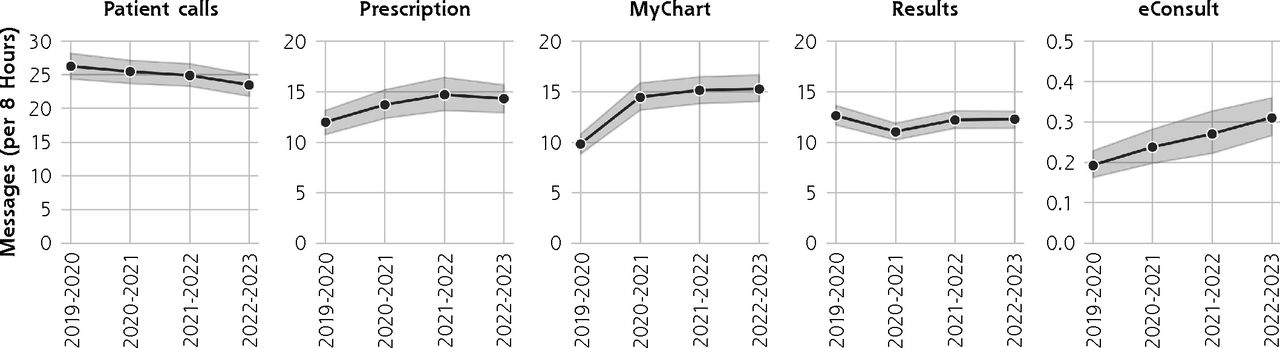
The volume of messages PCPs received per 8 hours of scheduled clinic appointments increased significantly between May 2019 to February 2020 and April 2022 to March 2023 for 3 message types (Figure 3) including MyChart8 (+5.4 messages, 55.5%), Rx8 (+2.3 messages, 19.5%), and eConsult8 (+0.12 messages, 61.0%) while the volume of PatientCall8 (−2.8 messages, −10.5%) and Results8 (−0.3 messages, −2.7%) both decreased. The direction and significance of changes in message volume between these years was the same when normalized per aFTE-week (Supplemental Table). Among the year-on-year changes, Rx8 decreased and MyChart8 increased, though not significantly, between the final 2 years of the study after significantly increasing each of the prior years (Table 2).

Primary care physicians’ average volume of select inbox message types received by year.
eConsult = electronic consult.
Note: Grey band represents 95% confidence interval.
DISCUSSION
The PCPs in this study experienced continued increases in total EHR time per 8 hours of scheduled clinic appointments over the past 4 years into early 2023. In the final year of this study (April 2022 to March 2023), compared to the pre-pandemic year (May 2019 to February 2020), PCPs spent nearly 30 minutes more in the EHR (7.8% increase) per 8 hours of scheduled clinic appointments. Both time in the EHR outside scheduled hours on days with appointments (TOSH8) and time on unscheduled days (TUSD8) also increased by 6.4 (8.2%) and 13.6 (19.9%) minutes, respectively.
Considering year-on-year changes, our results show Inbox8 rose then stabilized around 1 hour and 12 minutes in the last 2 years of the study (73.6 minutes in April 2021 to March 2022, 71.4 minutes in April 2022 to March 2023). The volume of MyChart and prescription messages PCPs received both increased significantly compared to pre-pandemic levels—55.5% and 19.5%, respectively—though their volume may have stabilized over the last 2 years of the study. Patient call volumes continued to trend down year-on-year which may be due to a shift to MyChart messaging to seek medical advice. The significant and steady rise in time in orders over the 4 years of the study (58.9% increase) is particularly concerning, although it is unclear what has led to the increase. One possibility is that the complexity of some MyChart messages and patient calls may be increasing as PCPs work with their patients to avoid visits. This could result in PCP orders in these encounters that are not touched by other team members.
Prior work found stabilization in message volumes through early 2021 after initial increases at the onset of the COVID-19 pandemic, while this study found they increased into early 2022 before stabilizing.2,3 These differences in our results are likely due to differences in specialty (eg, primary care vs all ambulatory specialties), health system, and timeframe observed. Whereas the prior studies stopped in December 2020 and May 2021, this study observed EHR use through March 2023. The normalized EHR time and inbox message volumes reported here may also appear higher than those reported in prior work2,3,9,12 due to normalizing EHR workload by 8 hours of scheduled clinic appointments rather than days logged into the EHR. When normalized per login day, Nath and colleagues reported that PCPs spent 25.1 minutes per day on inbox tasks from March 2020 to June 2021; we found the PCPs in our study spent a similar, though slightly higher, 27.7 minutes per day on inbox tasks during the overlapping timeframe of June 2020 to March 2021.3
The reasons for the observed increases in EHR time and some message volumes are likely multifaceted. Physicians in the United States receive nearly 3 times the messages as physicians elsewhere, presumably due to differences in policy and practice climates.12 There has been steady growth in the percent of UW Health primary care patients signed up for MyChart access with nearly 80% now having an active MyChart account. Additionally, the rapid shift to virtual care at the onset of the COVID-19 pandemic likely influenced patient expectations regarding telemedicine and portal access, and some patients may expect same-day responses directly from their PCP in lieu of an in-person or telemedicine visit. As a result of the 21st Century Cures Act requiring immediate result release to patients, it is not uncommon for PCPs to have new MyChart messages with questions about results within minutes of their release.13 These MyChart messages are often seen by the PCP before they see the result in the inbox. These policy changes impact primary care patient messaging behaviors and, therefore, overall PCP workload and associated burnout.14 Mental health needs have grown dramatically, and primary care teams have taken on many of these new needs in the context of a substantial shortage of behavioral health clinicians.15 Additionally, some of the initial increase in inbox volume was likely COVID-related vaccine, testing, and treatment questions that often bypassed traditional visits; however, much of this volume has since subsided.
Although increasing EHR workload has negative implications for physician well-being7,8 and potentially patient safety, Melnick and colleagues found that physicians perceive the EHR as valuable for patient care, and that higher perceived EHR usability tempers the perceived negative outcomes in terms of work-life integration.16 Additionally, Rotenstein and colleagues found greater EHR time was associated with better chronic disease and preventive care quality metrics.17 However, the positive associations were primarily noted among PCPs with clinical FTEs of 0.5 or less and below-average panel sizes. These findings suggest the cost of this increased EHR time may only be afforded by PCPs with lower clinical loads. Even then, the ability to take on additional EHR work is limited as physicians with lower clinical FTEs spend more time in the EHR per hour of clinic than their full-time peers.18 When some PCPs reduce their aFTE with intent to reduce overall workload, their total EHR workload may remain high if their panel size does not proportionally decrease—which can result in unpaid work in compensation plans largely based on billable patient visits.
The overarching goal in examining EHR workload trends in primary care is to influence policy that leads to potential adjustments in team structure, panel size expectations, visit volume and duration, and level-loading clinical staff support and synchronous visit capacity by day of the week.19,20 This may enhance the feasibility of the work and thus improve patient care and physician well-being. Improvements in clinical resources and realistic visit capacity could potentially create more real-time opportunities during clinic hours for PCPs to address asynchronous clinical work rather than during personal time outside scheduled clinic hours.
Limitations
This study focused on EHR workload experienced by PCPs, although non-physician primary care team members may also be experiencing increasing workload as they work to support the growing volume of overall acute, chronic, and preventive care needs of primary care patients. We also did not explore differences in time expenditure and message volume by primary care specialty as prior work has identified significant differences in EHR workload across primary care specialties.21 This study used disaggregated time data to assess how long PCPs spent on specific EHR activities such as inbox management. Time spent on some activities, such as viewing patient schedules, was not independently assessed, though it was included in measures of total and outside hours EHR time. Additionally, this study was conducted at a single academic health center employing a single EHR. This study did not examine variation in EHR workload by physician, though Cross and colleagues have demonstrated that most variation in EHR time is attributable to variation by physician rather than by health system, suggesting there are unrealized opportunities for organizations and policy makers to support consistency in how physicians engage in EHR-supported work.22 Finally, UW Health has a highly capitated primary care population. Nearly 45% of the patients associated with the PCPs in this study are in value-based payment arrangements. The asynchronous patient demands and associated responses by our primary care team may differ from health systems that provide more fee-for-service care as physicians who participate in Accountable Care Organizations or other pay-for-performance programs have a higher documentation burden and spend more time on documentation outside office hours.23
CONCLUSION
PCPs’ time in the EHR continues to grow. With high demand for asynchronous patient care, including a sustained increase in the volume of patient medical advice messages, it is imperative health systems develop strategies to change the overall EHR workload trajectory to minimize PCPs’ occupational stress and mitigate unnecessary reductions in the effective physician workforce that result from the increased EHR burden. Approaches might include reducing inbox volumes through policy change, redesigning primary care workflows and teamwork, and resetting patient expectations.
Footnotes
Conflicts of interest: Dr Sinsky is employed by the American Medical Association. The opinions expressed in this article are those of the authors and should not be interpreted as American Medical Association policy. All other authors report none.
Author contributions: All authors (B.G.A., M.A.M., A.R., C.M.S., J.J.B., C.A.S.) have made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafting the work or revising it critically for important intellectual content; and final approval of the version to be published; and agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Dr Sinsky of the AMA assisted in the interpretation of findings and contributed to the manuscript; the AMA had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Funding support: This work was supported in part by the American Medical Association (AMA) Practice Transformation Initiative: EHR-Use Metrics Research which has provided grant funding (#16114) for authors B.G.A., M.A.M., C.M.S., and J.J.B.
Data availability statement: The data that support the findings of this research study are maintained securely by UW Health according to security standards recommended by the University of Wisconsin’s health sciences institutional review board. The data are not publicly available.
- Received for publication November 2, 2022.
- Revision received August 23, 2023.
- Accepted for publication September 5, 2023.
- © 2024 Annals of Family Medicine, Inc.




{kind=link}
{kind=link}
{kind=link}