
Article Figures & Data
Figures
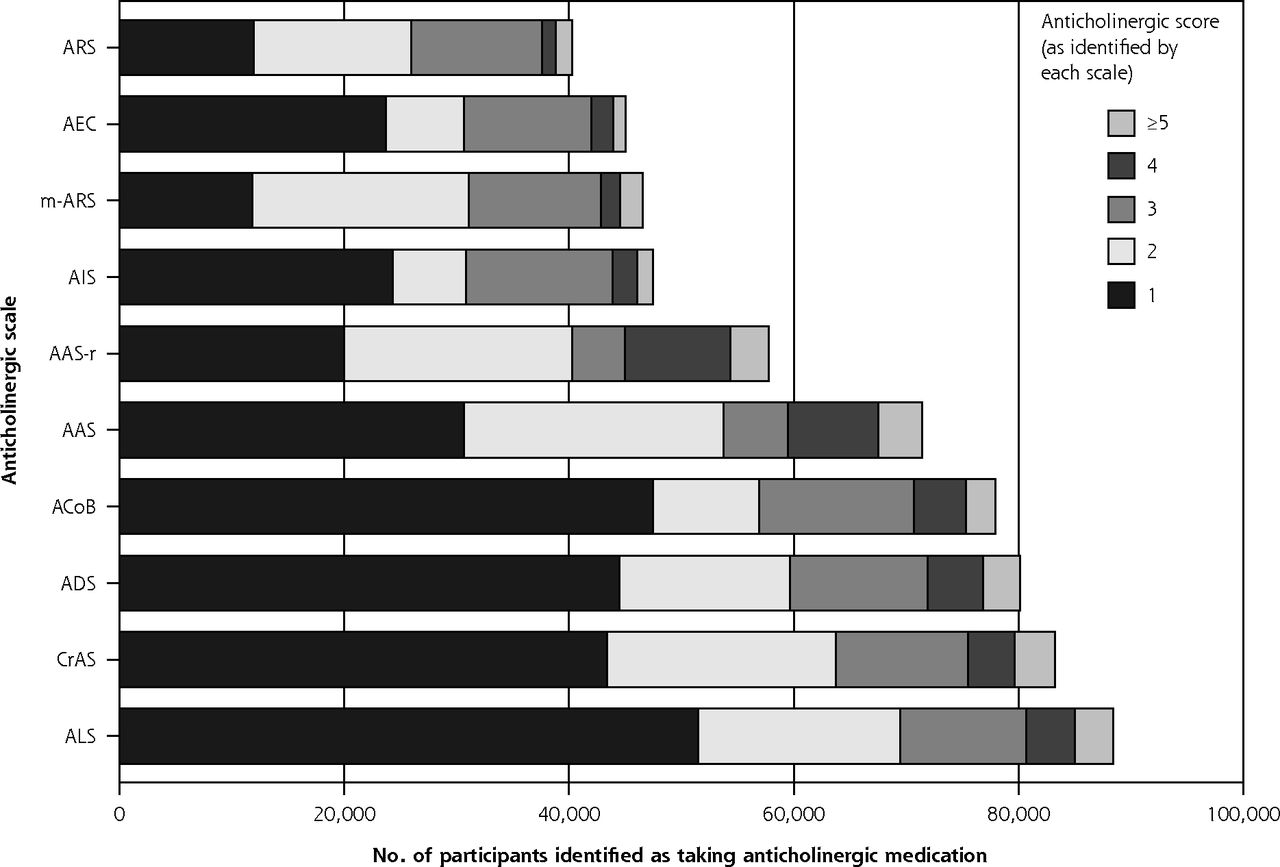
- Figure 1
Number of participants identified as taking anticholinergic medication, by each scale.
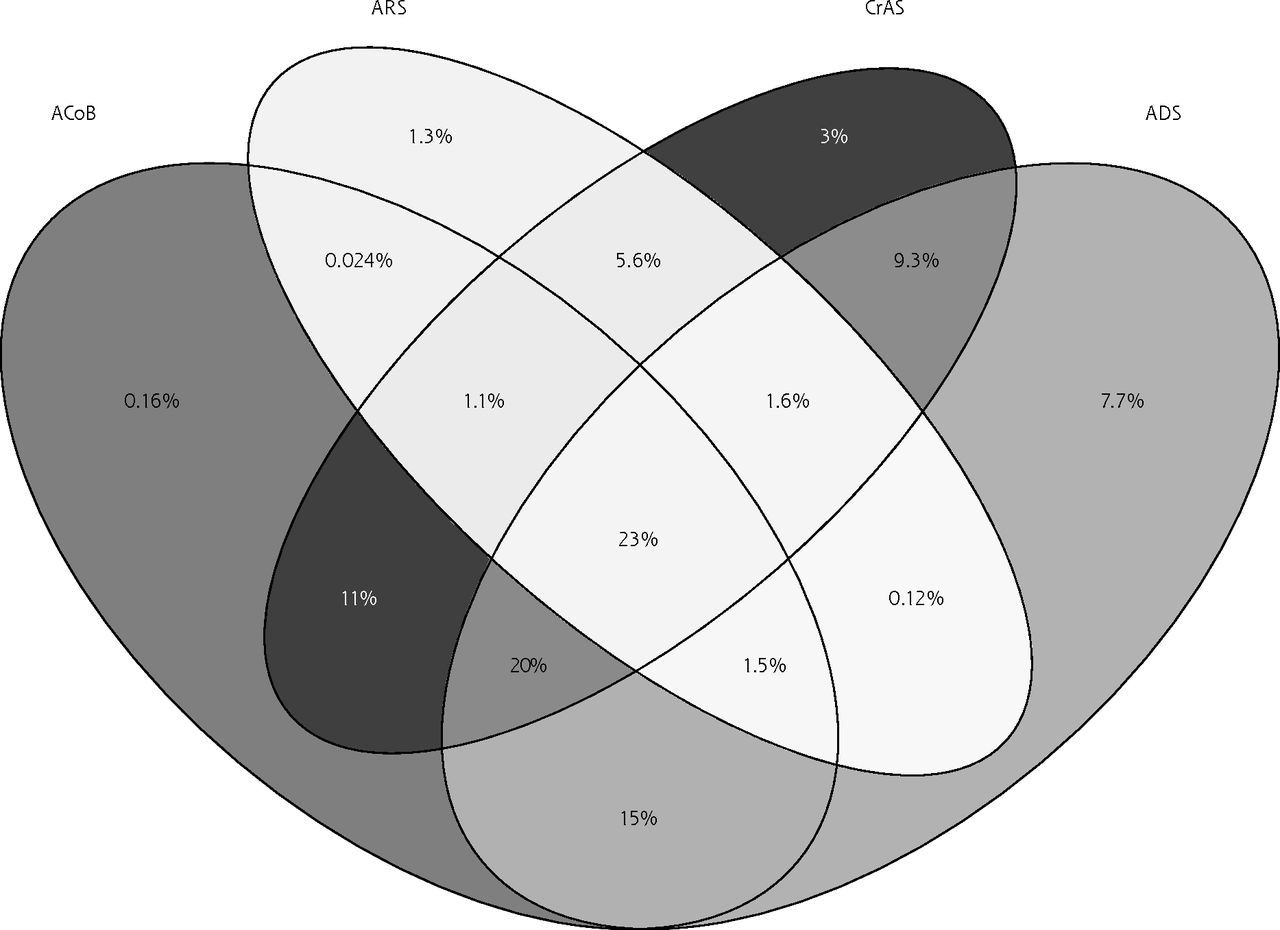
- Figure 2
Venn diagram of percent of participants scoring ≥1 on any of the 4 most validated scales.
ACoB = Anticholinergic Cognitive Burden; ADS = Anticholinergic Drug Scale; ARS = Anticholinergic Risk Scale; CrAS = Clinician-rated Anticholinergic Scale.

Tables
Variable Score = 0 on All Scales N = 367,319 Score ≥1 on Any Scale N = 135,321 Age, y, median (IQR) 57 (49-62) 60 (53-65) Missing 0 0 Sex, No. (%) Female 198,346 (54) 75,120 (55.5) Male 168,973 (46) 60,201 (44.5) Missing 0 0 Townsend score quintile (socioeconomic status), No. (%) 1 (Least deprived) 77,293 (21.1) 23,394 (17.3) 2 75,738 (20.6) 24,381 (18.0) 3 74,334 (20.3) 26,078 (19.3) 4 72,916 (19.9) 27,479 (20.3) 5 (Most deprived) 66,602 (18.2) 33,798 (25.0) Missing 436 191 BMI category, No. (%) <18.5 1,975 (0.5) 651 (0.5) 18.5-24.9 127,580 (35) 29,887 (22.5) 25.0-29.9 159,715 (43.8) 54,552 (41.1) ≥30 74,969 (20.6) 47,491 (35.8) Missing 3,080 2,740 Smoking status, No. (%) Never 208,977 (57.2) 64,624 (48.1) Previous 120,154 (32.9) 52,944 (39.4) Current 36,210 (9.9) 16,779 (12.5) Missing 1,978 974 Alcohol use, No. (%) Never/special occasions 61,230 (16.7) 37,460 (27.8) 1-3 times per month 39,987 (10.9) 15,886 (11.0) 1-4 times per week 187,445 (51.2) 57,339 (42.5) Daily/almost daily 77,572 (21.2) 24,218 (18.0) Missing 1,085 418 Physical activity level, No. (%) High 43,279 (11.9) 6,798 (5.1) Medium 290,383 (80.0) 103,221 (77.9) Low 11,330 (3.1) 7,613 (5.7) None 17,983 (5.0) 14,875 (11.2) Missing 4,344 2,814 Morbidity count, median (IQR) 1 (0-1) 2 (1-3) Missing 1,173 672 Number of regular medications, median (IQR) 1 (0-2) 4 (3-7) Missing 862 0 BMI = body mass index; IQR = interquartile range.
Note: Percentages were calculated excluding missing values.
Scale MACE/Mortality All-Cause Mortality MACE Fall or Fracture Dementia/Delirium CrAS 1.05 (1.03-1.07) 1.05 (1.04-1.07) 1.03 (1-1.06) 1.09 (1.06-1.11) 1.23 (1.1-1.36) ARS 1.05 (1.03-1.08) 1.06 (1.04-1.08) 1.01 (0.97-1.05) 1.06 (1.03-1.1) 1.23 (1.07-1.4) AAS-r 1.06 (1.04-1.08) 1.07 (1.05-1.08) 1.07 (1.04-1.09) 1.09 (1.06-1.12) 1.14 (1.02-1.28) ALS 1.06 (1.04-1.08) 1.07 (1.05-1.08) 1.04 (1.01-1.07) 1.1 (1.07-1.13) 1.26 (1.14-1.41) AAS 1.06 (1.05-1.08) 1.07 (1.05-1.09) 1.07 (1.05-1.1) 1.09 (1.06-1.12) 1.24 (1.11-1.37) AEC 1.07 (1.05-1.1) 1.08 (1.06-1.1) 1.04 (1-1.08) 1.12 (1.09-1.16) 1.45 (1.3-1.61) m-ARS 1.07 (1.06-1.09) 1.08 (1.06-1.1) 1.02 (0.99-1.06) 1.08 (1.05-1.12) 1.27 (1.13-1.43) AIS 1.08 (1.06-1.1) 1.09 (1.07-1.11) 1.04 (1.01-1.08) 1.14 (1.1-1.17) 1.38 (1.24-1.54) ACoB 1.12 (1.1-1.14) 1.13 (1.11-1.15) 1.17 (1.14-1.2) 1.11 (1.08-1.14) 1.26 (1.14-1.4) ADS 1.12 (1.11-1.14) 1.13 (1.12-1.15) 1.15 (1.12-1.17) 1.13 (1.1-1.16) 1.29 (1.16-1.42) AAS = Anticholinergic Activity Scale; AAS-r = revised Anticholinergic Activity Scale; ACoB = Anticholinergic Cognitive Burden; ADS = Anticholinergic Drug Scale;
AEC = Anticholinergic Effect on Cognition; AIS = Anticholinergic Impregnation Scale; ALS = Anticholinergic Loading Scale; ARS = Anticholinergic Risk Scale; CrAS = Clinician-rated Anticholinergic Scale; MACE = major adverse cardiovascular event; m-ARS = Modified Anticholinergic Risk Scale.
Results from Model 3: Adjusted for age, sex, socioeconomic status, body mass index, smoking status, alcohol use, physical activity level, and morbidity count.
Supplemental Appendix
Supplemental Appendix
Files in this Data Supplement:
- Supplemental data: Appendix - PDF file
The Article in Brief
Assessing Risks of Polypharmacy Involving Medications With Anticholinergic Properties
Frances S. Mair , and colleagues
Background Many common prescription medications for urinary problems and muscle spasms, as well over- the-counter medications for cold, cough and allergies, share an anticholinergic property. The use of multiple medications in this class can lead to negative cumulative effects referred to as anticholinergic burden. ACB is known to increase the risk for future adverse events like falls, dementia, heart attack, stroke, and death. Guidelines recommend against using anticholinergic medications for geriatric patients, but little is known about their effect on middle-aged patients. A variety of assessment scales are available for doctors and researchers to calculate a patient's risk of ACB. A study of more than 500,000 middle-aged adults, aged 37 to 73 years in the United Kingdom, compared 10 of those scales to assess their accuracy in predicting risk for future adverse events.
What This Study Found Researchers found that all 10 ACB scales identified individuals at higher risk for heart attack, stroke and death, after adjusting for sociodemographic and baseline health factors. Each scale also had significant predictive accuracy for falls and dementia. While the study showed consistent association between ACB and adverse outcomes, regardless of which scale was used, the populations identified as being at risk varied considerably depending on which scale was used. Less than one in four people detected to be at risk by one scale were also detected by the other three most frequently used scales.
Implications
- This variation across scales has implications for clinical practice and research interventions to target anticholinergic burden.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- A qualitative exploration of barriers to efficient and effective Structured Medication Reviews in Primary Care: Findings from the DynAIRx study
- Association between recently raised anticholinergic burden and risk of acute cardiovascular events: nationwide case-case-time-control study
- Managing drugs with anticholinergic activity
- Anticholinergic burden in middle and older age is associated with lower cognitive function, but not with brain atrophy
- Association between anticholinergic burden and dementia in UK Biobank
- Increase in anticholinergic burden in the UK from 1990 to 2015: a UK Biobank study
- Variation in VKORC1 is associated with vascular dementia