
Abstract
PURPOSE Anticholinergic burden (ACB), the cumulative effect of anticholinergic medications, is associated with adverse outcomes in older people but is less studied in middle-aged populations. Numerous scales exist to quantify ACB. The aims of this study were to quantify ACB in a large cohort using the 10 most common anticholinergic scales, to assess the association of each scale with adverse outcomes, and to assess overlap in populations identified by each scale.
METHODS We performed a longitudinal analysis of the UK Biobank community cohort (502,538 participants, baseline age: 37-73 years, median years of follow-up: 6.2). The ACB was calculated at baseline using 10 scales. Baseline data were linked to national mortality register records and hospital episode statistics. The primary outcome was a composite of all-cause mortality and major adverse cardiovascular event (MACE). Secondary outcomes were all-cause mortality, MACE, hospital admission for fall/fracture, and hospital admission with dementia/delirium. Cox proportional hazards models (hazard ratio [HR], 95% CI) quantified associations between ACB scales and outcomes adjusted for age, sex, socioeconomic status, body mass index, smoking status, alcohol use, physical activity, and morbidity count.
RESULTS Anticholinergic medication use varied from 8% to 17.6% depending on the scale used. For the primary outcome, ACB was significantly associated with all-cause mortality/MACE for each scale. The Anticholinergic Drug Scale was most strongly associated with mortality/MACE (HR = 1.12; 95% CI, 1.11-1.14 per 1-point increase in score). The ACB was significantly associated with all secondary outcomes. The Anticholinergic Effect on Cognition scale was most strongly associated with dementia/delirium (HR = 1.45; 95% CI, 1.3-1.61 per 1-point increase).
CONCLUSIONS The ACB was associated with adverse outcomes in a middle- to older-aged population. Populations identified and effect size differed between scales. Scale choice influenced the population identified as potentially requiring reduction in ACB in clinical practice or intervention trials.
INTRODUCTION
Many frequently prescribed medications for a range of medical conditions have anticholinergic properties.1 The use of multiple anticholinergic medications leads to a cumulative effect, referred to as the anticholinergic burden (ACB). The ACB is associated with adverse outcomes, including mortality, cardiovascular events, falls, and cognitive impairment, in older people.2 Several scales exist to quantify ACB3–12; however, there is no consensus regarding the optimal scale.13 It is recognized that the population identified as being at risk for adverse outcomes may vary depending on the choice of scale.14–17 The scales differ in the medications they include and the score they assign to specific medications. Scales for measuring ACB tend to classify medications into 4 categories, from no anticholinergic activity (score = 0) to high anticholinergic activity (score = 3). Scores are calculated by scoring each individual medication a person is taking and then summing them to provide an overall score. Validations of the scales vary in study design, participant age, setting, length of follow-up, and methodologic quality.13
Studies quantifying the impact of ACB have typically focused on patients aged at least 65 years, and often much older. It is not clear if findings from high-risk populations, such as nursing home residents, are relevant to the larger population of younger, less frail individuals. People aged <65 years can be affected by multiple chronic conditions (multimorbidity), multiple medications (polypharmacy), and frailty.18 Understanding how ACB affects such people is vital if the risks associated with ACB are to be mitigated at a population level.
Using data from the UK Biobank, a large community-based cohort of 502,538 participants aged 37 to 73 years, we aimed to quantify the ACB for participants using the 10 most validated anticholinergic scales, assess the association of each scale with adverse outcomes previously linked to ACB, and assess the agreement and degree of overlap of the scales in identifying ACB in the same population.
METHODS
Study Design and Participants
The UK Biobank is a community-based cohort study of 502,538 participants recruited from 2006 to 2010 in England, Scotland, and Wales. Participants completed a touchscreen questionnaire, had an interview with a study nurse, and had physical measurements (eg, height and weight) documented. All participants provided informed consent for data collection, analysis, and linkage to national mortality records and hospital episode statistics. This study was part of UK Biobank project 14151, with ethical approval from the National Health Service’s National Research Ethics Service (16/NW/0274).
Identification of Anticholinergic Scales
A total of 10 different scales quantifying ACB were identified via a systematic literature review19 (see Supplemental Appendix, http://www.AnnFamMed.org/con-tent/18/2/148/suppl/DC1). These included the Anticholinergic Drug Scale (ADS),8 Clinician-rated Anticholinergic Scale (CrAS),5 Anticholinergic Risk Scale (ARS),4 Anticholinergic Cognitive Burden (ACoB),3 Anticholinergic Activity Scale (AAS),6 revised Anticholinergic Activity Scale (AAS-r),7 Anticholinergic Loading Scale (ALS),9 Modified Anticholinergic Risk Scale (m-ARS),12 Anticholinergic Effect on Cognition (AEC),10 and Anti-cholinergic Impregnation Scale (AIS).11
Baseline Variables
All participants reported medications taken at the time of recruitment during an interview with a trained study nurse. Participants were asked to name all regular medications taken excluding short-term medications (http://biobank.ctsu.ox.ac.uk/crystal/label.cgi?id=100075). Specific data on dose, formulation, and duration were not collected. The British National Formulary was used to identify generic and branded names for each medication.20 We calculated each participant’s ACB at baseline using each of the identified scales. Weightings for each medication (0-3) were taken from the published description of each scale and then summed to provide a numeric value for each scale.
The following baseline variables were used in adjusted analyses: age, sex, socioeconomic status (Townsend score derived from participant postcodes and divided into quintiles), body mass index (BMI; categorized as <18.5, 18.5-24.9, 25.0-29.9, ≥30.0), smoking status (current, previous smoker, nonsmoker), alcohol use (never/special occasions only, 1-3 times per month, 1-4 times per week, daily/almost daily), and level of physical activity in the past 4 weeks (none, low [light household tasks only], medium [heavy house-hold tasks and/or walking for pleasure and/or other exercise], high [strenuous sports]). Participants also reported morbidities at the baseline assessment. The morbidities described in this study were from a list of 43 morbidities originally established for a large epidemiologic study in Scotland and subsequently amended for the UK Biobank.21,22 The number of morbidities reported was summed to give a morbidity count.
Outcomes
All outcomes were identified prospectively using data linkage. Baseline data were linked to national mortality records and hospital episode statistics. Hospital episode statistics outcomes were identified using International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10) diagnostic codes. The median follow-up was 74.7 months (interquartile range, 66.1-81.7 months).
Primary Outcome
The primary outcome was a composite of all-cause mortality and major adverse cardiovascular event (MACE; defined as nonfatal myocardial infarction [ICD-10 code I21], nonfatal stroke [ICD-10 codes I63, I64], or cardiovascular death [primary cause of death coded as I]).
Secondary Outcomes
Secondary outcomes included all-cause mortality, MACE, hospital admission for fall (ICD-10 codes W0, W1) or fracture (ICD-10 codes S02, S12, S22, S32, S42, S52, S62, S72, S82, S92, T05), and hospital admission with dementia or delirium (ICD-10 codes F00, F01, F02, F03, F05; analysis was limited to participants without a dementia diagnosis at baseline).
Statistical Analysis
All analyses were prespecified before inspection of the data, in keeping with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.23
Baseline Descriptive Analysis
We classified the cohort as participants taking any anticholinergic medication at baseline according to any of the 10 scales and those taking no anticholinergic medication. Age, sex, socioeconomic status, BMI, smoking status, alcohol use, physical activity level, morbidity count, and number of medications were summarized for each group.
Time-to-Event Analyses – Main Analysis
We used Cox proportional hazards models to assess the risk of each outcome for baseline values of each of the anticholinergic scales. We examined log-log survival curves to assess the proportional hazards assumption for each variable. Cause-specific models were used to account for competing risks.24 Each outcome was modeled using time to first event.
For the main analysis, hazard ratios (HRs) with 95% CIs were calculated for a 1-point increase in ACB for each scale. We excluded participants with missing data for ≥1 covariate. Each scale was modeled separately using 3 different models. Model 1 adjusted for age, sex, and socioeconomic status (n = 501,992; 0.1% missing). Model 2 adjusted as for Model 1 plus adjustment for BMI, smoking status, alcohol use, and physical activity level (n = 487,697; 3% missing). Model 3 adjusted as for Model 2 plus adjustment for morbidity count (n = 483,182; 3% missing).
Contribution of the anticholinergic scale was assessed by calculating the proportion of explainable variance explained by the scale. The predictive accuracy of Model 3 was assessed using Harrell’s C-statistic with 10-fold internal cross-validation. The C-statistic of a base model (including all covariates except the anticholinergic scale) was calculated for comparison.
Time-to-Event Analyses – Sensitivity Analyses
We performed 3 prespecified sensitivity analyses to assess potential sources of bias. The first excluded events occurring in the first 12 months of follow-up (to limit bias from reverse causality). For the second, follow-up was truncated at 24 months, with participants censored at first event or at 24 months of follow-up, whichever occurred first (to limit bias from unmeasured fluctuations in ACB over the full follow-up period). The third adjusted for all covariates of Model 2 plus hypertension, coronary heart disease, diabetes, stroke/transient ischemic attack, and heart failure at baseline. This was performed for the primary outcome (cardiovascular event or death), all-cause mortality, and MACE only.
RESULTS
Baseline Characteristics
Sociodemographic characteristics are shown in Table 1. Participants taking anticholinergic medication (score ≥1 on any scale) were significantly older than those taking no anticholinergic medication (score 0 on all scales) and more likely to be female, to be current or previous smokers, to report infrequent or no alcohol intake, and to have low physical activity. The median morbidity count was greater for those with greater ACB, as was the median number of medications.
Baseline Characteristics
Anticholinergic Burden Among UK Biobank Participants
Figure 1 shows the ACB for UK Biobank participants for each of the 10 scales. There was variation between scales in the number of people identified at all levels. The ALS identified the greatest number of people as taking anticholinergic medication (n = 88,409, 17.6%). The ARS identified the fewest (n = 40,298, 8%).
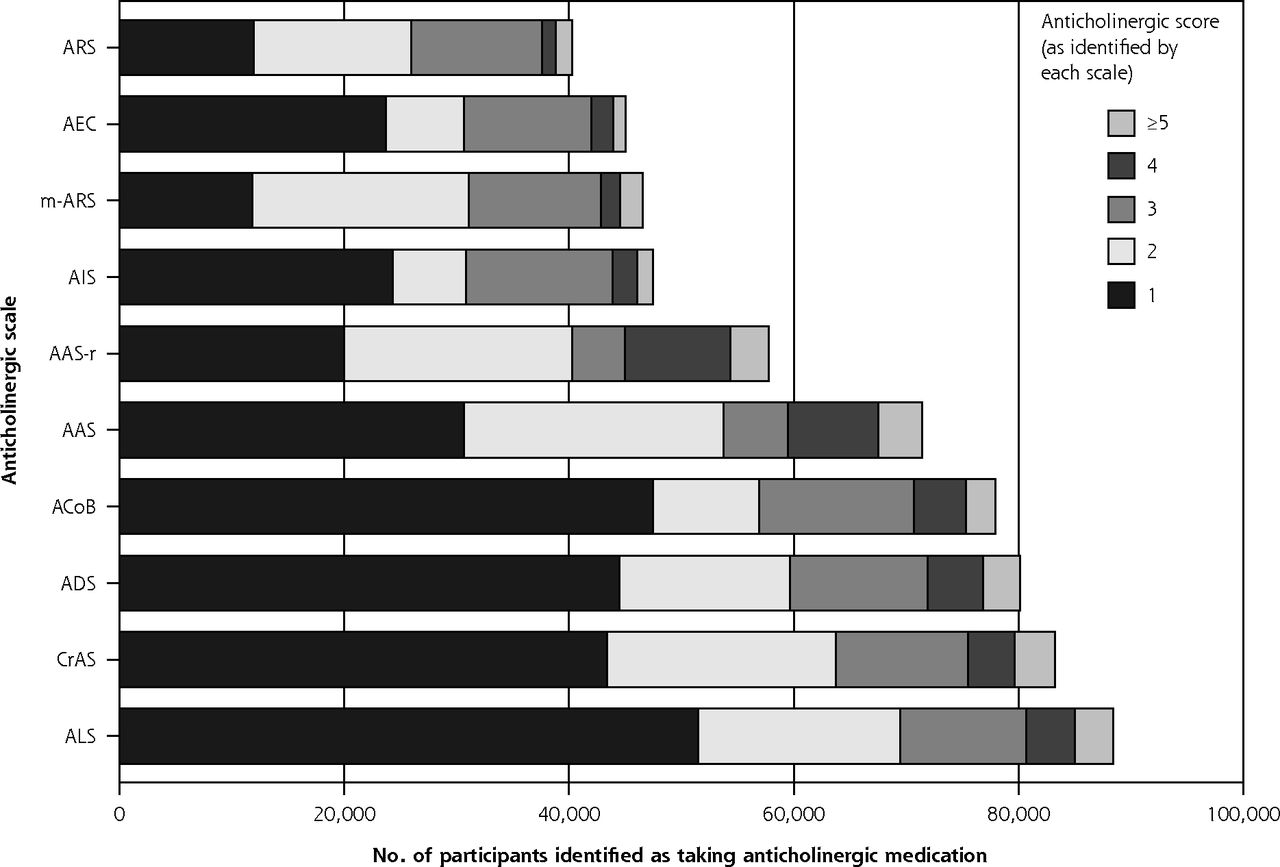
Number of participants identified as taking anticholinergic medication, by each scale.
Outcomes
Primary Outcome
With respect to the primary outcome composite of all-cause mortality and MACE, a total of 16,375 (3.3%) participants experienced nonfatal myocardial infarction, stroke, or death within the follow-up period. Greater ACB was significantly associated with a greater risk of the primary outcome for all scales (Table 2). The effect size associated with ACB was attenuated when adjusting for potential confounders (Supplemental Appendix). In the fully adjusted model (Model 3: adjusted for age, sex, socioeconomic status, BMI, smoking status, alcohol use, physical activity level, and morbidity count), HRs per 1-point increase in ACB ranged from 1.05 (95% CI, 1.03-1.07) for CrAS to 1.12 (95% CI, 1.11-1.14) for ADS.
Hazard Ratios (95% CI) for Anticholinergic Scales, by Outcome
Sensitivity analyses 1 (excluding events in the first year) and 3 (controlling for cardiovascular comorbidity) showed similar results to the main analysis. In sensitivity analysis 2 (truncated at 24 months follow-up), ARS was not significantly associated with MACE or death.
Secondary Outcomes
The HRs for the fully adjusted model (Model 3) for each of the secondary outcomes and each anticholinergic scale are shown in Table 2. Results were similar to the composite primary outcome when considering all-cause mortality and MACE separately. Each scale was significantly associated with risk of hospitalization for fall/fracture. However, the predictive accuracy was less than that for other outcomes (ie, the C-statistic was 0.626 for ADS; see Supplemental Appendix).
A total of 210 participants (not reporting dementia at baseline) had a hospital admission with dementia or delirium during follow-up. Each scale was significantly associated with increased risk (Table 2). The AEC score, which was designed to assess the risk of neurocognitive complications, showed the greatest effect size for this outcome (HR = 1.45; 95% CI, 1.3-1.61). Models including AEC had the greatest predictive accuracy for dementia/delirium compared to the base model (the C-statistic was 0.832 and 0.806 for the AEC model and base model, respectively). The HRs for ARS and AAS-r were no longer significant after excluding admissions in the first year. Truncating follow-up at 24 months, AAS-r did not show significant effect sizes (Supplemental Appendix).
Overlap of Populations Identified by Scales
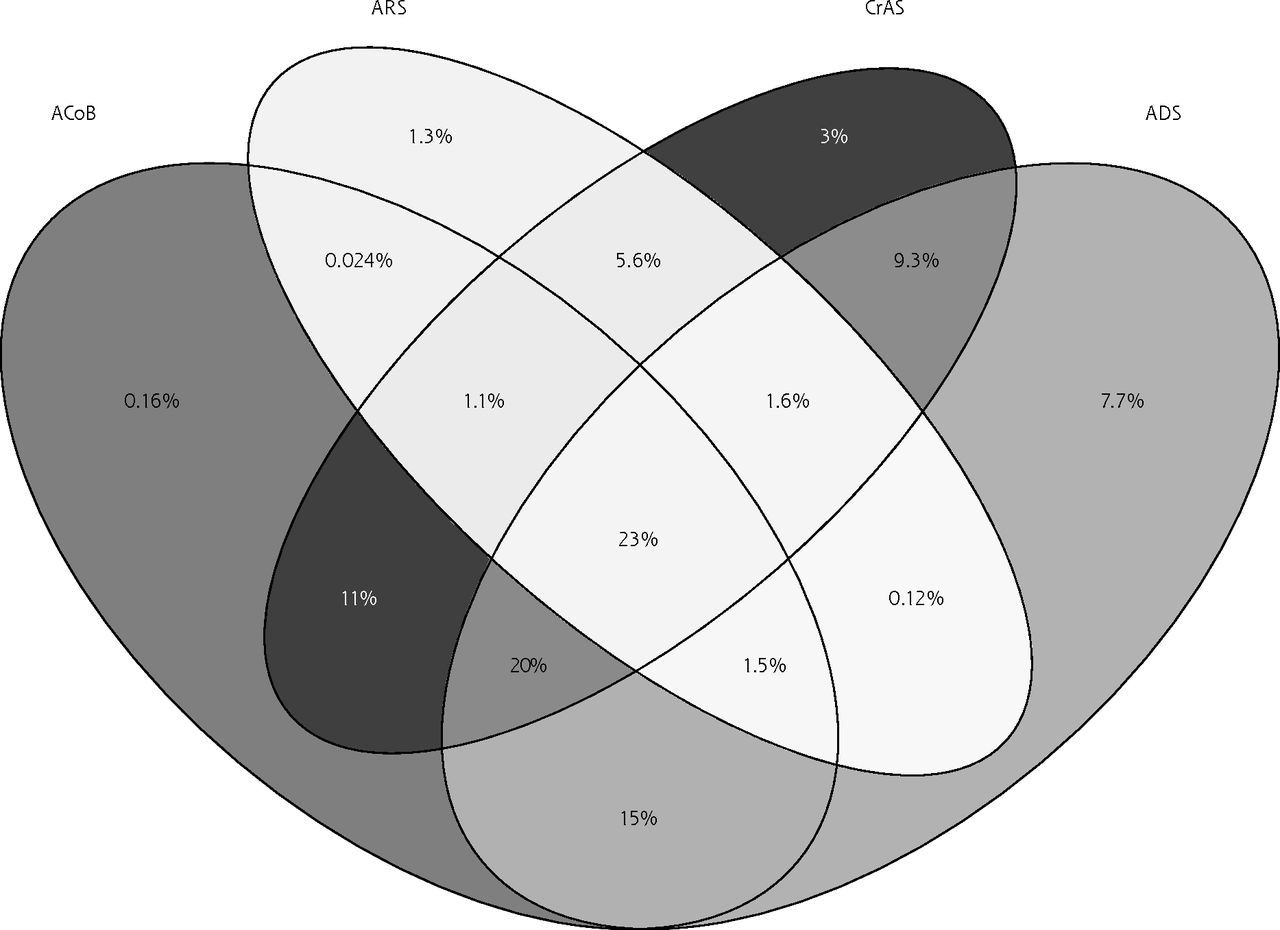
To illustrate the degree of overlap in populations identified as at risk by the different scales, participants scoring ≥1 on any of the 4 most validated scales (ADS, CrAS, ARS, ACoB)3–5,8 are shown in the Venn diagram in Figure 2. A total of 23% of these participants scored ≥1 on all 4 scales.

Venn diagram of percent of participants scoring ≥1 on any of the 4 most validated scales.
ACoB = Anticholinergic Cognitive Burden; ADS = Anticholinergic Drug Scale; ARS = Anticholinergic Risk Scale; CrAS = Clinician-rated Anticholinergic Scale.
DISCUSSION
Summary of Findings
We found considerable variability between scales in the proportion of participants identified as taking anticholinergic medication and the quantification of ACB. Regarding the 4 most validated scales,3–5,8 less than 1 in 4 of those scoring ≥1 on any scale were identified by all 4 scales. Despite this, a modest association between anticholinergic medication use and cardiovascular events, mortality, admission due to fall/fracture, or admission with dementia/delirium was seen across all scales after adjusting for multiple clinical and sociodemographic factors. Small effect sizes of this kind might still be important at the population level, especially when there is no proven intervention that halts or delays cognitive decline, one of the important adverse effects. The association between ACB and outcomes has biologic plausibility. Our results appear to be robust because associations remained consistent when corrected for potential confounders and across several prespecified sensitivity analyses. Effect sizes for AEC and AIS, which were developed to predict neurocognitive outcomes, were greater for dementia/delirium; however, CIs overlapped with the other scales. Whereas there was a consistent association between ACB and risk of adverse outcomes regardless of scale used, the populations identified as being at risk varied considerably depending on which scale was used. This has important implications if ACB is to be assessed in clinical practice and interventions designed to reduce its impact.
Strengths and Limitations
The UK Biobank cohort is larger than any previous cohort assessing ACB and includes data covering a broad range of sociodemographic and lifestyle characteristics. Follow-up via linkage to mortality registers and national hospital episode statistics limited recall bias in outcome assessment but relied on these events resulting in an inpatient episode and being accurately coded. Whereas this was unlikely to affect our identification of MACE, mortality, and fractures, other outcomes, such as falls and dementia/delirium, might lack sensitivity.25 Whereas the length of follow-up was an advantage, ACB and the extent of multimorbidity might change over time. These changes were not captured by modeling only baseline values. We conducted a sensitivity analysis truncating follow-up at 24 months to limit bias caused by unmeasured fluctuations in ACB or multimorbidity during the follow-up period. However, such an analysis might only partially mitigate potential bias from unmeasured changes over time. All medication and morbidity variables were defined by self-report, which is a potential source of bias. The UK Biobank data are not currently linked to primary care or prescribing databases that could validate medication use or diagnoses. However, participants were supported by a study nurse in providing accurate medical and drug history, and limitations of self-report would be expected to affect each scale similarly. Finally, we did not have information on dosage or duration of anticholinergic medication taken. The included scales do not specify medication dose. This meant that we were unable to include alternative scales, such as the Drug Burden Index, which includes a subscale assessing ACB.26 Duration of medication usage is also likely to be an important factor in the risk of adverse outcomes, and we were not able to measure this in the present study.
Our present findings indicate association only. A causal relation between ACB and adverse outcomes was not proven. As with any observational study, our findings were susceptible to residual confounding. Assessing adverse consequences from medication use is particularly susceptible to confounding by indication (wherein the indicating illness, rather than medication, is the causative factor in adverse outcomes).27 We attempted to limit this by adjusting for morbidity count as a measure of chronic disease burden. Results remained significant, although HRs were attenuated. We also conducted a sensitivity analysis for cardiovascular outcomes, adjusting for a range of cardiometabolic comorbidities, with similar results. However, these analyses cannot rule out residual confounding.
Context and Implications
Recommendations to reduce ACB are starting to be included in clinical guidelines (eg, for dementia or polypharmacy).28,29 Our present findings indicate that the number of people identified as being at risk will vary depending on the measures used (eg, ALS identified more than twice as many people as ARS), and different scales will identify different people. The ARS and ACoB had the greatest effect size for the primary outcome, although point estimates for AEC and AIS were greater for neurocognitive outcomes. Rather than identifying an optimal scale, our findings highlight pitfalls and implications that should be considered when attempting to identify and reduce ACB. The simplicity and usability of scales is also relevant to clinical use. The importance of classes of medications, compared to high or low scores, should also be explored.30
There is a need to explore the effect of reducing ACB at a population level, given that the focus of existing interventions is limited to frail older people.31,32 The average age of UK Biobank participants is younger than previous cohorts validating these scales (mean ages generally >70 years, many conducted in nursing homes or palliative care settings). Participants in the UK Biobank are more affluent and less multi-morbid than the UK average.33 Whereas this limits accurate inference regarding the prevalence of ACB in the general population, relations between exposures and outcomes remain valid. However, the effect sizes observed in the present study were modest, and the effect of reducing ACB at an individual level is not clear. Furthermore, residual confounding, particularly confounding by indication, cannot be excluded as an explanation for the associations observed. Our present finding that ACB is associated with various adverse outcomes, in a younger and relatively healthier population than previously studied, highlights that there may be value in interventions to reduce ACB at a population level because the absolute numbers of people potentially at risk are high. Developing such an intervention would require investigation of barriers and facilitators to optimizing anticholinergic prescribing at the patient, professional, and organizational levels. However, there is also a need to identify and understand what factors increase susceptibility to adverse effects of ACB (eg, older age, frailty, etc).
Conclusions
In a middle- to older-aged population of >500,000 people, we found levels of anticholinergic prescribing ranging from 8% to 17.6% depending on the scale used. There was an association of anticholinergic medication use with mortality, cardiovascular events, and admissions for falls/fractures and dementia/delirium, irrespective of scale used. This was true after adjusting for sociodemographic factors and morbidities. However, different populations will be identified depending on the scale used. These findings should inform their use in clinical practice and in decision making in future intervention trials.
Footnotes
Conflicts of interest: authors report none.
To read or post commentaries in response to this article, see it online at http://www.AnnFamMed.org/content/18/2/148.
Author contributions: Concept and design: P.H., T.J.Q., P.K.M., K.I.G., R.L., R.L.S., F.S.M.; acquisition, analysis, or interpretation of data: P.H., K.I.G., B.D.J., B.I.N., D.L., R.L.S., P.K.M., F.S.M.; drafting of the manuscript: P.H., F.S.M.; critical revision of the manuscript: P.H., T.J.Q., P.K.M., K.I.G., B.D.J., B.I.N., R.L., R.L.S., S.R.N., F.S.M.; statistical analysis: P.H., D.L.; supervision: T.J.Q., K.I.G., P.K.M., F.S.M.
Funding support: K.I.G. was funded by a Stroke Association HRH Princess Margaret Clinical Lectureship Award 2017/01. T.J.Q. was funded by a Joint Stroke Association and Chief Scientist Office Senior Clinical Lectureship. B.D.J. was funded by an NHS Research for Scotland (NRS) Career Research Fellowship.
Prior presentation: An earlier version of this work (oral presentation) was presented at the North American Primary Care Research Group annual meeting; November 2018; Chicago, Illinois.
Supplemental materials: Available at http://www.AnnFamMed.org/content/18/2/148/suppl/DC1/.
- Received for publication April 18, 2019.
- Revision received July 24, 2019.
- Accepted for publication August 16, 2019.
- © 2020 Annals of Family Medicine, Inc.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A qualitative exploration of barriers to efficient and effective Structured Medication Reviews in Primary Care: Findings from the DynAIRx study
- Association between recently raised anticholinergic burden and risk of acute cardiovascular events: nationwide case-case-time-control study
- Managing drugs with anticholinergic activity
- Anticholinergic burden in middle and older age is associated with lower cognitive function, but not with brain atrophy
- Association between anticholinergic burden and dementia in UK Biobank
- Increase in anticholinergic burden in the UK from 1990 to 2015: a UK Biobank study
- Variation in VKORC1 is associated with vascular dementia