
Article Figures & Data
Figures
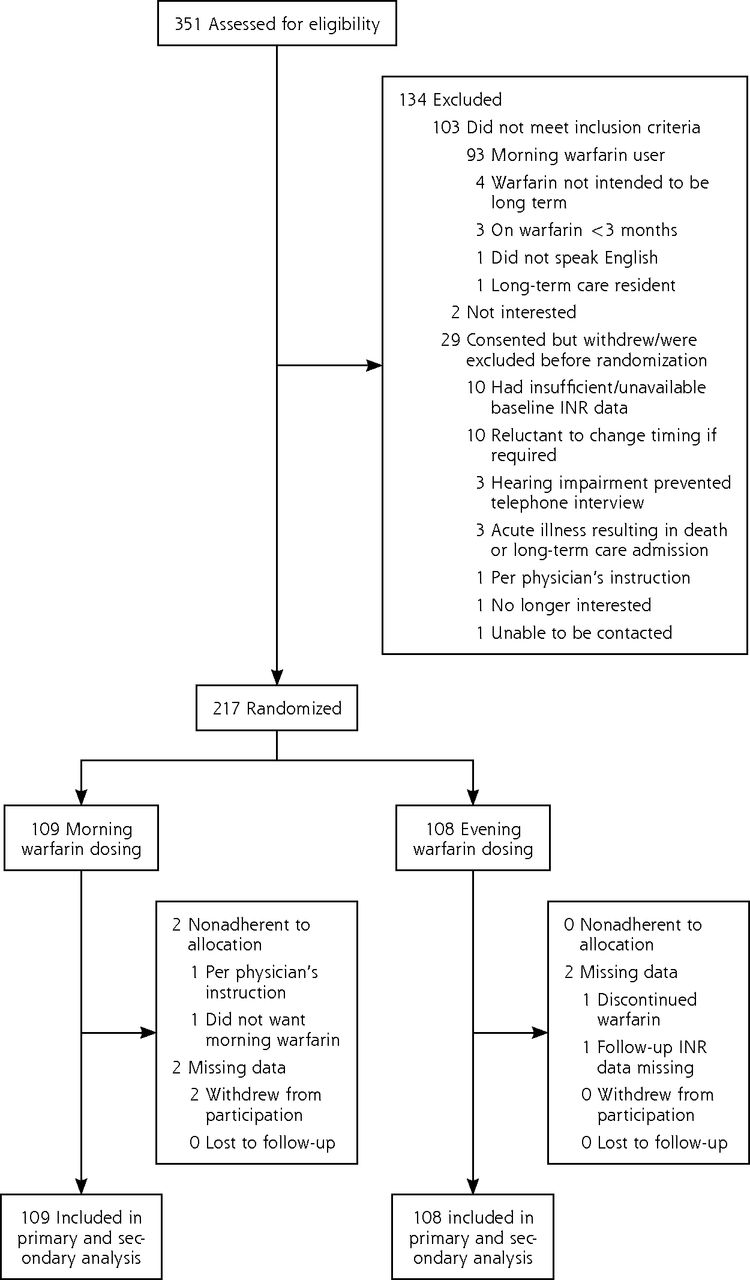
- Figure 1
CONSORT flow diagram.
CONSORT = Consolidated Standards of Reporting Trials; INR = international normalized ratio.
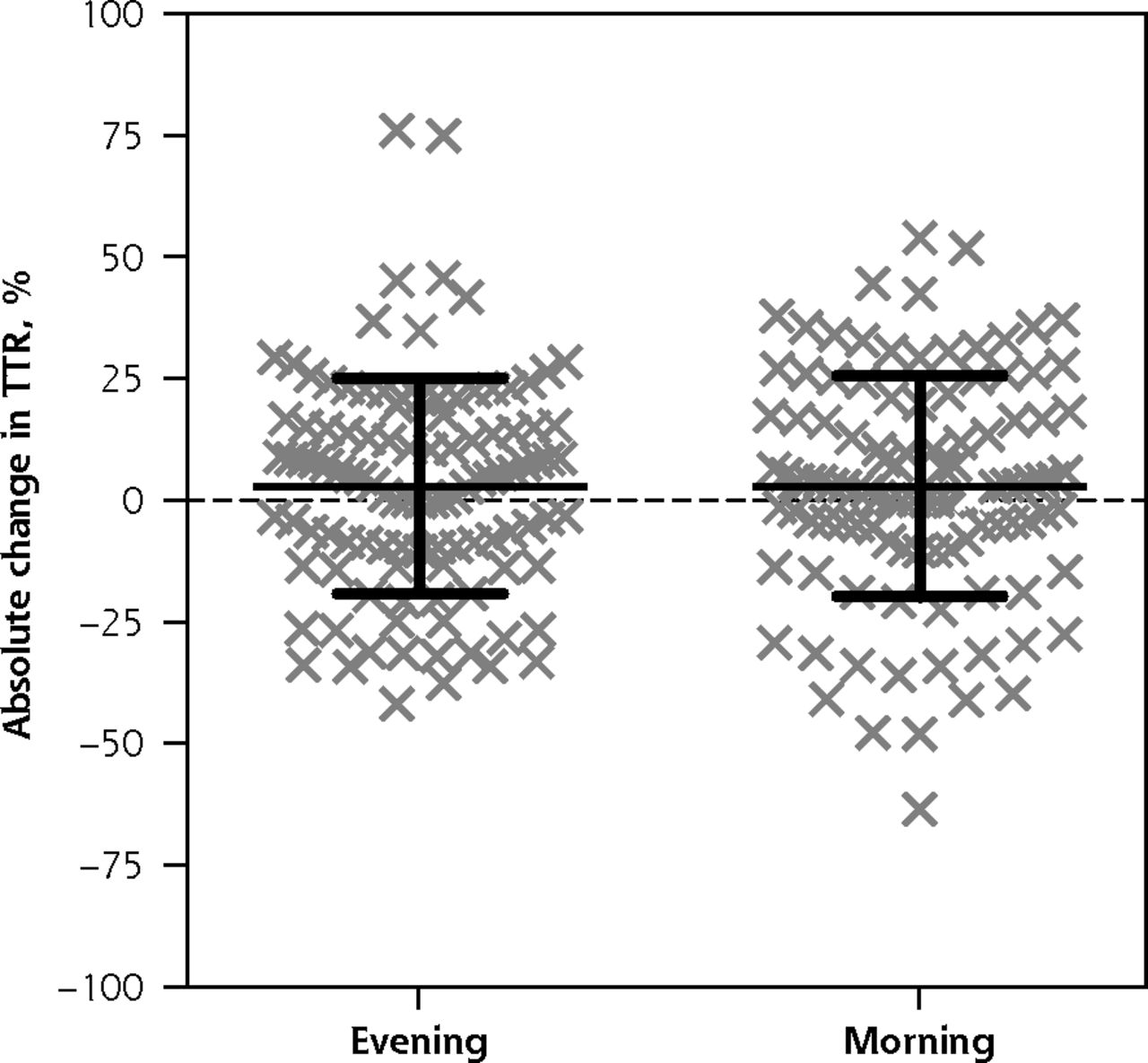
- Figure 2
Scatterplot of absolute change in TTR.
TTR = time within therapeutic range (of the international normalized ratio).
Note: Each of the 217 data points represents the absolute change in TTR for 1 study participant. The overlaid black crossbars indicate mean and SD.

Tables
Characteristic Morning (n = 109) Evening (n = 108) Sex, No. (%) Male 60 (55.0) 51 (47.2) Female 49 (45.0) 57 (52.8) Age Mean (SD), y 72.7 (10.3) 73.4 (10.3) ≥80 y, No. (%) 32 (29.4) 31 (28.7) Province, No. (%) Alberta 81 (74.3) 85 (78.7) British Columbia 28 (25.7) 23 (21.3) Location, No. (%) Urban 86 (78.9) 96 (88.9) Rural 23 (21.1) 12 (11.1) Indication for anticoagulation, No. (%) Atrial fibrillation 68 (62.4) 63 (58.3) DVT/PE 31 (28.4) 23 (21.3) Mechanical valve 11 (10.1) 12 (11.1) Other 10 (9.2) 17 (15.7) Target INR range, No. (%) 2.0-3.0 97 (89.0) 97 (89.8) 2.5-3.5 7 (6.4) 11 (10.2) Other 5 (4.6) 0 (0.0) Warfarin use Daily dose, mean (SD), mg 5.0 (2.1) 4.9 (2.2) Duration of use, mean (SD), y 7.9 (7.2) 7.4 (6.8) <6 months of use, No. (%) 2 (1.8) 4 (3.7) Forget warfarin at least once per month, No. (%) 8 (7.3) 8 (7.4) Warfarin administration time, No. (%) >30 minutes before dinner 15 (13.8) 18 (16.7) ≤30 minutes after dinner 46 (42.2) 49 (45.4) >30 minutes after dinner 13 (11.9) 5 (4.6) Bedtime 32 (29.4) 35 (32.4) Varies 3 (2.8) 1 (0.9) Stability of anticoagulation Proportion of time within therapeutic range of INR (TTR), mean (SD) 71.8 (20.2) 72.6 (19.5) Proportion of time outside of therapeutic range of INR, mean (SD) 28.2 (20.2) 27.2 (19.6) TTR >75%, No. (%) 53 (48.6) 57 (52.8) TTR <60%, No. (%) 34 (31.2) 24 (22.2) Stability of anticoagulation Maximum out of range INR, mean (SD) 3.9 (1.0) 4.0 (1.0) Minimum out of range INR, mean (SD) 1.6 (0.3) 1.6 (0.3) Percent of readings above range, mean (SD) 14.0 (13.3) 14.1 (13.9) Percent of readings below range, mean (SD) 18.0 (16.9) 17.4 (16.7) Randomization stratification, No. (%) <50% INR values in range 17 (15.6) 17 (15.7) 50%-80% INR values in range 61 (56.0) 61 (56.5) >80% INR values in range 31 (28.4) 30 (27.8) Days per week of high–vitamin K foods, No. (%) <2 days 44 (40.4) 30 (27.8) 2-5 days 47 (43.1) 57 (52.8) >5 days 18 (16.5) 21 (19.4) Variability of high–vitamin K foods, No. (%) High 44 (40.4) 48 (44.4) Low 65 (59.6) 60 (55.6) Medications other than warfarin Number, mean (SD) Prescription medications 4.8 (3.4) 5.0 (3.3) Over-the-counter medications 0.6 (1.1) 0.6 (1.1) Vitamins/herbs 1.9 (1.8) 1.9 (2.2) Prescription medications, No. (%) Cardiovascular 90 (82.6) 94 (87.0) Gastrointestinal 32 (29.4) 42 (38.9) Diabetes 14 (12.8) 21 (19.4) Pulmonary 23 (21.1) 14 (12.8) Antiplatelet agents, No. (%) Aspirin 23 (21.1) 25 (23.1) Clopidogrel 2 (1.8) 5 (4.6) Prasugrel 1 (0.9) 0 (0.0) Dipyridamole/ticlopidine/ticagrelor 0 (0.0) 0 (0.0) INR = international normalized ratio; DVT = deep vein thrombosis; PE = pulmonary embolism; TTR = time within therapeutic range.
Outcome Morning Evening Difference P Value 95% CI for Difference Primary outcome Percent change in proportion of time outside target INR range, median (IQR) –11.9 (–59.5 to 65.6) –22.9 (–62.5 to 77.4) 4.4a .62 –17.6 to 27.3 Secondary outcomes Absolute change in TTR, % 2.9 (22.1) 3.0 (22.7) –0.1 .97 –6.1 to 5.9 Percent of patients with TTR >75% 56.0 54.6 1.4 .89 –12.3 to 14.9 Percent of patients with TTR <60% 22.0 22.2 –0.2 .99 –11.5 to 11.9 Maximum out-of-range INR, median (IQR) 3.6 (3.3-4.0) 3.6 (3.4-4.0) 0.0a .52 –0.2 to 0.1 Minimum out-of-range INR, median (IQR) 1.6 (1.3-1.8) 1.7 (1.5-1.8) –0.1a .15 –0.2 to 0.0 Percent of INR values above range, median (IQR) 10.0 (0-20.0) 11.1 (0-19.7) 0.0a .90 –1.8 to 1.4 Percent of INR values below range, median (IQR) 15.0 (0-28.6) 12.8 (0-22.6) 0.0a .48 –0.5 to 4.3 INR = international normalized ratio; IQR = interquartile range; TTR = time within therapeutic range.
↵a The difference in medians is by Hodges–Lehmann estimation; hence, value differs from a simple subtraction of the group medians provided.
The Article in Brief
The Effect of Warfarin Administration Time on Anticoagulation Stability (INRange): A Pragmatic Randomized Controlled Trial
Scott R. Garrison , and colleagues
Background Without supporting evidence, clinicians commonly recommend that warfarin be taken in the evening.
What This Study Found A new study shows evidence that morning versus evening dosing has insignificant bearing on how long the drug provides the most benefit for preventing adverse health events. Two hundred and seventeen adults who regularly used warfarin in the evenings were randomized to the trial, with about half switching to morning medication use for seven months. Researchers measured the effectiveness of the drug by tracking the proportion of time that patients spent outside of the range for maximum effectiveness of the drug. Therapeutic changes did not significantly differ for patients who switched to morning administration.
Implications
- The clinical research team concluded that the time of day a patient takes the medicine has no effect on the stability of warfarin�s anticoagulant effect. Patients should take warfarin whenever regular compliance would be easiest.




{kind=link}
{kind=link}