
Abstract
PURPOSE Black birthing parents and their newborns disproportionately experience newborn drug testing for prenatal substance exposure by health care professionals (HCPs), which contributes to Child Protective Services (CPS) reporting, family separation, and termination of parental rights. This qualitative study aims to interrogate dominant power structures by exploring knowledge, attitudes, and experiences of HCPs and CPS professionals regarding the influence of structural racism on inequities in newborn drug testing practices.
METHODS We conducted semistructured interviews with 30 physicians, midwives, nurses, social workers, and CPS professionals guided by an explanatory framework, and conducted inductive, reflexive thematic analysis.
RESULTS We identified 3 primary themes: (1) levels of racism beyond the hospital structure contributed to higher rates of drug testing for Black newborns; (2) inconsistent hospital policies led to racialized application of state law and downstream CPS reporting; and (3) health care professionals knowledge of the benefits and disproportionate harms of CPS reporting on Black families influenced their decision making.
CONCLUSION Health care professionals recognized structural racism as a driver of disproportionate newborn drug testing. Lack of knowledge and skill limitations of HCPs were barriers to dismantling power structures, thus impeding systems-level change. Institutional changes should shift focus from biologic testing and reporting to supporting the mutual needs of birthing parent and child through family-centered substance use treatment. State and federal policy changes are needed to ensure health equity for Black families and eliminate reporting to CPS for prenatal substance exposure when no concern for child abuse and neglect exists.
INTRODUCTION
The United States Child Abuse and Prevention Treatment Act requires states to enact policies to identify newborns affected by substance use disorders or prenatal substance exposure (PSE) during pregnancy.1 Thirty-seven states and the District of Columbia go beyond federal requirements by requiring health care professionals (HCPs) to file a report for PSE to child welfare agencies, even in the absence of true HCP concerns for child abuse.2,3 For example, Michigan’s Child Protection Law requires reporting of suspected child abuse or neglect for suspicion of PSE.4 Black pregnant people and their newborns are more likely to undergo biologic testing for substance exposure than their White counterparts despite a similar prevalence of substance use.5,6 In a retrospective cohort study of 26,366 live births in Michigan, Black newborns were 3.8 times more likely to be tested for drugs than White newborns when there was no biologic test performed during pregnancy.7 Such biologic testing has been linked to disproportionate reporting to Child Protective Services (CPS).8-13 Once subjected to CPS investigation, Black parents face harsher penalties than other racial groups including family separation and termination of parental rights.14-17 The American College of Obstetrics and Gynecology opposes criminalization of substance use in pregnancy, noting that implicit bias on the basis of race or class influences coercion and criminalization.18
Structural racism is a root cause of the disparities in adverse health outcomes faced by Black families and mediates these outcomes in multiple, intersecting pathways, including federal, state, local, and institutional policies and interpersonal discrimination and microaggression.19-22 In the context of PSE, neighborhood poverty and lack of health care resources may lead to late presentation for prenatal care and lower rates of substance use treatment.23-25 When hospital systems implement testing policies based on risk factors, these social determinants may lead to disproportionate testing of Black people.26,27 Historical racism within racialized organizations and the “war on drugs” drive greater HCP suspicion of substance use among Black people via interpersonal racism. And, when state policies consider substance exposure to be abuse or neglect, Black people are exposed to higher rates of criminalization and its downstream economic, financial, familial, and emotional consequences.14,15,17,28
Examination into the role of HCPs in these pathways has shown that HCPs were concerned about possible harms but lacked knowledge about the details of CPS investigations and about how to change CPS reporting policies.29-34 Few of these studies examined the contributions of structural racism and obstetric racism (defined as mutually reinforcing systems of racial discrimination operating at multiple levels and threatening the well-being of Black birthing people and their newborns) at the health care system level, leaving a gap in understanding how dominant power structures and practices operate at the institutional level to foster racial inequities in newborn drug testing (NDT).23,34,35
This qualitative analysis is part of a larger antiracist, justice-informed, community-engaged, multiphase mixed methods study. An initial quantitative retrospective cohort analysis showed that clinicians are more likely to order drug testing on Black newborns compared with White newborns and other racial and ethnic groups.7 A second qualitative phase examines attitudes and experiences of recently pregnant patients who experienced NDT.36 In this third qualitative phase, the primary aim is to interrogate dominant power structures through interviews of HCPs and CPS professionals to understand the mechanisms by which structural racism influences HCP’s behavior. A secondary aim is to understand to what extent HCPs’ and CPS professionals’ observed knowledge, attitudes, and experiences reinforce policies that maintain racial inequities.
METHODS
Research Team and Reflexivity
Our study team members’ intersecting identities and shared commitment to practicing antiracism and reducing health inequities affected study design, interactions with study participants, and data analysis. Our perspectives include intersecting racial and ethnic identities (African American, Asian-American, Latin-American, immigrant, and first-generation American), salient lived experiences (Black birthing individual), and disciplines (obstetrics and gynocology, family medicine, addiction medicine, public health, and sociology). To interrogate power systems from an antiracist perspective and elevate community perspectives, we consulted with 2 scholars with expertise in antiracist research and convened 3 meetings with a participatory council of maternal child health advocates and parents identified as community change champions.
Setting
The study was conducted at the University of Michigan, a large academic health system in the Midwestern United States in a county with a racial distribution of Asian (9.2%), Black (12.2%), Hispanic or Latine (5.2%), multiracial (3.8%), and non-Hispanic White (74.3%) individuals.28 During the study period, there was no formal policy regarding NDT, leaving decisions to the discretion of the HCP. This study was considered exempt by the Institutional Review Board of the University of Michigan Medical School (HUM00198997) as procedures were deemed no more than minimal risk.
Participant Selection
Eligible study participants included HCPs who provided obstetrical or newborn care within the last 12 months or CPS staff members working in Washtenaw County. We recruited potential participants by e-mail, first approaching clinical leaders and then using snowball sampling to recruit participants with different roles and clinical sites. We interviewed a total of 30 participants in 4 groups, and conducted 20 individual interviews from May 2021 through October 2022 at which point we achieved thematic saturation and adequate representation of HCP roles.37
Explanatory Framework
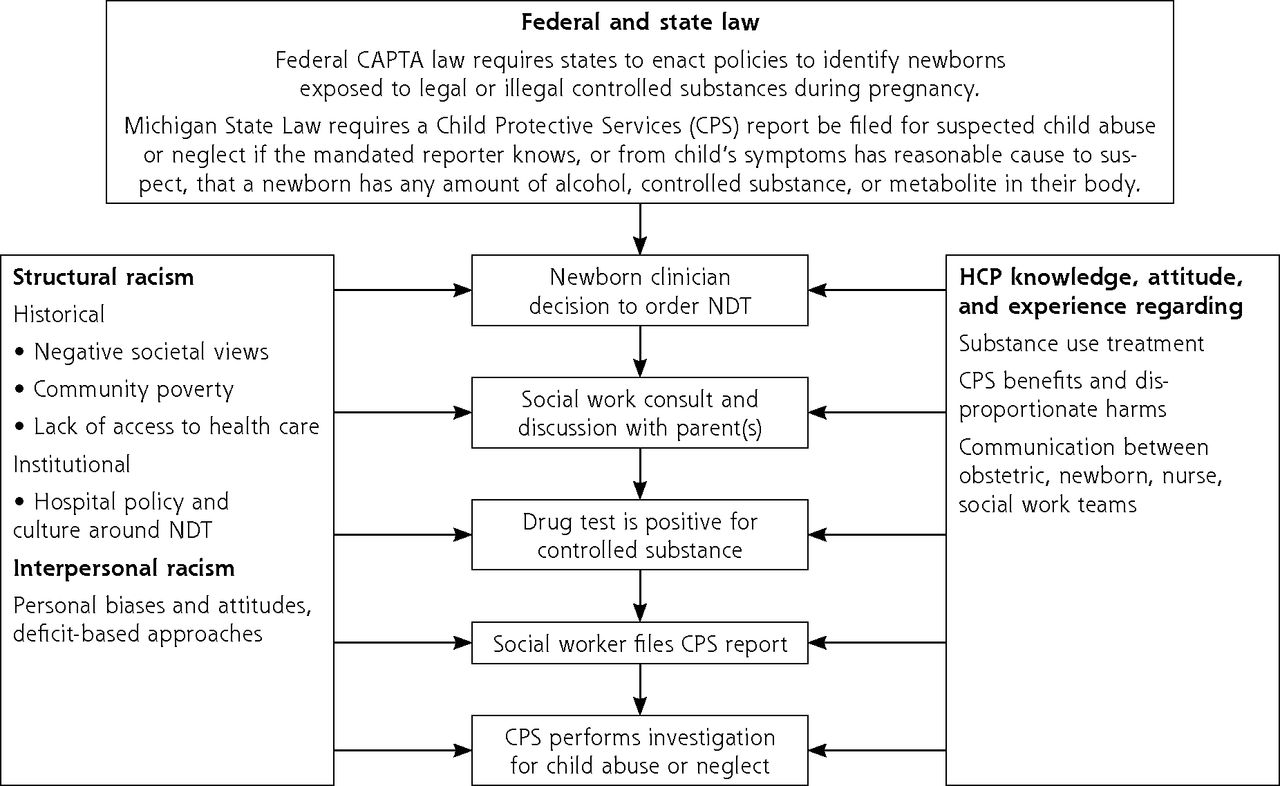
We developed and iteratively refined a framework to describe potential influences of structural racism on HCP decision making about NDT (Figure 1). We adapted elements from other frameworks that included: the Levels of Racism Framework, which identified the manifestations of structural (ie, institutional, historical) and interpersonal racism at multiple socio-ecological levels underlying NDT inequities38; the Theoretical Domains Framework, which uses behavior change theories to account for how HCP and CPS professional knowledge, skills, role, social and team influences, and beliefs impact decision making39; domains from a framework focused on the perspectives of Black women (community resources, policing, education)24; and the Public Health Critical Race Praxis, which conceptualizes race as proxy exposure to systematic racism, centers the perspectives of marginalized people, and emphasizes community perspectives in the research process.40

Explanatory framework of potential influences of structural racism on health care professional decision making in newborn drug testing.
CAPTA = Child Abuse and Prevention Treatment Act; CPS = child protective services; HCP = health care professional; NDT = newborn drug testing.
Data Collection
Team members developed, piloted, and revised a semistructured interview guide (Supplemental Appendix) informed by the framework to elicit the potential influence of racism at multiple levels on HCP decision making to order NDT. After obtaining written informed consent, a study team member (C.S., V.W., L.O., A.C.) conducted group interviews (with 2-4 participants with similar roles, such as pediatrician or CPS staff) or individual interviews if scheduling prohibited group participation. Interviews lasted 45-60 minutes. Interviews were audio recorded, transcribed verbatim, and cross-checked against recordings for accuracy. The team recorded field notes and debriefed findings after each interview.
Data Analysis
We selected reflexive thematic analysis, which allowed us flexibility in rich inductive coding, engagement of researcher positionality and reflexivity, and application of an explanatory framework to elucidate latent themes from the data.41 Six team members (C.S., L.O., A.C., V.W., E.M., M.J.) coded transcripts with at least 2 coding each transcript and a single senior investigator adjudicating any disagreement. We organized codes and related field notes into preliminary themes according to our framework. The team convened regularly and used a consensus approach to refine the codebook and to synthesize final themes.42 To enhance the credibility of our analysis, we utilized a paired coding approach to balance clinical and non-clinical perspectives, frequent team meetings to develop depth of understanding of our data, and used team discussion to understand discrepancies and collectively synthesize findings.43 To improve rigor in the data analysis, we identified salient perspectives and assumptions shaped by our personal backgrounds and professional experiences and regularly discussed the ways that these preconceptions may influence our research conceptualization, analytical approach, and interpretation of findings.44,45 Analysis was performed using Dedoose 9.0 software (SocioCultural Research Consultants).46 The description of this study followed the Consolidated Criteria for Reporting Qualitative Research.47
RESULTS
We interviewed 30 participants (P1 to P30) that included 5 certified nurse midwives, 4 nurses, 1 social worker, 4 CPS professionals, and 16 attending or resident physicians from the specialties of family medicine (4), medicine-pediatrics (1), obstetrics and gynecology (3), pediatrics (8). Additional demographics are represented in Table 1.
Characteristics of Study Participants (N = 26)
We identified 3 themes: (1) levels of racism beyond the hospital structure contributed to higher rates of NDT for Black newborns; (2) inconsistent hospital policies led to racialized application of state law and downstream CPS reporting; and (3) HCP knowledge of the benefits and disproportionate harms of CPS reporting on Black families influenced their decision making about testing. Theme descriptions, relevant sub-themes, and representative quotes are presented in Table 2.
Themes and Representative Quotations
Theme 1. Racism Contributed to Greater NDT of Black Newborns
Participants observed historical, institutional, and interpersonal manifestations of racism in their practices. A midwife noted that historical negative societal views of drug use in Black communities impacted their application of risk-based screening, “…long-standing implicit bias coming out of the 80’s and the war on drugs.” (P19) A family physician added that contemporary racialized views of drug use persist with cannabis use, “…an association in my mind with my African American patients.” (P16) A labor and delivery nurse identified complex racialized community barriers, including late presentation to care as targeting Black patients for NDT, “…your first go-to should[n’t] be a drug screen.” (P22) A pediatrician framed drug testing as marginalizing Black people in a hospital with predominantly White HCPs, “…when families … have different coping mechanisms [staff] can … think that something [related to drug use] is going on.” (P1) A midwife contextualized the disrespect and harm of NDT as obstetric racism, “…women of color are targeted in so many ways.” (P19)
Theme 2. Hospitals Racialized Application of State Law and CPS Reporting
Several participants perceived that the lack of a standardized institutional policy led to variable and subjective application of state law resulting in greater testing and risk of CPS reporting for Black patients. A family physician felt that state law was difficult to operationalize into specific indications for NDT, “…nobody has clarity including the state.” (P17) A labor and delivery nurse expressed concerned that the absence of “streamlined set criteria… leads to bias.” (P22) A certified nurse midwife observed that HCPs’ retain discretion to suppress NDT orders based on patients’ race, ethnicity, and socioeconomic background in ways that privilege “a fancy [White] professor who just smokes weed every now and then.” (P24)
Theme 3. Knowledge of CPS Reporting Influenced Testing Decisions
Some felt CPS reporting was critical for child protection, some were concerned that CPS reporting caused harm, and others lacked awareness of outcomes of CPS reporting. A pediatrician disclosed, “I don’t know what happens when CPS is contacted,” (P2) regarding lack of knowledge about the process of investigation for alleged abuse or neglect after filing a CPS report. One pediatrician stated, “Without that test we can’t protect the baby,” (P9) perceiving that biologic test results were necessary to trigger an investigation to ensure the newborn’s safety if the parent used substances during pregnancy. Another pediatrician contextualized the positives of a CPS home visit as “more like a resource safety net” (P26) to identify social and material needs. A CPS professional noted that reports of substance exposure require an investigation but “we have to dig … and see if there’s some other neglect tied to it” (P10) in order to open a case against the parent. A social worker agreed that when a case is not opened there is “nothing on this record under CPS.” (P7)
Other participants explicitly raised concerns about the harms of CPS reporting, particularly to Black people. A family physician noted that reporting for PSE was “mostly a punitive thing” (P18) and exacerbated mistrust of the health care system among Black and Brown communities. A midwife felt that Black patients may not disclose substance use to their treatment team because “you’re going to be treated badly for [it],” (P24) and the risk of CPS reporting outweighed the benefit of getting care. A CPS professional reflected that reporting triggered a chain reaction of unknown consequences, “where we don’t know what could potentially happen as they move through,” (P10) noting that a system that focused on treatment would be more appropriate. Finally, one participant hoped that testing would connect families to resources and “to get [the parent substance use] help and resources to have a family thrive,” (P3) but did not articulate how sending NDT results might actually connect families with these supportive services.
DISCUSSION
This qualitative study of HCPs and CPS professionals illuminates how racist practices in NDT may be perpetuated at the institutional level by dominant power structures. Consistent with our explanatory framework, HCPs recognized that structural racism underlies higher rates of drug testing on Black newborns. Similar to previous studies, we observed that HCPs lacked knowledge regarding the disproportionate harms of CPS reporting for Black families, found state law to be confusing and difficult to implement, and held beliefs that reinforce current practices and maintain racial inequities.31-33
Health care professionals can be powerful change agents when their beliefs and attitudes support implementation of new practices to achieve health equity.48 Many HCPs in this study, however, lacked knowledge about harms of reporting, especially to Black families, including the generation of mistrust of the health care system, avoidance of health care and substance use treatment, substantiation of abuse and neglect claims, family separation, and harm of exposure to the foster care system.14,49 While some HCPs in our study suggested that universal biologic testing could eliminate the inequities seen in biased application of risk-based testing, prior studies show inconsistent results regarding a reduction in racial inequities with either standardized risk-based or universal testing policies.6,27,50 The Doing Right at Birth course is a self-paced tool that HCPs may use to develop knowledge regarding family-centered substance use care in pregnancy, legally mandated reporting requirements, and how to advocate for changes to ensure that reporting of families to child welfare meets, but does not exceed, legal requirements.51
While this study focused on the level of the HCP, our results reflect institutional policies and interpersonal bias characteristic of a racialized organization that must be addressed as part of the implementation of reforms that focus on safety, dignity, and justice for Black birthing people.28 At the institutional level, systems change requires aligning goals toward supporting the birthing parent–infant dyad and framing needs of birthing parent and child as mutually supportive.52 Interventions to guide health care system transformations could employ the Cycle to Respectful Care to commit to antiracist institutional transformations53 and the Birthing Bill of Rights to provide equitable care, focusing on providing interventions for family-based supports.54 Clinical practice guidelines and exemplar approaches exist to guide hospital policy that moves focus from testing and reporting to a holistic approach to substance use treatment focused on harm reduction and support of the family unit.55-57
Further state and federal policy changes are needed to attain health equity for Black families. We advocate for delinking substance use with CPS reporting; mandated reporters should instead perform a holistic assessment and make CPS reports only when factors beyond substance use create a concern for abuse and neglect.58 An anonymous notification processes for PSE separate from current CPS reporting and compliant with the Child Abuse and Prevention Treatment Act, such as enacted in Vermont, should be implemented.59-61 Health care professionals can advocate for the allocation of additional substance use treatment resources focused on pregnant Black people to reduce harm from involvement of child welfare systems.62
While reflective of the overall lack of racial, ethnic, and gender diversity in the health care workforce, our study sample is limited to a predominantly White and female demographic and does not capture the distinctive experiences of Black and other minoritized HCPs.63,64 Given the crucial role of social workers in CPS reporting, our study is limited by having only 1 social worker interviewed. Another qualitative phase of our study explores the diverse perspectives of patients affected by NDT to collectively inform future patient-centered and antiracist interventions.
CONCLUSIONS
Health care professionals recognized structural racism as a driver of disproportionate NDT. Their beliefs, lack of knowledge, and skill limitations were barriers to dismantling power structures impeding systems level change. Ongoing work at our institution includes implementation of risk-factor–based NDT criteria paired with an equity dashboard to track and continuously improve racial inequities in testing, education tools to improve patient knowledge of state law and institutional testing protocols, and improved counseling and linkage to treatment for pregnant people using substances. Beyond health care system change, state and federal policy changes are needed to ensure health equity for Black families and to eliminate reports to CPS for prenatal substance exposure when no concern for child abuse and neglect exists.
Acknowledgments
We acknowledge external expert consultants Courtney S. Thomas Tobin, PhD, Associate Professor, Department of Community Health Sciences, UCLA, and Bita Amani, PhD, MHS, Associate Professor, Charles R. Drew University of Medicine and Science, who provided expertise in antiracist public health research. We conducted a series of community member interviews and convened a participatory council of community advocates and experts in prenatal substance use treatment and social policy who evaluated study results and recommended dissemination and future interventions to benefit the study’s patient populations, particularly Black families. We acknowledge the participatory council members Tara Radina, LLMSW, Women Specialty Program Manager, Home of New Vision; and Connie Braxton, Coordinator, Silverspoon Maternal Infant Health Program, who were all compensated for their time.
Footnotes
Conflicts of interest: authors report none.
Funding support: This study was sponsored by the University of Michigan Office of the Vice President for Research. Dr Chandanabhumma was supported, in part, by the National Center for Advancing Translational Sciences grant number UL1TR002240.
Disclaimer: The University of Michigan Research Office and Michigan Institute for Clinical & Health Research had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. This study was considered exempt (exemption category 2) by the University of Michigan Institutional Review Board (HUM00198997). Dr Oshman and Dr Shetty had full access to all the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis.
Previous presentations: This work was presented at the following conferences: University of Michigan Diversity in Medicine Conference, March 2022, virtual; Society of Teachers of Family Medicine Annual Meeting, June 2022, Indianapolis, Indiana; Pediatric Hospital Medicine Conference Research Day, August 2023, Philadelphia, Pennsylvania; NAPCRG Annual Meeting, October 2023, San Francisco, California.
- Received for publication July 31, 2023.
- Revision received January 30, 2024.
- Accepted for publication February 2, 2024.
- © 2024 Annals of Family Medicine, Inc.




{kind=link}